
Abstract
Objective:
Three-port laparoscopic radical cystectomy (LRC) is a novel method of radical cystectomy, which is being spread by our team in primary hospitals in our country. The purpose of this study was to evaluate the learning curve of urologists using this technique for bladder cancer patients.
Methods:
We retrospectively evaluated clinical data from patients with bladder cancer who received three-port LRC with urinary diversion at our medical center between January 2018 and December 2021. Consecutive cases were grouped according to different surgical years, and perioperative parameters among groups were assessed as variables for the learning curve, including operative time, estimated blood loss (EBL), lymph nodes (LN) yield, and postoperative hospital stay.
Results:
We assessed 154 patients who were divided into three groups, all of which were comparable in terms of preoperative characteristics. With the increase in surgical experience, the operation time of urologists is obviously reduced (P < .05), especially after 100 surgeries, whereas no statistically significant difference was observed in terms of EBL, LN yield, and postoperative hospital stay in the different surgical experience groups (P > .05).
Conclusions:
Our early learning curve experience indicates that the three-port LRC with urinary diversion is a safe and feasible technique that can be mastered by urologists after learning from a large sample. Given its advantages in cost and significantly improved learning curve, we recommend this technique to surgeons with extensive laparoscopic experience.
Introduction
In recent years, the incidence of bladder cancer has been increasing worldwide due to changes in environment and lifestyle. A surgical procedure has remained the primary treatment for bladder cancer patients despite advances in immunotherapy. 1 Radical cystectomy and urinary diversion remain effective surgical treatments for nonmetastatic muscle-invasive and high-risk nonmuscle-invasive bladder cancer, including open radical cystectomy (ORC), laparoscopic radical cystectomy (LRC), and robot-assisted radical cystectomy (RARC).2,3 In the past 20 years, RARC and LRC have been increasingly used for the surgical treatment of bladder cancer as a viable alternative to traditional ORC due to similar surgical outcomes and prognoses. 4 LRC and RARC are low complication rates and rapid postoperative recovery. 5
However, RARC mainly exists in some large medical centers, and its application is limited by the huge cost and steep learning curve. 6 So far, LRC remains important for the treatment of bladder cancer and is widely performed in primary medical centers.
In China, traditional LRC is still the mainstream surgical approach, which also occurs in most developing countries. Conventional LRC usually needs five or four ports and a 4 to 7 cm abdominal incision for specimen retrieval. With the development of laparoscopic surgery, urologists have begun to explore minimally invasive surgery, mainly involving fewer abdominal incisions and better cosmetic outcomes. Our team has designed an improved three-port technique to minimize the number of ports. 7 Compared to the conventional LRC (using five ports), the three-port approach reduces the number of incisions, overcome the influence of assistants and major equipment, and decreases treatment costs. 8 Nevertheless, there is a lack of data to evaluate improvement in surgical experience during the learning curve for three-port LRC surgeons. In this study, we aim to evaluate the learning curve and surgical results of three-port LRC in bladder cancer patients and to popularize our surgical technique.
Methods
Ethical approval for the study was obtained from the Research Ethics Committee of the Second Affiliated Hospital of Anhui Medical University. Our study retrospectively analyzed the clinical data of bladder cancer patients who received three-port LRC combined with urinary diversion in our medical center from January 2018 to December 2021 and evaluated the relationship between surgical experience and perioperative results.
The inclusion criteria included the following: (1) all patients were diagnosed with muscle-invasive bladder cancer or high-grade nonmuscle invasive bladder cancer by cystoscopy or transurethral resection of bladder tumor (TUR-BT) preoperatively, (2) it was operated by a single surgeon (Dr. L.B.) and a scope assistant, (3) the operation was completed only by three trocars, and (4) no additional trocar was added during the procedure. The exclusion criteria included the following: (1) medical records and perioperative data were incomplete, (2) patients with previous major abdominal surgery, and (3) perioperative death of patients.
A total of 154 of these patients met the eligibility criteria for our analysis of the learning curve. We reviewed the patient demographics, including gender, age, body mass index (BMI), American Society of Anesthesiologists (ASA) grade, neoadjuvant chemotherapy, clinical tumor stage, TUR-BT history, and operative and oncologic outcomes. All procedures were performed by an experienced laparoscopic surgeon (Dr. L.B.), including LRC, pelvic lymph node (LN) dissection, and urinary diversion, with surgical approaches that have been reported in previous studies.8,9 Position of the trocars and incisions for three-port LRC in Figure 1.

Cannula distribution and surgical incision in three-port surgery.
All patients were assigned to group A (surgery in 2018), group B (surgery in 2019), and group C (surgery in 2020 and 2021) based on the year of surgery. There were 51 cases in group A (33.12%), 51 cases in group B (33.12%), and 52 cases in group C (33.76%). To evaluate the learning speed of the three-port surgery, operative time, estimated blood loss (EBL), LN yield, and postoperative hospital stay among groups was assessed as variables for the learning curve.
Statistical analysis was performed by R software (version 4.04). LOWESS curve and box plot was drawn by the ggplot2 package. 10 Classified variables are expressed as frequency and percentage, and continuous variables are expressed as average standard deviation. Fisher's exact test and χ 2 test is performed to study the relationship between variables. Pearson correlation analysis was used to determine the relationship between groups, and Kruskal–Wallis was used to verify the statistically significant differences among groups. All P values were two-sided, with P < .05 indicating statistical significance.
Results
In general, we evaluated 154 patients with bladder cancer treated by urologists in our center from 2018 to 2021 using the “three-port” LRC method. Table 1 summarizes patient characteristics and demographics in detail. There were no significant differences in preoperative characteristics among the three surgical experience groups, except for patients receiving neoadjuvant chemotherapy. As for gender, age, BMI, ASA grade, clinical tumor stage, and TUR-BT history, such data were comparable without significant difference.
The Preoperative Demographics of 154 Patients According to Surgical Experience Group
Signifcant P values are shown in bold.
ASA, American Society of Anesthesiologists; BMI, body mass index; TUR-BT, trans urethral resection of bladder tumor.
Of the 154 patients, 69 patients underwent ileal conduit, 54 patients received neobladder, and 31 patients were treated by cutaneous ureterostomy. Operative and oncologic outcomes were shown in Table 2. There were no serious complications during the operation. The mean operative time in the three surgical experience groups was 288.78 ± 55.52, 277.10 ± 52.40, and 261.73 ± 48.33 minutes, respectively (P < .016, Fig. 2A). The median EBL in the three groups were 80 (40–300) mL, 100 (40–300) mL, and 50 (30–300) mL, respectively (P < .82, Fig. 2B). The median LN yield in the three groups were 22 (8–37) LN, 20 (7–37) LN, and 17 (8–35) LN, respectively (P < .27, Fig. 2C).

Comparison of perioperative results for three-port LRC among different groups, including
The Operative and Oncologic Parameters of 154 Patients According to Surgical Experience Group
Signifcant P values are shown in bold.
LN, lymph nodes; PSM, positive surgical margins.
The median postoperative hospital stay in the three groups were 14 (8–28) days, 12 (7–26) days, and 11.5 (7–26) days, respectively (P < .066, Fig. 2D). Ten patients had positive surgical margins (PSM) because their tumors were large and malignant. Adjuvant chemotherapy was used for patients with postoperative pathological outcomes above T2b.
The LOWESS curve showed that the operative time decreased in surgical experience, but no significant difference with EBL, LN yield, and postoperative hospital stay (Fig. 3A–3D). Unfortunately, this method cannot provide a coefficient, unable to explain the internal relationship between variables. Pearson correlation analysis showed a negative correlation between surgical experience and operating time (P < .001, R = −0.256), but no significant correlation with EBL (P = .457, R = −0.06), LN yield (P = .055, R = −0.18), and postoperative hospital stay (P = .313, R = −0.082). With the increase in surgical experience, the operation time of urologists is obviously reduced, whereas no statistically significant difference was observed in terms of EBL and oncologic outcomes in the different surgical experience groups.
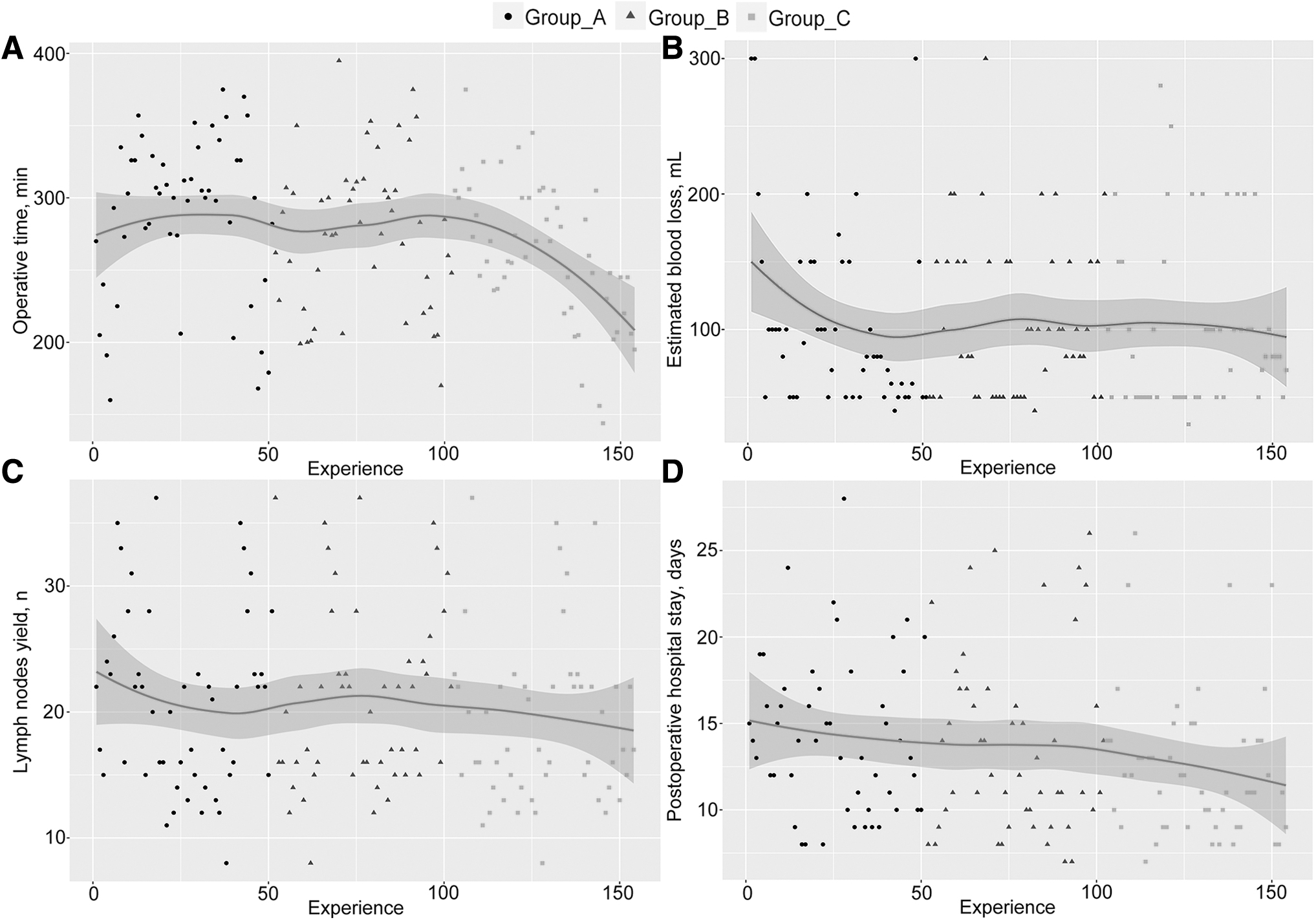
A learning curve of three-port LRC by comparing the parameters among different groups, including
Discussion
In 1992, Parra et al 11 applied laparoscopic technique to treat bladder pyometra, and since then, LRC and urinary diversion have been widely spreading.4,12 With the advent of the Da Vinci robot system, RARC is widely used in many developed countries as the most common surgical treatment for bladder cancer.2,13 There is a general consensus that RARC or LRC have similar outcomes to ORC in terms of complications, but with less bleeding and shorter hospital stays.14–16 Due to the steep learning curve and high cost, the application of RARC in medical centers in most areas is extremely limited, and the standard laparoscopic technique continues to be implemented, especially in hospitals in China.
With the advancement of minimally invasive surgery, urologists are aware of the limitations of traditional LRC techniques, especially the need for 3 or 4 surgeons to perform the procedure, which undoubtedly increases the difficulty and cost of this technique. To minimize the incision, urologists reported the initial experience using single-port and two-port LRC techniques for the treatment of bladder cancer.17,18 However, because surgical incisions are concentrated at one site, the range of movement of surgical instruments is limited, which can cause crowding and clashing in a narrow surgical space. To overcome these limitations, our team modified the traditional LRC technology, which requires only a surgeon and a scope assistant to perform the surgery.
This novel technique can be used for ileal conduit or neobladder,8,9 and the removal of specimens via the vagina means the perfect minimally invasive treatment for female patients. At short-term follow-up, our three-port technique proved feasible, with similar surgical and tumor outcomes compared to conventional LRC techniques, but at a lower cost of treatment.
The learning curve refers to the process of a surgeon's learning practice in a minimally invasive procedure, from initial practice to gradual reduction of complications to eventual mastery of the procedure. 19 Learning curve analysis can guide urologists to learn and master the three-port LRC, but this may be different from individual to operation. In the current study, we attempted to assess the learning curve of the three-port LRC and the impact of various factors. The results showed that with the increase in the number of cases, the operation time decreased significantly, and surgeons can break the learning curve bottleneck in the 100th case.
The three-port technique requires the surgeon to make full use of the left hand instead of the first assistant, to realize the unification of surgical steps and operations, and the operation is repeatable and easy to master and popularize the technique. 7 As surgeons became familiar with anatomy and muscle memory, operative time decreased significantly. However, the efficacy and complications of bladder cancer patients with pelvic stenosis, malformation, vascular variation, and other pelvic abnormalities that cannot fully expose the pelvic space remain to be summarized by long-term large sample data. In this study, our three-port LRC achieved surgical and oncological results comparable to those of the published conventional LRC series in most parameters.12,20
On the learning curve of specific surgery, surgeons need to consider not only the relationship between the operation time and the number of cases, but also some relevant surgical indicators, including EBL, LN yield, and postoperative hospital stay. Several previous reports on the RARC learning curve have shown no significant association between the consecutive cases and complications, EBL, PSM, and survival.21,22 With experience, bleeding improved and then remained stable. Oncology results seem to be of greater importance for mastering the learning curve. Our results suggest that PSM rates and LN yields remain relatively stable across the surgeon's learning curve. Moreover, the correlation between length of stay and continuous cases was not significant, mainly because there were many influencing factors.
Urinary diversion is the most important component of surgical treatment of bladder cancer because postoperative complications are closely related to the type of shunt, including ileal conduit, neobladder, and cutaneous ureterostomy. 23 The effect of ileal conduit on intestinal function is slight, and postoperative recovery is quick. Urine has a relatively short retention time in the ileal bladder, reducing the incidence of complications. Orthotopic neobladder allows patients to urinate autonomically and improves their quality of life, but it carries risks such as potential retrograde infection. Cutaneous ureterostomy is a salvage procedure that is often recommended for patients with advanced or elderly tumors. 24 All three types of urinary diversion combined with three-port LRC can successfully complete the treatment of bladder cancer patients, and the outcome have been reported in our previous study.8,9
There are several limitations to our study that need to be addressed. First, the data were collected retrospectively, so the results were affected by selection bias. Second, we did not report the complications of these procedures in detail, because different types of urinary diversion can affect the incidence of complications. Third, we need further studies to confirm the clinical relevance of these findings.
Conclusion
Three-port LRC with urinary diversion is a complex procedure, but it can be safely performed by the surgeon using a structured method in an established high-volume laparoscopic center without affecting perioperative and pathological outcomes. Given its advantages in cost and significantly improved learning curve, we recommend this technique to surgeons with extensive laparoscopic experience.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The present study was supported by the Clinical Research Cultivation Program of The Second Affiliated Hospital of Anhui Medical University (Hefei, China; grant nos. 2020LCZD03; 2021LCZD04).