
Abstract
Background:
Postoperative outcomes of portoenterostomy (PE) and redo-PE were evaluated using selected biochemical markers (SBM) and biochemical status categories (BSC).
Methods:
Subjects were 70 consecutive PE performed for biliary atresia. SBM were aspartate aminotransferase (AST)/alanine aminotransferase (ALT), cholinesterase (ChE), and platelet count (PLT) assessed at 1, 2, 3, 6, and 12 months, and thence, annually for a maximum of 10 years. BSC were as follows: all SBM normal (N-SBM), normal AST/ALT (N-SLT), normal ChE (N-ChE), normal PC (N-PLT), all abnormal (A-SBM), abnormal AST/ALT (A-SLT), abnormal ChE (A-ChE), and abnormal PC (A-PLT). Subjects achieving jaundice clearance (JC) and surviving with native livers (SNL) also had gamma glutamyl transpeptidase assessed. Redo-PE indicated for failed PE was assessed postoperatively using the same SBM/BSC protocol.
Results:
PE were laparoscopic (LPE; n = 40) or open (OPE; n = 30). Mean age/weight at PE and duration of follow-up were similar. For JC, LPE = 34/40 (85.0%) and OPE = 22/30 (73.3%); P = .23. For SNL, LPE = 29/40 (72.5%) and OPE = 16/30 (53.3%); P = .10. LPE and OPE were similar for SBM/BSC, except for a single significant increase in ALT in OPE at 6 months. Redo-PE was performed 17–180 days (mean 67.1 days) after primary PE. AST was significantly increased at the last preredo assessment 3 months after primary PE; P < .05. After redo, AST decreased and SBM/BSC results were equivalent to nonredo subjects.
Conclusion:
Postoperative biochemical data for all PE cases were comparable; redo-PE would appear to be viable for restoring SBM, and AST could be valuable as a single marker of deterioration in redo cases.
Introduction
Portoenterostomy (PE) improved the prognosis of biliary atresia (BA) immensely when it was first introduced 1 because BA requires surgical intervention, but cannot be cured by surgery. Laparoscopic PE (LPE), first reported by Esteves et al in 20022 and developed to apply the advantages of minimally invasive surgery (MIS) to open PE (OPE),3–7 was subsequently attempted by many pediatric surgeons worldwide3,8 and despite the high initial expectations, the outcome of LPE was reported to be worse than OPE with concerns about safety and surgical stress9–12 leading to the International Pediatric Endosurgery Group abandoning LPE as a recommended procedure in 2007 13 because of high failure rates and poor outcomes. In 2011, similar results were reported by a prospective study in Europe conducted specifically to justify LPE as a valid treatment for BA, 11 and LPE ceased to be performed in Europe thereafter.
Pediatric hepatobiliary surgeons face a dilemma because astute caregivers are aware of the benefits of MIS; less intraoperative blood loss, faster recovery times, smaller wounds, less requirement for postoperative analgesia, and technically, LPE interferes with the liver hemodynamics less because intraoperative mobilization of the liver is not required, accuracy of anastomosis is similar to OPE because of magnification, and there are also reports of fewer adhesions 14 postoperatively that could facilitate surgical intervention should further surgery or liver transplantation (LTx) be required in the future. 15 In fact, more recent reports appear to favor LPE.5,7
In 2016, the authors' colleagues published a report comparing postoperative changes in selected biochemical markers (SBM) after PE between LPE and OPE in an effort to improve understanding of the clinical impact of LPE. SBM used were aspartate aminotransferase (AST) and alanine aminotransferase (ALT) as indicators of liver cell damage, 16 total bilirubin (T-Bil), and platelet count (PLT) as an indicator of hypersplenism 17 secondary to the histopathologic progression of BA. Changes observed in SBM were similar for LPE and OPE. 18 Data were obtained prospectively from blood biochemistry assessed at the last outpatient clinic attendance made by each postoperative BA subject, and so, clinical status was assessed at a single point in time that varied between subjects.
The current study sought to improve on the earlier study by focusing on postoperative BA patients surviving with native livers (SNL) using more SBM (cholinesterase [ChE] as an indicator of liver synthetic function 19 and gamma glutamyl transpeptidase (γ-GTP) as an indicator of liver cell and bile duct epithelial damage and cholestasis 20 ), and making assessments at multiple predetermined times that were fixed and identical for all subjects to compare LPE and OPE more thoroughly and objectively.
Subject data were also analyzed using biochemical status categories (BSC) to further assess postoperative outcome from specific perspectives. While this approach was considered reasonable for comparing LPE and OPE, subjects who began to deteriorate requiring redo surgery, LTx, or at risk for death also require active intervention, and an assessment of the biochemical status of redo-PE cases was included to demonstrate the value of SBM and BSC for assessing postoperative PE cases and the value of redo-PE for treating PE cases who fail to achieve jaundice clearance (JC). While the success of redo-PE has been reported,21,22 redo-PE cases have not been assessed previously using SBM and BSC.
The aim of this study was twofold: to use SBM and BSC for comparing LPE with OPE and to use SBM and BSC for comparing the outcome of redo-PE cases with nonredo cases.
Materials and Methods
Subjects enrolled in this study were 70 consecutive BA patients treated by either LPE or OPE between 2009 and 2021. The type of procedure performed was indicated by clinical status and weight at the time of planning PE; the choice of procedure was made by the operating surgical team. Surgical techniques for OPE and LPE may be found elsewhere. 23 All PE were performed by a team of surgeons who trained and worked together at Juntendo University School of Medicine and all patient management was strictly protocolized.
For comparing LPE and OPE biochemically, subjects were classified according to the post-PE outcome into the following: Group 1: all subjects who achieved JC (T-Bil ≤1.2 mg/dL) at least once, SNL, irrespective of the type of PE (primary or redo) or technique (LPE, OPE, redo-LPE, redo-OPE); Group 2: subjects who achieved JC initially but required redo-PE or LTx; and Group 3: subjects who did not achieve JC and required redo-PE, LTx, or died.
SBM (AST, ALT, γ-GTP, ChE, and PLT for Group 1, and AST, ALT, ChE, and PLT for Groups 2 and 3) were used to compare LPE with OPE and redo-PE cases with nonredo cases. Definitions of “normal” used in this study obtained from the Department of Clinical Laboratory Medicine at Juntendo University School of Medicine were as follows: T-Bil ≤1.2 mg/dL, AST ≤37 IU/L, ALT ≤43 IU/L, γ-GTP ≤75 IU/L, ChE ≥178 IU/L, and PLT ≥153 × 109/L. All subjects were also classified into eight BSC as follows: all SBM normal (N-SBM), normal AST/ALT (N-SLT), normal ChE (N-ChE), normal PC (N-PLT), all SBM abnormal (A-SBM), abnormal AST/ALT (A-SLT), abnormal ChE (A-ChE), and abnormal PC (A-PLT).
All data were obtained retrospectively from outpatient clinic records. Commonly assessed demographic criteria (age/weight at PE, types of BA) were compared. SBM and BSC were assessed according to a standard protocol (1, 2, 3, 6, and 12 months) in each group, and thence, annually for 10 years in Group 1, until redo-PE or LTx in Group 2, and until redo-PE, LTx, or death in Group 3. Subjects who required redo-PE were assessed for SBM and BSC postoperatively, according to the standard protocol. Numbers of subjects at each scheduled assessment decreased over time because newer subjects had a shorter duration of follow-up and subjects who had LTx or died were excluded. No subject was lost to follow-up. Other criteria associated with operative safety and outcome such as operative time, blood loss, and duration of hospitalization were considered beyond the scope of this study.
Statistical analysis
The Student's t test and chi-squared test were used for statistical analysis. A P value <.05 was considered to be statistically significant.
Ethics
Informed consent for the PE procedure chosen to be performed by the senior operating surgeon was obtained from caregivers for each subject in this study after careful explanation of the procedure and risks by the senior operating surgeon. The institutional review board number for this study granted by the Ethics Committee at Juntendo University School of Medicine for complying with the Helsinki Declaration of 1975 (revised 1983) was 20-307.
Results
PE (n = 70) was LPE = 40 and OPE = 30. Types of BA were as follows: LPE: type III: n = 33, type II: n = 5, type I: n = 2; OPE: type III: n = 24, type II: n = 2, type I: n = 4; P = .37; according to being syndromic: LPE: nonsyndromic: n = 38, syndromic: n = 2; OPE: nonsyndromic: n = 26, syndromic: n = 4; P = .22; according to being cystic: LPE: noncystic: n = 38, cystic: n = 2; OPE: noncystic: n = 26, cystic: n = 4; P = .22.
Mean age at primary PE was 65.5 days (range: 21–123 days) for LPE and 72.6 days (range: 29–149 days) for OPE; P = .31. Mean weight at primary PE was 4.3 kg (range: 3.2–7.1 kg) for LPE and 4.7 kg (range: 2.5–7.0 kg) for OPE; P = .16. JC was achieved in 34/40 (85.0%) taking a mean of 54.8 days (range: 22–110 days) in LPE and 22/30 (73.3%) taking a mean of 45.0 days (range: 14–134 days) in OPE; P = .23 and .21, respectively. SNL was 29/40 (72.5%) in LPE and 16/30 (53.3%) in OPE; P = .10 (see Table 1).
Summary of Data According to Types of Portoenterostomy
Postoperative T-Bil ≤1.2 mg/dL, n: no. of cases.
BA, biliary atresia; LPE, laparoscopic portoenterostomy; OPE, open portoenterostomy; T-Bil, total bilirubin.
The number of subjects in each group was as follows: Group 1 (n = 45: LPE = 29, OPE = 16; redo-PE = 6, nonredo = 39), Group 2 (n = 10: LPE = 4, OPE = 6; redo-PE = 2, nonredo = 8), and Group 3 (n = 15: LPE = 7, OPE = 8; redo-PE = 3, nonredo = 12). Mean durations of postoperative follow-up were as follows: Group 1 = 5.6 years (range: 0.3–12.9 years), Group 2 = 1.6 years (range: 0.3–4.9 years), and Group 3 = 0.6 years (range: 0.1–0.8 years). Differences in mean duration of postoperative follow-up between groups were significant; P < .0001, respectively. Mean durations of postoperative follow-up for LPE were 5.4 years (range: 0.1–12.3 years) and for OPE were 5.4 years (range: 0.8–12.9 years); P = .94.
The number of subjects at each assessment for 10 years in Group 1 (n = 45) was as follows: 1 month (n = 45), 2 months (n = 45), 3 months (n = 45), 6 months (n = 43), 12 months (n = 37), 2 years (n = 34), 3 years (n = 31), 4 years (n = 28), 5 years (n = 27), 6 years (n = 27), 7 years (n = 19), 8 years (n = 12), 9 years (n = 9), and 10 years (n = 6). The number of subjects at each assessment until redo-PE or LTx in Group 2 (n = 10) was as follows: 1 month (n = 10), 2 months (n = 10), 3 months (n = 10), 6 months (n = 8), 12 months (n = 5), and 2 years (n = 3). The 3-year assessment could not be performed in Group 2. The number of subjects at each assessment until redo-PE, LTx, or death in group 3 (n = 15) was as follows: 1 month (n = 15), 2 months (n = 14), 3 months (n = 12), and 6 months (n = 9). The 12-month assessment could not be performed in Group 3.
Figure 1 shows differences in SBM data according to the PE technique. AST, ALT, and γ-GTP results were higher and ChE and PLT results were lower for LPE, but differences were not significant throughout the entire study in Group 1; there was a significant improvement in ALT 6 months postoperatively in OPE that was transient (P < .05). The range in differences between the LPE and OPE data decreased with a longer follow-up, but all differences were not significant (data not shown).
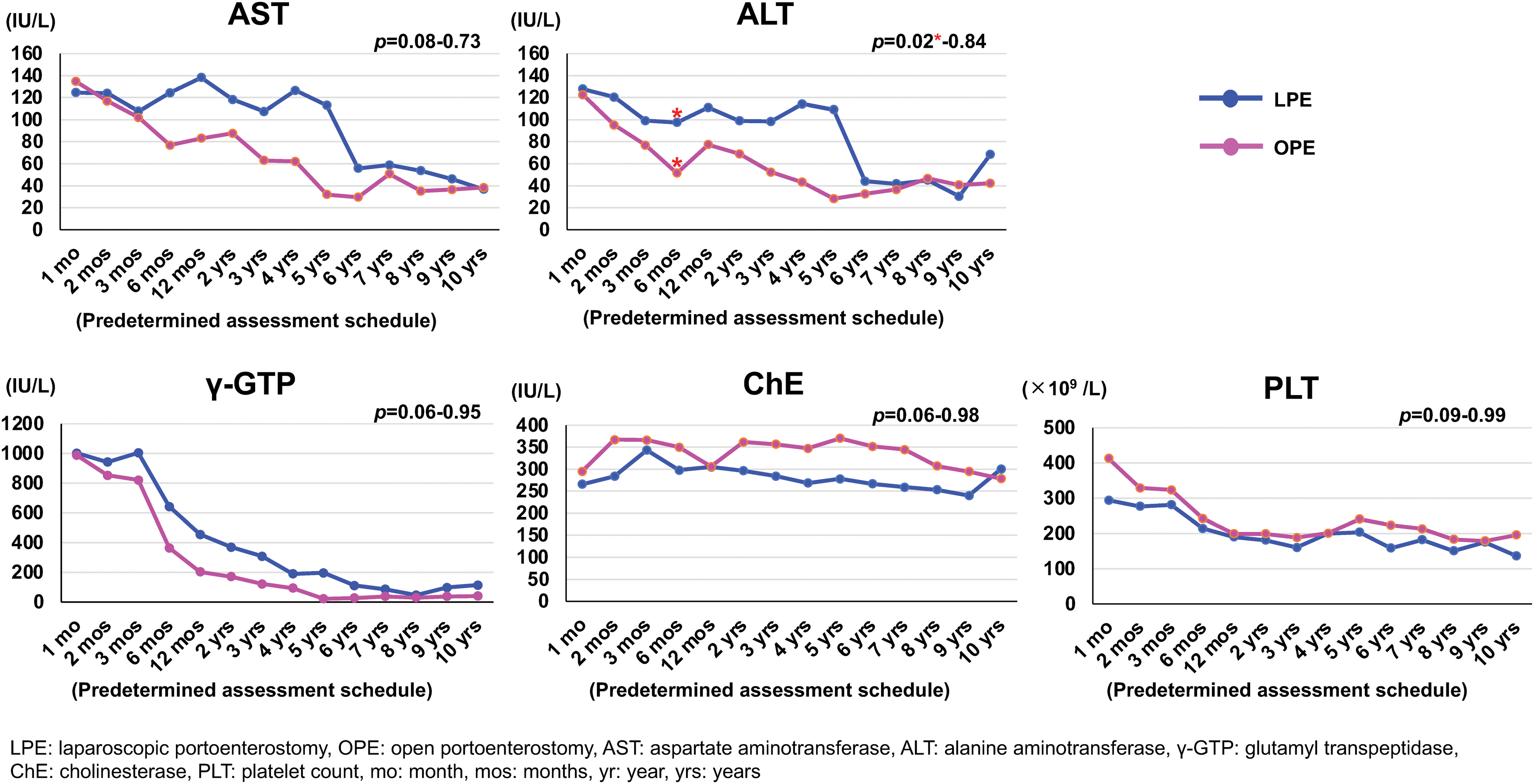
Trends in AST, ALT, γ-GTP, ChE, and PLT in Group 1 expressed according to surgical technique (LPE/OPE). OPE subjects appear to do better; there was a transient statistically significant difference for ALT at 6 months (P < .05); otherwise, there were no significant differences in SBM between LPE and OPE (ranges in P for completed protocol assessments were .06–.99). γ-GTP, gamma glutamyl transpeptidase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ChE, cholinesterase; LPE, laparoscopic portoenterostomy; OPE, open portoenterostomy; PLT, platelet count. Color images are available online.
For BSC, there were no significant differences between LPE and OPE in Group 1 (range in P for completed protocol assessments was .20–.88), Group 2 (range in P for completed protocol assessments was .20–.75), and Group 3 (range in P for completed protocol assessments was .35–.95). For Group 1, only BSC data for 1 month, 3 months, 6 months, 12 months, 2 years, 4 years, 6 years, 8 years, and 10 years are presented in Figure 2, results for other assessments were similar. BSC distributions for LPE and OPE completed in Group 2 (n = 10) from 1 month (n = 10) to 2 years (n = 3) and completed in Group 3 (n = 15) from 1 month (n = 15) to 6 months (n = 9) were similar (ranges in P for completed protocol assessments were .20–.75 and .35–.95, respectively) (see Figs. 2–4).
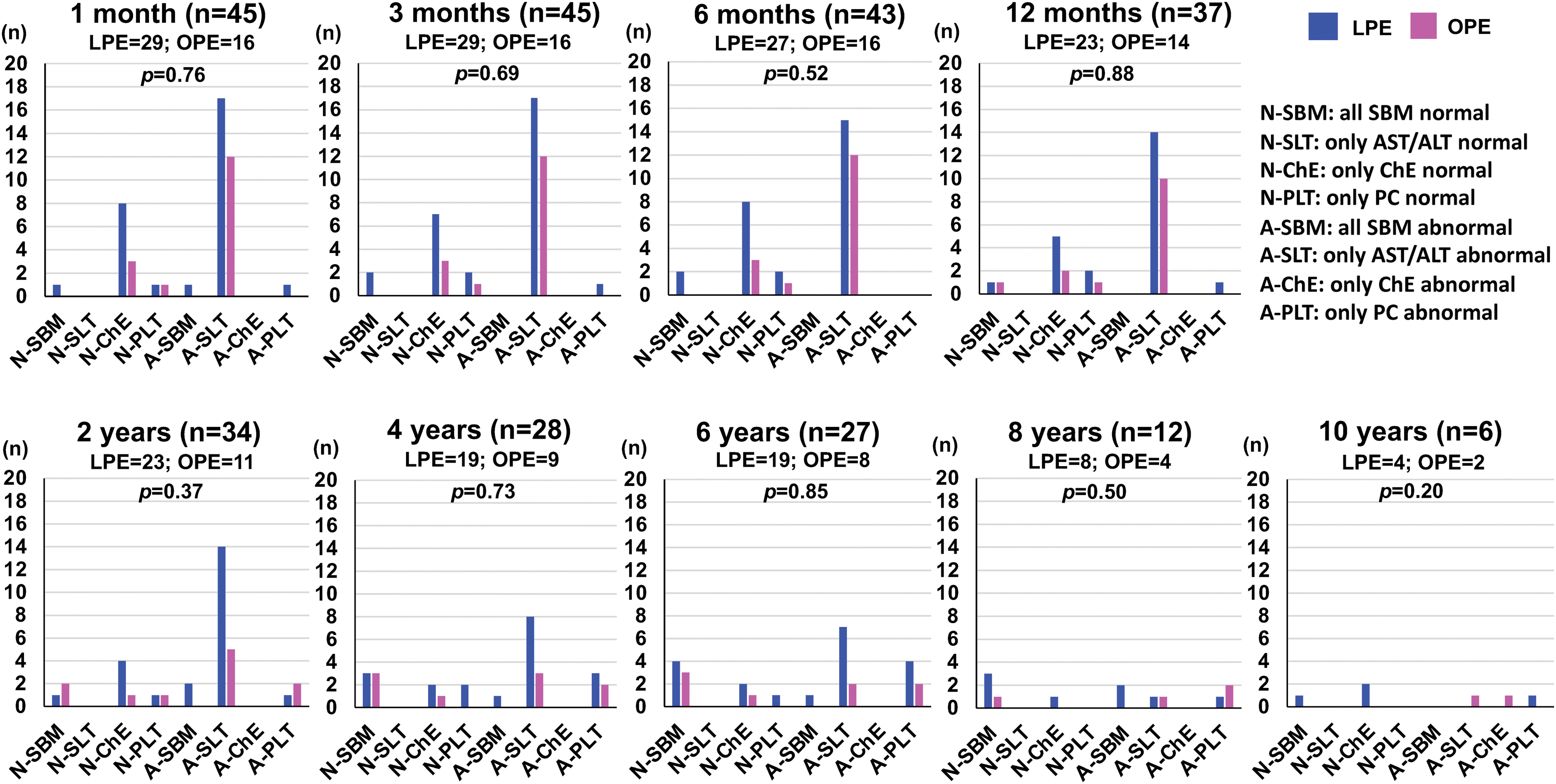
BSC for Group 1. Subjects in Group 1 completed the full assessment protocol. BSC distributions followed similar patterns; A-SLT was the most common BSC in both LPE and OPE and there were no significant differences between LPE and OPE (ranges in P for completed protocol assessments were .20–.88). A-SLT, abnormal aspartate aminotransferase/alanine aminotransferase; BSC, biochemical status categories; LPE, laparoscopic portoenterostomy; OPE, open portoenterostomy. Color images are available online.
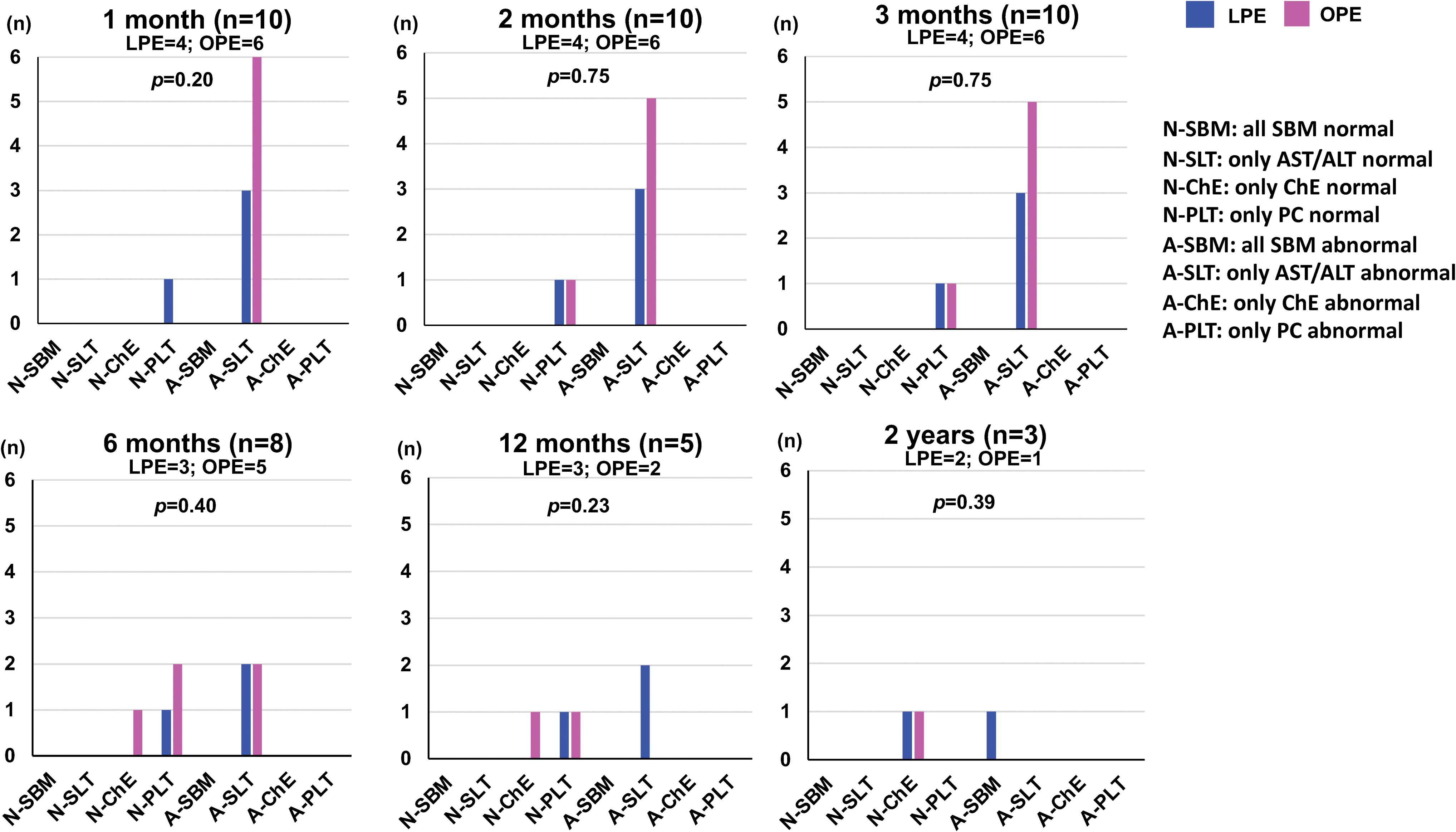
BSC for Group 2. Subjects in Group 2 were only assessed for 2 years because of redo-PE, LTx, or death. BSC distributions followed similar patterns with no significant differences between LPE and OPE (ranges in P for completed protocol assessments were .20–.75). BSC, biochemical status categories; LPE, laparoscopic portoenterostomy; LTx, liver transplantation; PE, portoenterostomy; OPE, open portoenterostomy. Color images are available online.

BSC for Group 3. Subjects in Group 3 were only assessed for 6 months because of redo-PE, LTx, or death. BSC distributions followed similar patterns with no significant differences between LPE and OPE (ranges in P for completed protocol assessments were .35–.95). BSC, biochemical status categories; LPE, laparoscopic portoenterostomy; LTx, liver transplantation; OPE, open portoenterostomy. Color images are available online.
Mid- to long-term changes in N-SBM in Group 1 for LPE were as follows: 5 years (n = 3), 6 years (n = 4; +1 for a new N-SBM case), 7 years (n = 3; −1 for abnormal results), 8 years (n = 3; unchanged), 9 years (n = 2; −1 for abnormal results), and 10 years (n = 1; −1 for abnormal results); and for OPE were 5 years (n = 3), 6 years (n = 3; unchanged), 7 years (n = 1; −2 for abnormal results), 8 years (n = 1; unchanged), 9 years (n = 1; unchanged), and 10 years (n = 0; −1 for abnormal results) (see Fig. 2).
During the study period, 11 redo-PE (5 by LPE and 6 by OPE) were performed. Specifically, 5 failed LPE had redo-LPE and 3 failed LPE and 3 failed OPE had redo-OPE. Mean age at redo-PE was 127.8 days (range: 90–256 days). Redo-PE was performed 17–180 days (mean: 67.1 days) after primary PE; mean age at primary PE was 54.1 days (range: 30–76 days) for redo cases and 69.5 days (range; 21–146 days) for nonredo cases; P = .08. Mean weight at redo-PE was 4.8 kg (range: 2.6–6.5 kg); mean weight at primary PE was 3.9 kg (range: 2.6–5.0 kg) for redo cases and 4.5 kg (range: 2.5–7.1 kg) for nonredo cases; P = .10. JC was achieved in 6/11 redo-PE cases; SNL was achieved in 6/11 redo-PE cases. Redo-PE data were included in the overall analysis of LPE versus OPE according to the type of redo performed; 3/8 LPE subjects who had redo-OPE were included in OPE.
SBM assessments of subjects requiring redo before redo was indicated tended to have higher AST/ALT and γ-GTP and lower ChE, but differences were only significant for AST at the last scheduled assessment (3 months) before redo; P < .05. After redo, AST decreased and there were no differences in SBM and BSC for redo-PE and nonredo cases. In other words, outcomes according to SBM and BSC for redo-PE were the same as nonredo cases (see Fig. 5).
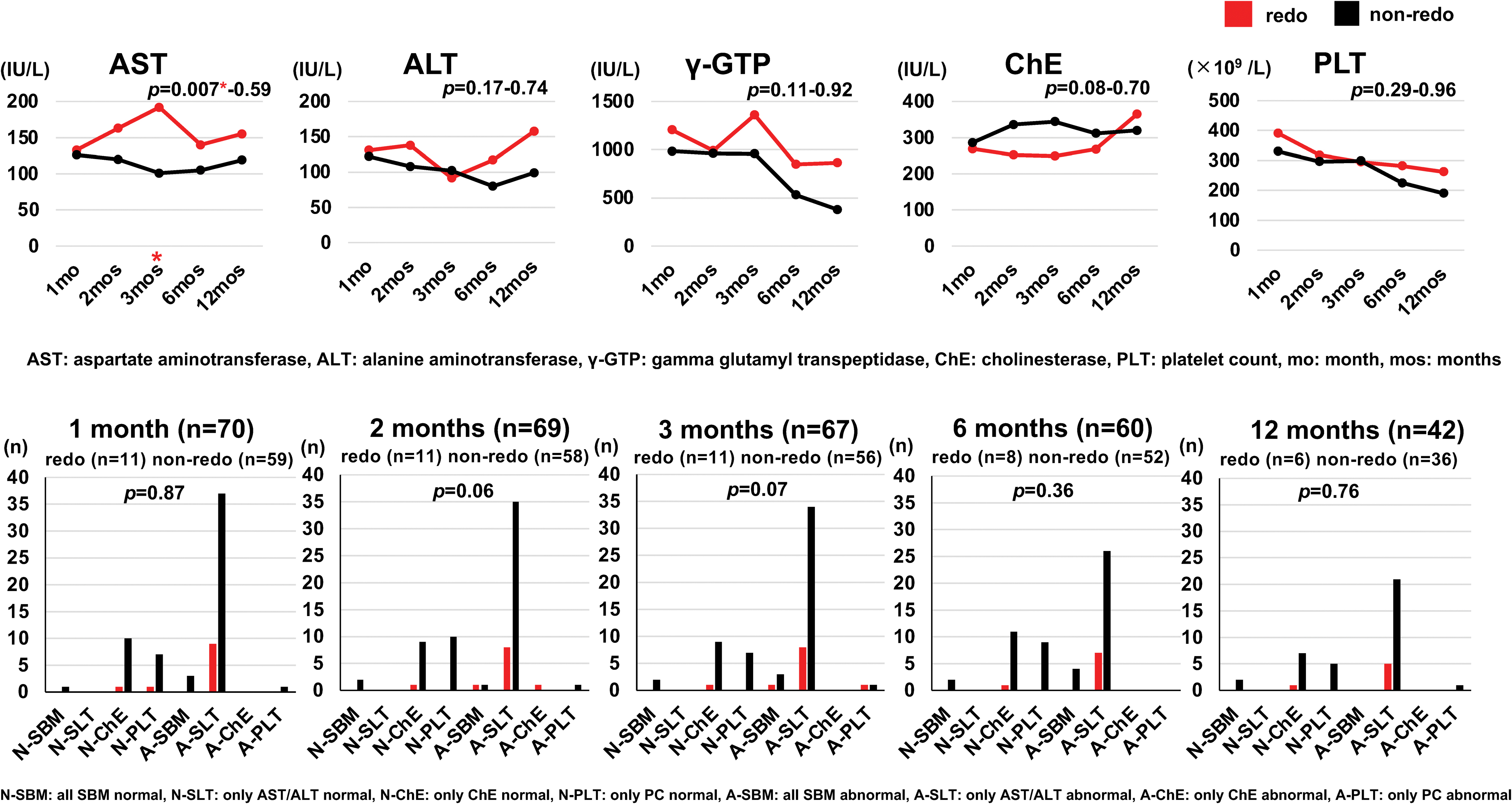
SBM and BSC for redo-PE cases. There were significant differences in SBM for AST at 3 months, the last assessment before redo-PE in redo-PE cases (P < .05). After redo-PE, AST decreased and there were no differences between redo-PE cases and nonredo cases for SBM and BSC. AST, aspartate aminotransferase; BSC, biochemical status categories; PE, portoenterostomy; SBM, selected biochemical markers. Color images are available online.
Discussion
Historically, LPE has come to be considered an inferior procedure with worse outcomes. While this study is limited somewhat by its retrospective design, the impact of LPE on BA patients was the same as for OPE; in other words, by choosing SBM that assess post-PE liver status specifically, the outcome of LPE was no worse than OPE, at least biochemically. Although the SBM used in this study have been reported previously, they have not been validated categorically as specific markers of success or failure of PE although they assess the clinical status using criteria that are relevant to BA. Of note, there are few reports that include ChE and PC as SBM although Davenport et al 24 reported that high PLT and low AST levels may be prognostic. Thus, ChE was added as an indicator of liver synthetic function and PLT to reflect hypersplenism associated with the natural progression of BA.
ChE was relatively preserved in many cases, but an upward trend was observed in the first few months after initial PE, along with decreased T-Bil, AST, ALT, and γ-GTP, suggesting that ChE may be useful as a postoperative indicator. γ-GTP is known to be raised in BA patients but was considered to be potentially useful for following liver cell and bile duct epithelial damage and cholestasis because of its sensitivity.20,25 In this study, it continued to remain high postoperatively irrespective of the operative technique and took more than 5 years to reach normal levels. For all the SBM investigated in Group 1, results for OPE seemed better, but statistically, there was only a significant difference in ALT at 6 months (P < .05), and no significant differences in SBM results according to the operative technique (Fig. 1).
As there were no differences between LPE and OPE identified in this study using SBM results, LPE could be reappraised as a valid option for treating BA rather than being bypassed for historical reasons. In fact, LPE could be associated with other advantages typical of MIS such as superior cosmesis because of smaller scars and less reported adhesions 14 that could influence the incidence of postoperative intestinal obstruction and the success of any future surgery.
Distributions of the eight BSC chosen specifically to assess liver status from different perspectives without functional overlap were not different between LPE and OPE, although transient significant differences were observed. Koga et al 26 reported that AST can continue to be high even after successful PE, suggesting that hepatocyte deterioration is progressive in BA; AST would appear to be correlated significantly with risk for LTx as early as 1 month post-PE. Thus, all post-PE cases with high levels of AST should be considered LTx candidates, especially if postoperative clinical improvement is poor. In fact, the simplest approach to outpatient postoperative monitoring may be observing AST/ALT closely during the first few months after PE. The most common BSC for both LPE and OPE in this study was A-SLT (only AST/ALT abnormal). In Group 1, AST/ALT gradually improved over time, with some subjects achieving normal results after 2 years.
While performing BSC analysis, the BSC category, N-SBM, was of particular interest because no similar data could be found in the literature. Midterm follow-up (5–7 years after PE) identified N-SBM in 6/70 subjects (3 LPE and 3 OPE), which fell to 3/70 (1 LPE and no OPE) on long-term follow-up (10 years after PE), indicating that N-SBM after PE using the SBM in this study is uncommon and unrelated to the PE technique. Despite good results reported for JC and SNL, data for N-SBM are surprisingly limited in the literature and other centers are encouraged to report data for their postoperative PE cases who are SNL with normal data to create a database for this important category of BA patients.
There are several reports in the literature about postoperative SBM and prognosis.16,19,24–27 One assessed SNL subjects after OPE with SBM and another compared LPE with OPE using SBM, but both are less intensive than the current study; in the SNL article, only OPE subjects were reviewed for a few months after surgery with no comparison with LPE, 16 and in the article comparing LPE and OPE with SBM, SNL subjects were not investigated specifically and the study period was for only 6 months after PE. 28 This is the first time for post-PE patients to be compared at multiple predetermined points in time according to the surgical technique (LPE or OPE) using SBM (AST, ALT, ChE, and PLT for all subjects and with the addition of γ-GTP for Group 1 subjects).
Redo-PE is performed more often in Japan because of limited access to LTx; in other words, patients indicated for redo-PE in Japan would probably have LTx at centers overseas.14,29,30 Redo-PE was performed using redo-OPE until 2018 when redo-LPE was introduced. More than half of the 11 redo-PE cases achieved JC in this study, and postredo SBM and BSC results were equivalent to nonredo subjects. The postoperative clinical status of redo-PE cases was similar to nonredo subjects according to the SBM and BSC analysis, suggesting that redo-PE has the capacity to improve deteriorating clinical status even in the LTx era. Unfortunately, follow-up after redo-PE in this study is inadequate for making a concrete recommendation about redo-PE, but it would appear from this study and a report about redo-LPE performed elsewhere with promising results 14 that redo-PE has the potential for improving the postoperative status of deteriorating BA patients. Although the technique would not appear to be an issue from the current study, further follow-up will clarify the effect of technique on the prognosis of redo-PE cases.
In terms of SBM/BSC biochemical analysis used in this study, LPE did not underperform and the results were not nearly as bad as previously reported. In fact, LPE was so similar to OPE that they could even be considered equivalent. Increasing the number of subjects and extending the follow-up will focus further attention on the potential of LPE and redo-PE for treating BA.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.