
Abstract
Introduction:
The enhanced-view extraperitoneal (eTEP) technique was first described for minimally invasive inguinal hernia repairs and later for laparoscopic ventral hernia repair. The objective of this study was to report our early experience and learning curve (LC) with the robotic-assisted eTEP (R-eTEP) approach.
Materials and Methods:
We performed a retrospective analysis of patients undergoing R-eTEP repair for ventral hernias from December 2018 to September 2021. A single surgeon operative time (OT)-based LC was evaluated.
Results:
A total of 81 patients underwent an R-eTEP from December 2018 to September 2021. Sixty-five patients were ultimately included in our analysis. Fifty-seven patients underwent eTEP-Rives–Stoppa (RS) and 8 patients underwent eTEP-transversus abdominis release (TAR). The median age in the whole cohort was 57 years (interquartile range [IQR] 51.5–64.5 years) with no difference between the groups. The median body mass index (BMI) was 31 kg/m2 (IQR 27–34.7 kg/m2) in the eTEP-RS group and 29.7 kg/m2 (IQR 28.5–31 kg/m2) in the eTEP-TAR group. There were 36 incisional hernias (63%) in the eTEP-RS group and 8 (100%) in the eTEP-TAR group. There were 14 recurrent hernias (25%) in the eTEP-RS group and 2 (25%) in the eTEP-TAR group. The LC was evaluated only in the eTEP-RS cases. We divided the cohort into 3 chronological groups (G1, G2, and G3), including 19 cases each. The median OT in each group was 177 (IQR 147–200), 153 (IQR 127–187), and 125 minutes (IQR 106–152 minutes), respectively. There was no difference in the median OT between G1 and G2 (P = .390). G3 had a shorter median OT than G2 (P = .02) and G1 (P = .001). There was no difference between these groups in median age, BMI, defect area, defect width, and mesh area.
Conclusions:
The R-eTEP approach has been shown to be safe and feasible for ventral and incisional hernia repairs. A statistically significant decrease in OT was observed after 38 cases.
Introduction
A wide array of surgical techniques have been described for ventral hernia repairs (VHRs). Many authors have described the laparoscopic approach to VHR with the positioning of an intraperitoneal underlay mesh.1,2 Advantages of a laparoscopic approach include reduction of surgical site infection (SSI), shorter length of stay, and a similar recurrence rates compared with an open approach.3,4
The enhanced-view extraperitoneal (eTEP) technique was first described by Dr. Jorge Daes for minimally invasive inguinal hernia repairs.5,6 The surgical steps of this technique involve a fast and easy creation of extraperitoneal domain, flexible trocar setup, and a large operative field. It can be easily attained by junior surgeons who are still mastering minimally invasive hernia repairs and complex cases.5,6
The Rives–Stoppa (RS) technique that includes the placement of mesh in the retromuscular space has been widely used for open VHRs. Its advantages include low rates of SSI and recurrence as well as restoring the abdominal wall functionality and avoiding any complications that arise with an intra-abdominal mesh.7–9 The eTEP access for VHR was first described by a multicenter study by Belyansky et al. 10 In the last 3 years, many authors have published results of the minimally invasive eTEP-RS technique with a large mesh overlap in the retromuscular space.10–26
Few studies in the literature show the robotic-assisted eTEP (R-eTEP) approach for ventral hernias. The objective of this study was to report our early experience and learning curve (LC) with the R-eTEP approach.
Materials and Methods
Study design
We retrospectively reviewed a prospectively collected database of cases performed between December 2018 and September 2021. All procedures were performed by one surgeon with a large experience in minimally invasive surgery and abdominal wall reconstruction at a single institution. Adult patients who underwent elective robotic VHR with retromuscular approach were included in this study. We excluded patients who had concomitant inguinal hernia repairs. In our LC analysis, we excluded patients who had concomitant transversus abdominis release (TAR) as this would increase outliers in operative times (OTs).
Data collection
Institutional review board approval was obtained to conduct this study. Data were retrospectively collected and divided into four sections: patient characteristics, hernia characteristics, perioperative data, and patient outcomes. Patient demographics and comorbidities were analyzed: age, sex, body mass index (BMI), diabetes mellitus, hypertension, chronic obstructive pulmonary disease, smoking status, stroke, cerebrovascular accident, previous myocardial infarction, and American Society of Anesthesiologists class. We did not collect data from open surgeries as our objective was to show the early results of minimally invasive procedures.
Preoperative data in the setting of incisional or recurrent hernias included type of primary hernia and/or presence of multiple hernia defects. Intraoperative and postoperative data consisted of defect area, mesh area, fixation of the mesh, OT, length of stay, intraoperative and postoperative complications, 30-day readmissions, and follow-up.
We also evaluated the LC of the surgeon doing only eTEP-RS cases. We divided this cohort into 3 discreet groups (G1, G2, and G3) organized in chronological order to assess improvement over time.
Surgical technique
The patient is placed in the supine position. The patient's hips are placed over the operating table's flexion point. The bed is flexed, extending the working space between the subcostal margin and anterior superior iliac spine to create more space for our port placement. Usually, the access is done on the patient's left side, unless there are prior incisions on this side (e.g., old stoma sites). Next, after reviewing a preoperative cross-sectional computed tomography image of the patient's abdomen, the width of the retrorectus space is measured and subsequently marked on the patient. A 5 mm Fios port (Applied Medical) is placed in the left upper quadrant (LUQ) just medial to the semilunar line. The retromuscular space is identified under direct vision after traversing the anterior sheath and rectus muscle. Then, the port is directed inferiorly at a 45° angle and insufflation is initiated.
Blunt dissection is performed to allow space creation for the second port placement 8 cm caudal the LUQ port and 1 cm medial to the semilunar to avoid any injuries to the neurovascular bundles. A spinal needle is utilized to ensure a safe tract into the retrorectus space, and an 8 mm robotic port is placed under direct vision. Electrocautery with a hook or Maryland dissector is used to create space inferiorly for an additional 8 mm robotic port at the left lower quadrant (LLQ), 8 cm inferiorly and 1 cm medial to the semilunar line. Before docking the robot, the camera is switched to the inferior port to complete the dissection superiorly and the initial 5 mm optical trocar is exchanged for an 8 mm robotic port. No assistant port is used.
The robot is docked from the right side of the patient. Dissection is initiated from lateral to medial toward the linea alba, performing a crossover at the subxiphoid area, taking advantage of the preperitoneal fat of the falciform ligament, and entering the contralateral retrorectus space by incising the posterior rectal sheath and dissecting the right retrorectus space. The dissection is carried out caudally toward the hernia, identifying the hernia sac and reducing its contents into the abdominal cavity.
After the dissection is complete, any opening on the peritoneum or posterior fascia (if there is no excessive tension) is closed using running 3-0 barbed sutures. The linea alba and hernia defect should be plicated with a running 0 barbed slowly absorbable or nonabsorbable suture. The mesh can be fixed in position with 0 Vicryl® interrupted sutures. Once the mesh lays flat in the retrorectus space, the abdomen should be deflated under direct vision, thus completing the procedure. Drains are only used on TAR cases.
Statistical analysis
A descriptive analysis was performed. Continuous variables whose distribution approximated normality are reported as mean and standard deviation, and median and interquartile range (IQR) for those with skewed distributions. Categorical variables are reported as frequencies and percentages. Chi-square and Fisher's exact tests were used for categorical variables. Nonparametric tests were used for continuous variables. A P value of <.05 was considered statistically significant. Data were analyzed using the SPSS v.28 Chicago: SPSS Inc.
Results
A total of 81 patients underwent an R-eTEP from December 2018 to September 2021. We excluded from our analysis patients who had concomitant inguinal hernia repair and patients with no 30-day follow-up. Sixty-five patients were ultimately included in our analysis. Patient characteristics are listed in Table 1. Fifty-seven patients underwent eTEP-RS and 8 patients underwent eTEP-TAR. The median age in the whole cohort was 57 years (IQR 51.5–64.5 years) with no difference between the groups. The median BMI was 31 kg/m2 (IQR 27–34.7 kg/m2) in the eTEP-RS group and 29.7 kg/m2 (IQR 28.5–31 kg/m2) in the eTEP-TAR group. There were 36 incisional hernias (63%) in the eTEP-RS group and 8 (100%) in the eTEP-TAR group. There were 14 recurrent hernias (25%) in the eTEP-RS group and 2 (25%) in the eTEP-TAR group (Table 1). Six patients had lateral defects associated with the midline hernias in the eTEP-TAR group (75%) being 3 patients L1 and 3 L2. Only 2 patients had associated lateral defects in the eTEP-RS group (one L1 and one L2).
Patient Characteristics and Perioperative Outcomes
Bold values are statistically significant.
Median (IQR).
EBL, estimated blood loss; EHS, European Hernia Society; LOS, length of stay; IQR, interquartile range; SSI, surgical site infection.
The median defect area was 32 cm2 (IQR 9–72 cm2) in the eTEP-RS group and 78.5 cm2 (IQR 43–102.5 cm2) in the eTEP-TAR group (P = .027) (Table 1). The median hernia width was 4 cm (IQR 2–5 cm) in the eTEP-RS group versus 5.5 cm (IQR 4.6–7.7 cm) in the eTEP-TAR group (P = .013). Regarding mesh area, the eTEP-RS group had a lower median area of 504 cm2 (IQR 412.5–565 cm2) versus 638 cm2 (IQR 600–894.7 cm2) in the eTEP-TAR group (P < .001).
In all cases, polypropylene mesh was positioned in the retromuscular space, and the defect was primarily closed with absorbable suture. Mesh was fixated mostly with absorbable suture, followed by tacks and fibrin glue.
The median OT was 151 minutes (IQR 124.5–181 minutes) in the eTEP-RS group versus 215.5 minutes (200.5–236.7 minutes) in the eTEP-TAR group (P < .001). There were two conversions to open, three 30-day readmissions, being two in the eTEP-RS group and one in the eTEP-TAR group, and no recurrences in 30 days.
Learning curve
The LC was evaluated only in the eTEP-RS cases where the cohort was more homogeneous. We divided the cohort into 3 chronological groups (G1, G2, and G3), including 19 cases each (Table 2). The median OT in each group was 177 (IQR 147–200), 153 (IQR 127–187), and 125 minutes (IQR 106–152 minutes), respectively. There was no difference in the median OT between G1 and G2 (P = .390). G3 had a shorter median OT than G2 (P = .02) and G1 (P = .001) (Fig. 1). There was no difference between G1 and G2 regarding the median estimated blood loss (EBL) (P = .105), but the median EBL in G3 was lower than that in G2 (P = .026) and in G1 (P < .001) (Table 2). There was no difference between these groups in median age, BMI, defect area, defect width, and mesh area.
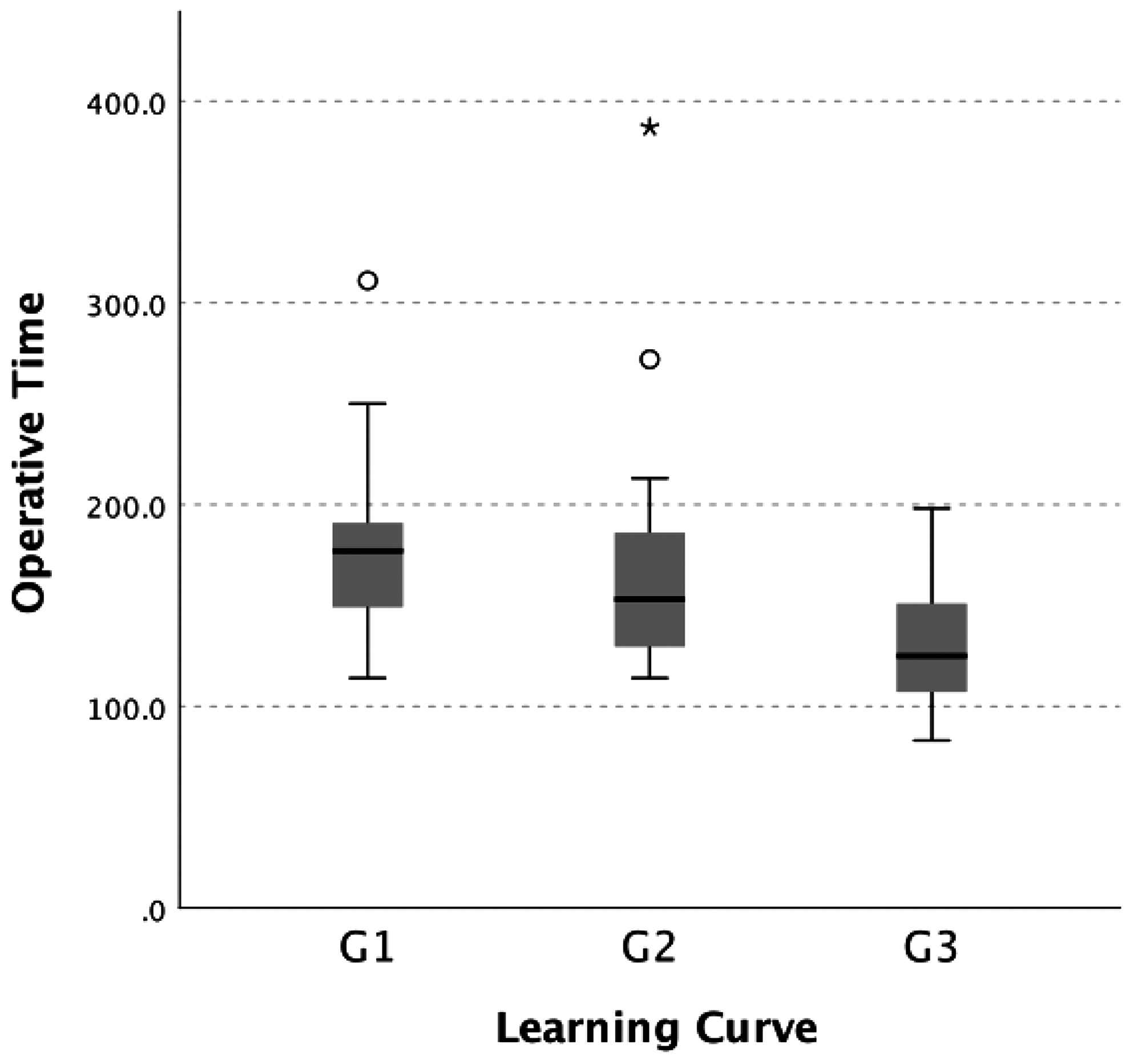
Learning curve evaluating the median operative time between the groups. G2–G1 (P = .390), G3–G2 (P = .020), G3–G1 (P = .001).
Learning Curve of Robotic Enhanced-View Extraperitoneal
Bold values are statistically significant.
Median (IQR).
P-value between G1 and G2.
P-value between G2 and G3.
P-value between G1 and G3.
P-value between the 3 groups.
EBL, estimated blood loss; EHS, European Hernia Society; LOS, length of stay.
Discussion
The eTEP technique has been shown to be a safe and feasible option for VHRs. 11 The robotic platform allows surgeons to perform the RS repair using both transabdominal and TEP approaches. Our study demonstrated that the R-eTEP is safe and effective in the short-term, with similar results to the literature. Furthermore, we presented a LC for this procedure based on the OTs from a single surgeon's experience.
There are few studies in the literature showing the R-eTEP approach. Belyansky et al. published the first cohort of 37 patients who underwent R-eTEP approach for primary and incisional hernias. 11 Lu et al. also compared both laparoscopic and R-eTEP techniques for ventral and incisional hernias. 12 Patients with a larger defect size, mean BMI, and more complex abdominal wall defects were more likely to undergo the robotic approach. This may have influenced the longer mean OT and higher operative cost of R-eTEP procedures when compared with laparoscopic approach.
Kudsi and Gokcal reported early outcomes of 52 patients undergoing R-eTEP by a lateral docking approach. 27 This docking was used for all patients with lateral or midline defects. The mean console time was 121.6 minutes, with no intraoperative complication or conversion to conventional laparoscopy or open surgery. Some studies looked at the positioning of ports relative to the location of the hernia in laparoscopic eTEP repairs.10–14,16,23,26 For hernias located in the upper abdomen, trocars should be placed below the umbilicus. For hernias located in the lower abdomen, trocars should be placed above the umbilicus.
Köhler et al. described the precostal top-down eTEP for any type of hernia. The authors performed a precostal access to the right retrorectus compartment through an incision 5 cm lateral to the sternum at the level of the xiphoid's cranial end. 15 Prakhar et al. included only patients with paraumbilical and incisional hernias in lower midline using the left subcostal incision to enter the retrorectus space. 25 Studies reported the robotic-assisted approach detailed the superior, lateral, and inferior docking according with the hernia location.11,24,27 The lateral docking is becoming the most common approach because it can be used independently of the hernia location.
The eTEP-RS allows the surgeon to repair hernias up to 10 cm wide; if larger, an endoscopic TAR should be performed. 28 An associated TAR may be necessary for wider hernia size or larger defect area. This can increase OTs and complication rates when compared with eTEP-RS, as demonstrated by Quezada et al. 26 Belyansky et al. 10 reported a higher length of stay for the eTEP-TAR group. In our study, patients undergoing eTEP with myofascial release had a higher median defect area, median defect width, longer OT, and EBL when compared with patients undergoing eTEP-RS. Furthermore, 6 patients from the eTEP-TAR group had lateral defects. The myofascial release may be necessary to accomplish better positioning of the mesh and appropriate overlap.
The eTEP technique allows the surgeon to address both ventral and inguinal hernias in the same retromuscular space. In our initial cohort, there were 10 patients with concomitant unilateral and bilateral inguinal hernias that we excluded from our analysis, thus aiming for a more homogeneous cohort. There were two conversions in our cohort. One was due to a challenging fibrosed incisional hernia, and the other was due to muscle atrophy that did not allow us to finish the procedure robotically. There were three 30-day readmissions in our cohort. One of the readmissions was due to postoperative abdominal pain. The other two were non-related to the operation. Our median length of stay was less than 1 day for the eTEP-RS group and 1 day for the eTEP-TAR group. This is a clear advantage of the robotic platform over the open approach when performing these complex abdominal wall reconstructions.
The LC of complex surgical procedures such as complex abdominal wall repairs depends on several factors. These include patient characteristics such as BMI and age, as well as hernia characteristics such as defect width and defect area. Therefore, evaluating the proficiency of a surgeon based on OT may not be ideal. In our cohort, all the groups involved in the LC analysis had no differences in their characteristics. Furthermore, surgeons usually perform a new surgical procedure with less challenging cases. With time and experience, the surgeon is more likely to attempt these procedures in complex cases. Studies have showed that higher surgical volume is correlated with improved outcomes.29,30 Regarding our LC analysis of robotic eTEP-RS, our study showed a consistent decrease in OT that became statistically significant after 38 cases. Kudsi et al. performed an LC study in 81 patients who underwent robotic RS for primary ventral and incisional hernias, and they observed a decrease in OTs and adverse outcome rates after 29 and 51 cases. 31
Limitations of the study
This is a retrospective study with a small sample that evaluated the surgical outcomes and LC of one surgeon who was well experienced in robotic surgery. In this study, we had a small sample size that was underpowered to detect small differences. Furthermore, we had a short median follow-up of 26 days.
Conclusions
The R-eTEP approach has been shown to be safe and feasible for ventral and incisional hernia repairs. This study shows an OT-based LC of a single surgeon performing robotic eTEP-RS. A statistically significant decrease was observed after 38 cases. Future studies with longer follow-up and larger cohorts are necessary to better understand the acquisition of proficiency by surgeons performing this complex procedure.
Footnotes
Authors' Contributions
Study design: F.M., L.T.C., and D.L.L. Data collection and analysis: D.L.L. and R.B. Article preparation and editing: D.L.L., F.M., R.B., and L.T.C.
Disclosure Statement
D.L.L. and R.B. disclose no financial relationships with industry or conflicts of interest. L.T.C. discloses consulting fees from BD. F.M. discloses consulting fees from BD, Intuitive and Medtronic, outside the submitted study.
Funding Information
No funding was received for this article.