
Abstract
Introduction:
In children, gallbladder disease has become more common due to the rise in childhood obesity and subsequent shift in etiology. While the gold standard of surgical management remains a laparoscopic technique, there has been increasing interest in robotic-assisted techniques. The aim of this study is to report a 6-year update on the experience of treating gallbladder disease with robotic-assisted surgery at a single institution.
Materials and Methods:
A database was created to prospectively collect patient demographic and operative variables at the time of operation from October 2015 to May 2021. Descriptive analysis of select available variables was performed using median and interquartile ranges (IQRs) for all continuous variables.
Results:
In total, 102 single-incision robotic cholecystectomies and one single-port subtotal cholecystectomy were performed. From available data, 82 (79.6%) patients were female, median weight was 66.25 kg (IQR: 58.09–74.24 kg), and median age was 15 years (IQR: 15–18 years). Median procedure time was 84 minutes (IQR: 70.25–103.5 minutes) and median console time was 41 minutes (IQR: 30–59.5 minutes). The most frequent preoperative diagnosis was symptomatic cholelithiasis (79.6%). One (0.97%) operation was converted from a single-incision robotic approach to open.
Conclusion:
Single-incision robotic cholecystectomy is a safe and reliable technique for the treatment of gallbladder disease in the adolescent population.
Introduction
Gallbladder disease is one of the most common surgical diseases in the United States, with laparoscopic cholecystectomy being one of the most common procedures done in the adult population. 1 The volume of cholecystectomies in the pediatric population is far less than in adults, and, historically, the etiology of pediatric cholelithiasis has been secondary to hemolytic disorders. 2 However, the rise in childhood obesity over the past few decades has caused both a shift in etiology as well as an increase in the rate of cholelithiasis requiring cholecystectomy in the pediatric population.3,4 Current estimates of cholelithiasis in the pediatric population range from 1.9% to 4%.5–7
While laparoscopic cholecystectomy remains the gold standard of surgical management, 8 there is a growing interest in the use of robotic-assisted techniques. Robotic-assisted approaches share the advantages of laparoscopy, while also offering solutions to its disadvantages, including three-dimensional visualization, greater degrees of freedom and dexterity with wrist-like graspers, tremor reduction, motion scaling, improved surgeon ergonomics, and a shorter learning curve due to intuitive movements.9–12 Despite its advantages over laparoscopy, robotic surgery has not yet been widely adopted in pediatric surgery due to the perceived challenges in this population, namely the smaller body habitus of children.13,14 Some reports show the average age at which gallstone disease affects the pediatric population is from 12.9 to 14.3 years, thus making these limitations in size less of an issue for the purposes of cholecystectomy.2,4,5
Literature from the adult population has shown similar outcomes with robotic-assisted cholecystectomy when compared to laparoscopic approaches.15–17 Currently, there is a paucity of literature describing robotic cholecystectomies in children and adolescents, although reports have demonstrated this approach's efficacy and safety.13,18–22 The aim of this article is to provide an update on the performance of single-incision robotic cholecystectomies at a pediatric hospital following a significant increase in case volume after an initial report.
Materials and Methods
A database was created to prospectively capture all robotic surgeries occurring within the institution where the cases in this study were performed. All operations in this study occurred at a freestanding children's hospital, that is both a level 1 pediatric trauma center and international referral center. The operative technique has been previously described by the senior author of this study (F.A.). 20 The database was queried for all single-incision robotic cholecystectomies performed by the Department of Pediatric Surgery from the creation of the database in October 2015 to May 2021. Multi-port robotic cholecystectomies were excluded from this analysis. Descriptive analysis of select available variables was performed using median and interquartile ranges (IQRs) for all continuous variables.
For cases where data were missing, the missing observation was not included in the descriptive analysis of that variable, but the case remained in the overall study count and additional observations from that case were analyzed when available for other variables. All operations were completed by authors F.A., L.M., J.C., and S.S. F.A. served as the “master robotic surgeon” and was responsible for the development of the robotic surgery program within the department. All other attending surgeons completing robotic surgeries had to first observe 5 robotic procedures performed by F.A. and then proceeded to be proctored by F.A. for an additional 5 robotic procedures before they were able to operate autonomously. The creation of the database and subsequent analysis were approved by the Institutional Review Board of Nicklaus Children's Hospital.
Results
In total, 103 single-incision robotic cholecystectomies were performed from October 2015 to May 2021. Six (5.88%) operations included an intraoperative cholangiogram, 1 (0.97%) operation was a single-incision subtotal cholecystectomy, 1 (0.97%) operation was converted to open, and no operation was converted to laparoscopic or multiport. As previously mentioned, some variables were missing in the database; these included 1 weight, 5 estimated blood loss, and 11 console times.
Full demographic and operative measures are listed in Table 1. Overall, 82 (79.6%) patients were female, median weight was 66.25 kg (IQR: 58.09–74.24 kg), and median age was 15 years (IQR: 15–18 years). Across all cases, median procedure time was 84 minutes (IQR: 70.25–103.5 minutes) and median console time was 41 minutes (IQR: 30–59.5 minutes). Median estimated blood loss was 3 mL (IQR: 2–5 mL).
Demographics and Operative Measures
Patient demographics and operative variables.
EBL, estimated blood loss; IQR, interquartile range.
The highest number of operations completed in a single year (Fig. 1) occurred in 2017 with 24. The most frequent preoperative diagnosis (Table 2) was symptomatic cholelithiasis (79.6%). There were 16 different operative assistants consisting of fellows, residents, and medical students.
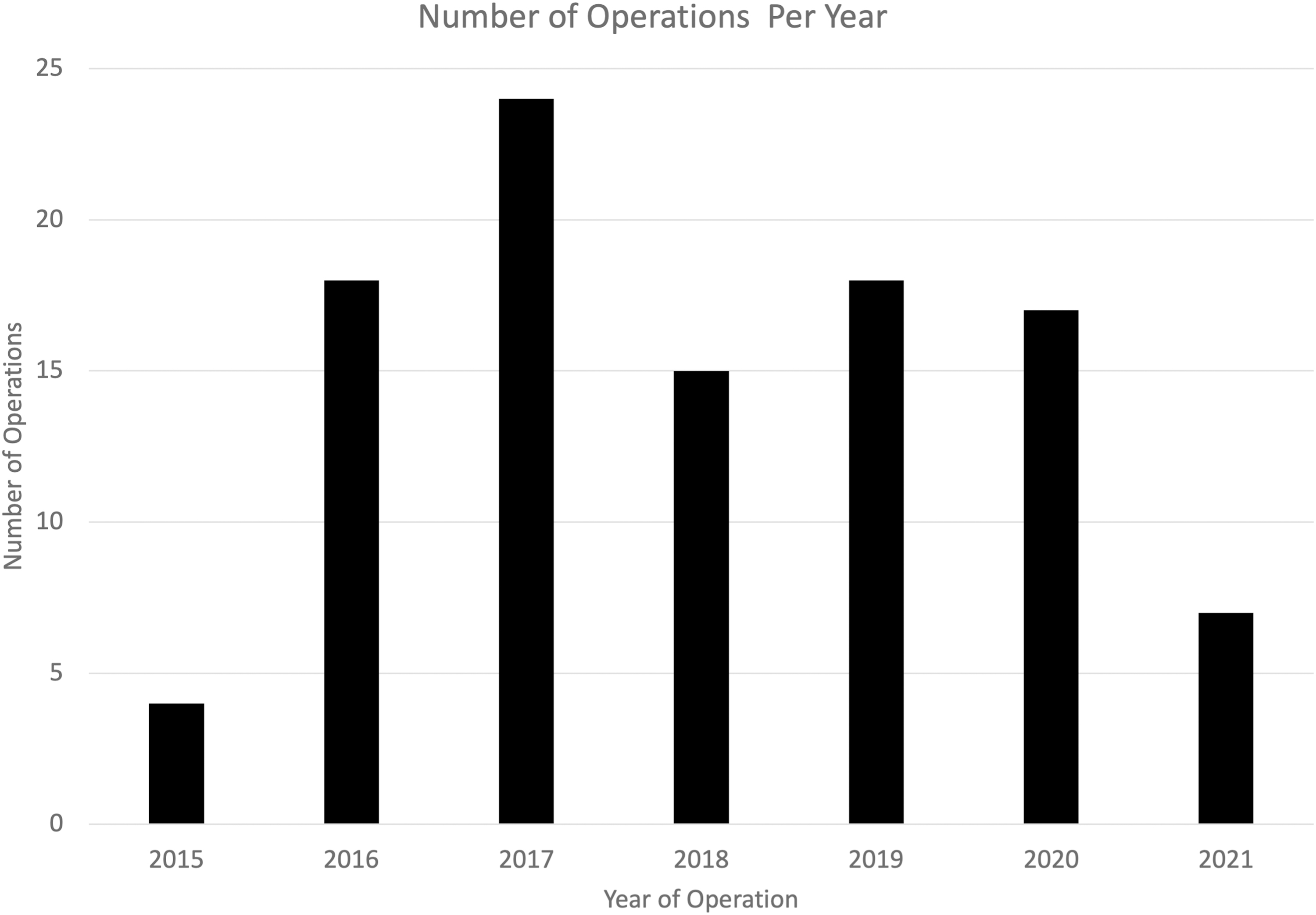
Operative Volume by Year.
Unique Preoperative Diagnosis
Number of unique preimperative diagnosis.
In total, 15 patients (14.6%) were kept in the hospital overnight for observation after their operation and were discharged on postoperative day 1. All other patients were discharged on the same day as the operation on Tylenol and Motrin, with no narcotics.
In the instance of the conversion from robotic-assisted to an open surgical technique, the patient had multiple previous operations. As a consequence, many adhesions had formed throughout the abdomen and after an initial attempt to proceed robotically, ultimately, the decision was made that the safest operative technique for the patient was to proceed with an open surgical technique.
Across all patients, follow-up ranged from 6 months to 6 years with no incidence of incisional hernia in any patient and no other serious complication during this period. Two patients were treated in an outpatient setting with antibiotics for simple wound infection (Clavien-Dindo classification Grade I).
Discussion
Following the diagnosis of gallbladder disease, the gold standard of surgical management remains laparoscopic cholecystectomy in both the adult and pediatric populations.8,23 However, since its first use in the early 2000s, robotic-assisted surgery has been gaining popularity in the pediatric population.24,25 This study reports on the operative characteristics and outcomes of single-incision robotic cholecystectomy (SIRC) in a pediatric population. Our study describes a longitudinal prospective case series, showing the continued feasibility and safety of performing this operative technique, with a conversion rate of 0.97% and no major complication.
As minimally invasive surgery has continued to evolve, single-incision or single-port techniques have been used in both laparoscopic and robotic approaches as a means of achieving superior cosmetic results and improved recovery after surgery.23,26 Since the introduction of single-site instrumentation to robotic surgery in 2011, SIRC has been reported to be safe and effective in the adult population, but the literature describing SIRC in children remains limited.19,21,26–30
The senior author of this study previously reported the safety, feasibility, and cosmetic outcomes of SIRC with a small sample size of 15 cases. 20 This study expands upon these previous results with a sevenfold increase in sample size over the course of 6 years, with the expansion of participating surgeons to a total of 5. With the growth of the program during this time, it is evident that clinical observation followed by in-depth proctoring from a “master surgeon” can be a reliable avenue for the acquisition of new surgical skills, in this case robotic surgical techniques, for pediatric surgeons.
In addition to providing an update from a single institution, this report documents the successful completion of six intraoperative cholangiograms using the robot. The technique employed by the authors is as follows: a small catheter is placed into the abdomen through a laparoscopic instrument port that had been used for one of the robot arms by a surgical assistant. Once the catheter is placed into the abdomen, the surgeon uses the robot to place the catheter into the cystic duct. Once the catheter is securely in place, the robot is undocked, so the appropriate equipment for the cholangiogram can be safely positioned. Once the cholangiogram is complete, the robot is re-docked, and the catheter safely removed from the cystic duct and abdomen.
Single-incision laparoscopic cholecystectomy (SILC) has been reported to be both safe and feasible for use in the pediatric population, although it is a technically challenging operation with disadvantages and limitations.23,26,30,31 These limitations include a narrow working space, loss of triangulation with clashing of instruments, longer operative times, and increased complications.23,30
Robotic-assisted surgery may alleviate some of these limitations, allowing for better vision and improved dexterity. SIRC offers a three-dimensional view of the operative field and a greater degree of freedom of operative instruments with intuitive movements, as opposed to the inverted movements of SILC, increasing the ability of the surgeon to accurately and confidently maneuver in a narrow working space.28,30 With much of the patient population of this study being adolescent, the typical concerns of robotic surgery in pediatric populations, namely small working area, were limited in our experience. However, it is our experience that difficulties with using the robot in smaller surgical fields can be overcome with appropriate trocar selection and operative experience.
SIRC requires additional time to set up, dock, and undock the robot, which can add to the total operative time when compared to SILC. Kulaylat et al. report a median operative time of 98 minutes with robotic cholecystectomy which was significantly longer than the laparoscopic cholecystectomy time of 78 minutes at their institution (P < .001). 21 Subanalysis showed that the mean operative time of the robotic cholecystectomies performed using a single incision was 99 minutes. 21
Despite concerns over increased operative time, we found that our median procedure time of 84 minutes was comparable to some reported pediatric SILC times, ranging from 65 to 145 minutes, and nearly matched the average time of 86.5 minutes reported in a review of 6 studies on SILC from 2009 to 2011.31–33 A study of adult patients undergoing SIRC was able to demonstrate an average total operative time of 71 minutes. 30 The difference in size between adults and children may explain this difference in average operative time with a larger operative field in the former, but confirmation of this remains to be seen.
Jones reports a median console time of 39 minutes in pediatric SIRC, comparable to our median console time of 41 minutes. 18 These times are also comparable to those reported in the adult population, which can range from 32 to 39 minutes.28,30,34 In comparison to the senior author's previous study, our median operative time is similar, although the range of operative times has decreased with the longest operative time moving from 169 to 103.5 minutes, possibly owing to an increase in experience of both the surgeon and the operating room team. 20 Our study does not include a cost analysis, but it is reasonable to conclude that a robotic operation that leads to longer operative times may lead to higher costs.
Overall, we demonstrated a 0.97% conversion rate with no major postoperative complications. In the single instance of conversion in this study, it was deemed that the patient's abdomen had adhesions too extensive to proceed laparoscopically. Rather than viewing this a “failure” of the technique, we interpret this conversion as a demonstration in the safe and appropriate application of a robotic surgical technique.
A comparison of robotic versus laparoscopic cholecystectomies found a complication rate of 7.6% and 4.1% respectively. 21 This same comparison also showed no difference in conversion rate between the two techniques, with 0 robotic cholecystectomies converted during the period of the study. A study analyzing SIRC in an adult population demonstrated a conversion rate of 2% in a study population of 100 patients. 30
Approximately 85% of our patient population was discharged home on the day of the procedure. In contrast, a review found that the average length of hospital stay after single-port laparoscopic cholecystectomy in children was 1.4 and 1.2 days after a multiport technique. 31
The limitations of our study include missing data points not collected at the time of the operation, given the prospective nature of the database. In addition, the sample size may limit the generalizability of the study findings. The study sample could be prone to selection bias, given the convenience sampling that generates our sample and the manner in which the attending surgeon chose the operative technique to use. The operative technique chosen includes using a single incision.
Subsequently, this analysis is limited by a lack of data collected to compare a single-incision vs multiple-incision technique regarding cost-effectiveness, cosmesis, or patient recovery. However, the authorship concludes it is logical that a single incision is preferable cosmetically and in terms of recovery. 35 As well, with this being a single-institution study, it may not be generalizable across geographies and different practice settings. Finally, case series may be prone to bias, given their inherent lack of a comparison group.
Conclusion
Single-incision robotic cholecystectomies remain a safe and feasible treatment modality for gallbladder disease in the pediatric population. Further investigations should continue to elucidate advantages between operative techniques for gallbladder disease in pediatrics populations, namely perioperative complications, length of stay, and cost-effectiveness between laparoscopic and robotic techniques.
Footnotes
Authors' Contributions
M.T.H.: conceptualization, data curation, formal analysis, methodology visualization, writing—original draft, and reviewing and editing. M.M.: visualization and writing—reviewing and editing. S.R.: data curation and writing—revieing and editing. J.C., S.S., and L.M.: conceptualization and writing—reviewing and editing. : F.A.: conceptualization, data curation, formal analysis, methodology, supervision, validation, and writing—reviewing and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.