
Abstract
Introduction:
Surgical intervention is the definitive management for congenital diaphragmatic hernia (CDH) repair from 1902. Since this time, two mainstay approaches have been used, open and minimally invasive surgical (MIS) repair. An invasive laparotomy is used in around 91% of cases. So, this systematic review of the published literature will compare the surgical outcomes of open (CDH) repair vs MIS for CDH repair and will determine which approach is superior.
Material and Methods:
Our literature search across MEDLINE and EMBASE included articles from 2004 to 2022, incorporating pediatric CDH repairs, human subjects only, and English language articles. Primary outcomes analyzed were rate of recurrence, length of surgery, length of hospital stay, use of diaphragmatic patch, mortality, postoperative chylothorax, and extracorporeal membrane oxygenation (ECMO) use postoperatively.
Results:
After application of exclusion criteria, 32 articles were reviewed. Comparison of MIS repair versus open repair had a rate of recurrence at 8.6% versus 1.6% (P < .00001). Length of hospital stay was 19.6 days versus 33.6 days (P = .0012), mortality rate at 4.6% versus 16.6% (P < .0001), patch repair required in 19.6% versus 55.4% (P = < .00001), and postoperative ECMO use of 3.7% versus 12.3% (P < .00001), respectively.
Conclusion:
MIS repair is associated with decreased length of hospital stay, reduced mortality rate, and postoperative ECMO usage. Hernia recurrence is still high among MIS repair groups compared to the open repair groups. Large, multicentered randomized control trials are recommended for further analysis to decipher the true superior surgical intervention.
Introduction
The formation of the diaphragm is complete between the 8th and 12th week of gestation with growth of the septum transversum, and later the pleuroperitoneal membrane.1,2 Congenital diaphragmatic hernias (CDHs) are a congenital malformation characterized by incomplete formation of the diaphragm with the presence of an orifice. It results in protrusion of the abdominal viscera into the thoracic cavity.1,3 Most commonly CDHs protrude on the postero-lateral left side of the diaphragm (Bochdalek) in >85% of cases and postero-lateral right side (Bochdalek) in ∼10% of cases. Rarer forms comprise of Morgagni hernias that are an anterior parasternal or retrosternal hernia presenting in 2% of cases and central hernia involving the central tendinous aspect of the diaphragm.2,4 CDH cases have a 1-week survival rate of 69.3%, and therefore, planned tertiary perinatal center delivery is recommended. 5 Their classification can be determined by the size of the defect as depicted in Table 1.
Congenital Diaphragmatic Hernia Classification Based on Defect Size
CDH, congenital diaphragmatic hernia.
Although the exact cause is unknown, it is postulated that the development of CDH increases with chromosomal abnormalities relating to genetic disorders such as Fryns syndrome, Pallister–Killian mosaic syndrome, and Donnai–Barrow syndrome. 3 Maternal tobacco exposure, pregestational diabetes, maternal age ≥35 years old, and maternal alcohol intake correlate with an increased risk of CDH formation. 6 CDH is prevalent in 2.3/10,000 live births across Europe, and 1.6/10,000 live births are isolated CDH cases, with marginally more male:female cases. 5
Antenatal ultrasound screening, complemented by magnetic resonance imaging (MRI), has proven to identify >70% of CDH cases.1,2 Unidentified cases can present in the neonatal period with respiratory distress from pulmonary hypoplasia, pulmonary hypertension, gastroesophageal reflux disease (GORD), cyanosis, tachypnea, and a scaphoid abdomen.1–3 Severity of CDH presentation varies according to the severity of pulmonary hypertension, pulmonary hypoplasia, associated cardiac defect, and associated chromosomal disorder.1,3
Management of CDH revolves around the stabilization of neonates before the definitive treatment of surgical repair. Respiratory stabilization is important before surgical intervention with studies highlighting the beneficial outcomes of delayed surgical repair (>24 hours) compared to immediate postdelivery surgery. 7 Gentle ventilation with or without high-frequency oscillatory ventilation is required, as without stabilization persistent pulmonary hypertension (PPHN) can occur from lung hypoplasia. 8 A peak inspiratory pressure of ≤25 cm H2O is advocated by the CDH EURO Consortium to avoid lung damage and reduce mortality rates. 7 If these measures fail, extracorporeal membrane oxygenation (ECMO) can be used as rescue therapy before surgery to improve surgical outcomes and pulmonary physiology, but is rarely reported postoperatively. 9 The CDH Euro Consortium has formulated a selection criterion for ECMO use (Table 2).
Congenital Diaphragmatic Hernia EURO Consortium Extracorporeal Membrane Oxygenation Criterion
CDH, congenital diaphragmatic hernia; ECMO, extracorporeal membrane oxygenation.
Since the first successful CDH surgical repair in 1902 which was undertaken using a laparotomy, the minimally invasive surgical (MIS) approach has gained traction. 10 MIS incorporates both thoracoscopic and laparoscopic approaches. Open repair by a laparotomy through a subcostal incision occurs in 91% of cases. 11 The rise in MIS since its emergence, particularly thoracoscopy with the insertion of two to four trocars within the intercostal space, is becoming more common. 12 Open repair is seen mainly in larger, complex defect repairs and thoracoscopy reserved for type A and B, low risk defects.
Comparative data for the two gold standard approaches are sparse with small sample sizes among studies and limited representation of data with the MIS approach. It is important to undertake a systematic review to analyze the published literature of open CDH repair versus MIS CDH repair, to gain a greater understanding of which approach is better.
Materials and Methods
We performed a systematic review by conducting a pediatric literature search of studies outlining the outcomes of neonates and infants undergoing surgery (open or MIS) for CDH. In line with our aims of the review we used EMBASE and MEDLINE to obtain the chosen publications. Those included within the study were publications from 2004 to 2022, limited to pediatric patients undergoing CDH repair (0–18 years), human subjects, and English language articles only. Searched terms used for identification included “open versus thoracoscopic CDH repair,” “open versus laparoscopic CDH repair,” “open versus MIS CDH repair,” “open CDH repair,” “thoracoscopic CDH repair,” “laparoscopic CDH repair,” and “MIS CDH repair.”
All articles retrieved were independently evaluated. Retrospective and prospective study data on CDH repair were included. All were nonrandomized control trials. Inclusion of publications was discussed by study authors, and extraction of data was commenced.
Data collected from each publication considered the following primary measures of the study: rate of recurrence, length of surgery, length of hospital stay, use of diaphragmatic patch, mortality, postoperative chylothorax, and use of ECMO postoperatively. Secondary measures considered were as follows: number of patients treated by each approach, age at surgical intervention, and length of follow-up.
Collected data were presented as mean (±standard error of the mean)/(range) and median (interquartile range). Assessing continuous and binary parametric data were attained through an unpaired t-test and Fisher's exact test, respectively. A P ≤ 0.05 was used to measure significance.
Results
The initial literature search retrieved 57 publications from EMBASE and MEDLINE, 27 of these were duplicates and removed from the review (Fig. 1). Reviewing the abstracts, 10 were excluded primarily, in conjunction with the exclusion criteria, leaving 20 titles for in-depth review. An additional 16 articles were identified from references of the 20 original articles and underwent full text review. After careful reading of the full titles, another four articles were excluded based on being review articles (2) and conference abstracts without full text publications (2). Thirty-two articles were included in the final review (Table 3).
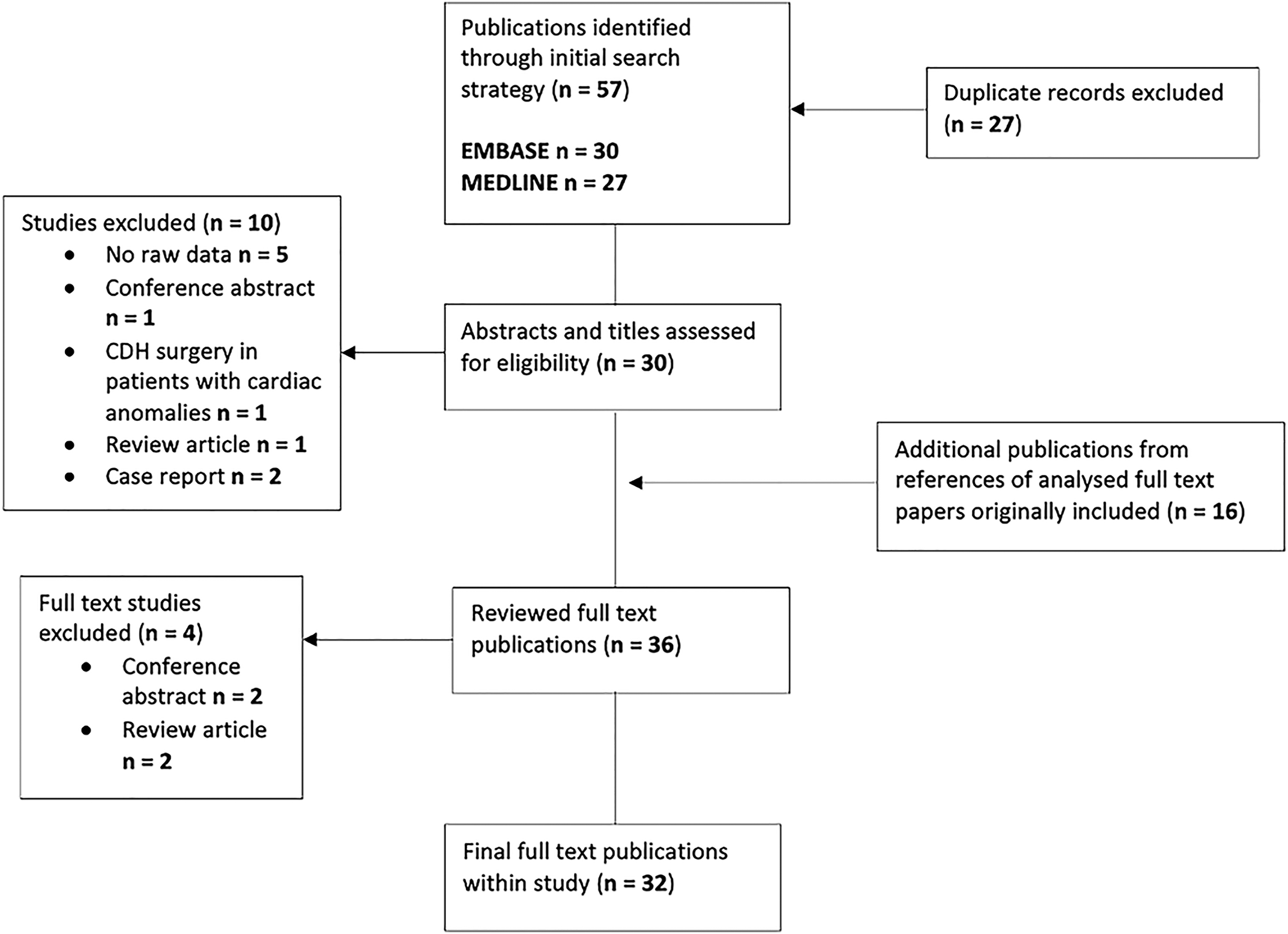
PRISMA flow diagram depicting the selection criteria with appropriate exclusions for analysis of postoperative outcomes into those patients undergoing MIS versus open CDH repair. CDH, congenital diaphragmatic hernia; MIS, minimally invasive surgery.
Summary of Literature Analysis
Mean.
Median.
MIS, minimally invasive surgery
We identified 9385 patients throughout the 32 publications reviewed. One thousand eight hundred sixteen (19.4%) underwent MIS CDH repair, and 7569 (80.6%) were repaired openly. Their age ranged from 0 to 1017 days of life from when their surgery occurred and length of follow-up between 1 and 168 months postsurgery.
Comparison for rate of recurrence between MIS CDH repair and open CDH repair reveals a six-times higher rate of recurrence for those patients undergoing MIS repair compared to open (8.6% versus 1.4%, P = < .00001). Data were retrieved from 31 publications and statistically significant difference with MIS/thoracoscopic repair resulting in more hernia recurrences, subsequently leading to further surgical intervention for the patient (Table 4).
Comparative Data for Thoracoscopic/Minimally Invasive Surgery Congenital Diaphragmatic Hernia Repair and Open Congenital Diaphragmatic Hernia Repair
Mean value.
CDH, congenital diaphragmatic hernia; ECMO, extracorporeal membrane oxygenation; MIS, minimally invasive surgery.
MIS patients had a mean of 19.6 days (5.6–40.7) within hospital, and open repair patients had a mean of 33.6 days (17–65), P = .0012 (Table 4).
The mean operative time of open CDH repair was 119.2 minutes (70–171) and for MIS CDH repair 129.7 minutes (42–161). This result has no statistical significance for duration of surgical time between the two main approaches (P = .4514; Table 4).
A high statistical significance occurred for the use of diaphragmatic patches among open CDH repairs compared to MIS repair with a 35.4% increase in usage, across 28 articles analyzed (55.4% versus 19.6%, P ≤ .00001). Only 250 MIS patients required a diaphragmatic patch repair compared to 2732 open repair patients (Table 4).
The mortality rate following an open CDH repair was 16.6% (1243/7488) compared to 4.6% (81/1761) for an MIS approach (P < .0001).
A chylothorax occurred postoperatively in 8 and 9 patients undergoing MIS and open repairs, respectively. Chylothorax was only represented in three studies. The comparison of MIS and open approaches showed no statistical significance between the formation of chylothorax during the postoperative period (5.9% versus 11.7%, P = .1876).
Limited evidence was observed within studies regarding postoperative ECMO, which was only noted in four articles. An increase of 3.3 times was seen for ECMO use postoperatively in open repair compared to MIS repair, 12.3% versus 3.7% (P = .00001).
Discussion
A CDH is the underdevelopment of the diaphragm leading to an abnormal defect through which abdominal contents could herniate into the thorax. Since its first report by Silen et al in 1995 45 and the successful use of the thoracoscopic approach by Liem et al among a small cohort in 2003, its safety and feasibility, in conjunction with minimal trauma and early recovery for neonates and infants, have been highlighted. 46 Traditional invasive surgical management by laparotomy should be reviewed.
Nearly two decades on and evident within this review, the use of MIS repair is still restricted and only seen sparingly compared to an open repair. The articles within this systematic review have been able to depict the advantages and disadvantages of these approaches in a sufficient manner, to ensure that the most appropriate procedure is put into practice that improves both patient morbidity and mortality. MIS repair has been shown to have lower rates of mortality, decreased ECMO use postoperatively, reduced diaphragmatic patch usage, and a shorter duration of hospital stay postoperatively. However, increased rate of recurrence has been associated with MIS repair compared to open repair.
Our findings showed a six-fold increase in recurrence for MIS CDH repair at a mean rate of 8.6% versus 1.4% for open CDH repair. These findings among the publications lie within the reported range of MIS recurrence rates for CDH repair between 5% and 23.1% 17 versus 0%–13% for open repair. 47 The range of those undergoing MIS approach was shown to be between 0% and 35.3%. As previously theorized high recurrence incidences in MIS may be attributable to the substantial learning curve in technique and proficiency with a limited working space for the procedure, which inevitably diminishes the ability to use a patch or mobilize the posterior diaphragmatic rim to achieve a sufficient muscular repair.17,37,48–51 Interestingly, this systematic review demonstrates that the recurrence rate following MIS repair was lower in the more recent publications compared to the earlier publications (Table 3), which reinforces the learning curve needed to gain proficiency with this technique.
Research has shown the advantage of sandwich-type buttress repair with bovine pericardium underlay and Marlex mesh overlay for both type A and B defects in MIS repair. Double-layer patch of Gore-Tex underlay and Marlex overlay for type C and D defects can improve the recurrence risk in MIS repair, in parallel with improved surgical technique.52,53 Surgeons previously suggested extra ports for thoracoscopic surgery for content reduction while suturing and knotting. He et al have shown knot-tying technique with a combination of a granny knot and modified surgeons knot for MIS approach with no conversion to open or recurrence at 13.7-month median follow-up. 32 In contrast with another review, MIS repair of recurrent CDH does not relate to noteworthy sequelae. 53 To improve surgical knowledge and proficiency to reduce recurrence risk, incorporation of surgical knot technique in combination with a patch repair should be analyzed through large, randomized control trials.
A reduced length of hospital stays for patients undergoing an MIS approach compared to an open repair has been seen (19.6 days versus 33.6 days) with an average difference of 14 days. In comparison, further studies have shown that thoracoscopic repair patients remained more stable with less postoperative mechanical ventilation reduction and a shorter period of antibiotic use leading to shortened hospitalization. 54 It is feasible that those undergoing MIS approaches are selected based on the type of defect, typically A and B, which could introduce bias in affording the MIS approach to more favorable postoperative outcomes. 55
No statistical significance was evident between MIS and open repair for operative time (129.7 minutes versus 119.2 minutes). Criticism for MIS repair has been historically related to prolonged operative times compared to the open approaches, attributable to the learning curve for the surgical technique, surgical preparation, and demanding nature of the surgery. 42 It seems that a correlation between surgical familiarity can decrease operative time and could have contributed to the nonstatistical significance present within this review. 17 Improvement in suturing skill may reduce closure time and could show substantial decrease in patch repair that has demonstrated to have higher rates of operative times within studies, related to the complexity in MIS approaches. 36
Open repair saw a 35.4% increased usage of diaphragmatic patches compared to MIS approaches. This may be due to the fact that type C and D defects are more likely to undergo an open repair due to the difficulty of thoracoscopic CDH repair with a patch. Hence the selection bias may be a cofounding factor in disparity of patch use in open versus MIS approaches. 56 Abello et al newly hypothesized self-expandable novel patch has proven to be successful in repairing type C and D defects while reducing the operative time. 57 Progressive surgical techniques could divert the need for surgical conversion of MIS to open repair when encountering difficulties with closure.
Open repair patients were shown to have a higher mortality rate compared to patients undergoing MIS repair (16.6% versus 4.6%). A recent study analyzing postopen repair mortality over 1 year showed a 7% mortality rate with 0% among MIS approaches. 58 Putnam et al showed a staggering increase in open repair mortality occurring in 446/2579 (17.3%) patients compared to 13/488 (2.7%) MIS repair patients. 42 Chaudhary et al demonstrated that the relationship between open repair and mortality could be due to adverse outcomes secondary to moderate-to-severe PPHN, higher ventilatory demand, reduced Apgar score at 5 minutes, and shock. 56 MIS approach has been limited to stable patients with less comorbidities hence a selection bias of less complex patients undergoing MIS repair. 15 A randomized controlled trial would be beneficial to remove these selection biases from studies.
In the review only three studies included the rate of chylothorax development postoperatively among both approaches, with no significant difference noted. A recent publication identified the presence of a hernia sac, present in 20% of cases as a risk factor for chylothorax alongside direct trauma to lymphatic vessels as identified in multiple studies. Conservative management has been shown to be the first-line option in these cases.59,60 The presence of a hernia sac was not analyzed within this review, making it difficult to comment further on this variable.
Open repair had 3.3 times more patients using ECMO postoperatively but was only included in three studies and shown to be rarely reported unlike perioperative ECMO use. Low postoperative ECMO use for MIS approach seems to be attributed to contraindications of this approach when patients need ECMO preoperatively and during surgery. In contrast, those critically ill patients using ECMO can be repaired open, contributing to the rise of potential ECMO use postoperatively in this group. 61
Previous problems with MIS approach have surrounded surgical preference. Enhanced surgical technique improves with experience, and technique refinement can decrease operative time. It can shift surgical preference to MIS repair over open repair, to potentially reduce mortality rates seen with open CDH repair. 13
Limitations for the systematic review relate to the inability to eliminate selection bias within individual studies with the need for multicenter randomized control trials. Minimal sample sizes and not all outcomes being measured were seen within selected articles. MIS surgical conversion and direct surgical approach comparisons were not reviewed.
Conclusion
After analysis of MIS and open CDH repairs within this systematic review, the MIS approach was shown to be associated with reduced length of hospital stay, reduced mortality rate, and lower rates of postoperative ECMO usage, compared to the open repair. These results may be attributable to a selection bias, with more physiologically stable patients undergoing MIS repair compared to an open repair. Therefore, it is difficult to state categorically that the MIS approach is the independent factor for better outcomes.
However, MIS CDH repair is associated with higher recurrence rates across the analyzed publications. It is evident with the rise of diaphragmatic patch use; surgeon proficiency and surgical suturing technique can reduce recurrence outcomes among patients. A multicenter, randomized control trial should be undertaken to provide detailed analysis to compare these two surgical approaches for CDH repair.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.