
Abstract
Introduction:
Portal hypertension is a syndrome characterized by increased pressure in the portal vein system and can be caused by impaired blood flow in the portal vein, hepatic veins, or inferior vena cava. The main complications of this condition are bleeding from varicose veins of the esophagus (in our study in 100% of patients), splenomegaly with hypersplenism (in our study in 98% of patients), ascites (in our study in 1 patient). The main goal of treating portal hypertension is to prevent bleeding from esophageal varices. However, today the goal of surgical treatment of portal hypertension in children is not only to prevent the development of bleeding but also the possible restoration of intrahepatic blood flow.
Materials and Methods:
A retrospective analysis of the results of treatment of portal hypertension in 75 children (41 boys, 34 girls) operated in our Center for the period from 2019 to 2022 was carried out. The mean age of the patients was 7 ± 1 years. Sixty-nine patients had an extrahepatic form of portal hypertension, and 6 patients had an intrahepatic form (liver fibrosis). In 14 patients (18.6%), the operation was repeated (a vascular shunt was previously applied in another hospital; 4 children were operated on repeatedly).
Results:
A good result was obtained in all children, and the risk of bleeding from varicose veins of the esophagus was eliminated. Vascular bypass surgery was performed in all cases: mesoportal bypass in 17 (22.7%) patients, splenorenal bypass in 37 (49.3%) patients, mesocaval bypass in 21 (28%) patients. In 10 (13%) cases, repeated bypass surgery was required due to dysfunction or thrombosis of the previously performed bypass. In 14 (18.6%) patients with mesoportal shunts, blood flow in the liver was completely restored.
Conclusions:
The main method of surgical treatment of portal hypertension today is portosystemic bypass surgery, which effectively prevents bleeding from varicose veins of the esophagus. Mesoportal shunting is a definitive treatment for extrahepatic portal hypertension that restores portal perfusion of the liver.
Introduction
Portal hypertension is a syndrome characterized by increased pressure in the portal vein system and can be caused by impaired blood flow in the portal, hepatic, or inferior vena cava. In children, unlike adults, the main cause of this condition is the obstruction of blood flow through the portal vein due to its thrombosis or malformation. The subhepatic form of portal hypertension in children is a severe pathology that requires active treatment from early childhood due to a significant number of severe complications. 1 The main complications of this condition are bleeding from varicose veins of the esophagus (in our study in 100% of patients), splenomegaly with hypersplenism (in our study in 98% of patients), ascites (in our study in 1 patient). The most dangerous complication is bleeding from varicose veins of the esophagus and stomach. According to the literature data, in more than half of the cases, the first bleeding occurs before the age of 7 years.
According to our observations, bleeding before surgical treatment was observed in 30% patients. 1 The main goal of surgical treatment of portal hypertension is to prevent bleeding from varicose veins of the esophagus; however, today, due to the widespread introduction of portosystemic bypass operations into the practice, the question of the possibility of restoring normal intrahepatic blood flow remains extremely important. Currently, in connection with the emergence and introduction of endoscopic sclerosis techniques into pediatric practice, the question of the optimal management of pediatric patients with portal hypertension also remains debatable. 2
Materials and Methods
A retrospective analysis of the results of treatment of portal hypertension in 75 children (41 boys, 34 girls) operated in the surgical thoracic department of the National Research Center for Children's Health of the Ministry of Health of Russia for the period from 2019 to 2022 was carried out. All patients in our study underwent portosystemic shunting. The mean age of the patients was 7 ± 1 years. Sixty-nine patients had an extrahepatic form of portal hypertension; 6 patients had an intrahepatic form (liver fibrosis). In 14 patients (18.6%), the operation was repeated (a vascular shunt was previously applied in another hospital, 4 children were operated on repeatedly). In 4 patients, endoscopic sclerosis of varicose veins of the esophagus was previously performed (at the place of residence).
As a preoperative examination, all patients underwent an ultrasound examination of the abdominal organs with Dopplerography, as well as Dopplerography of the neck vessels (to assess the possibility of using the jugular vein as an autovenous insert), angiography to assess the angioarchitectonics of the vessels of the portal system and a preliminary assessment of the possibility of performing portosystemic shunting, fibroesophagogastroduodenoscopy to assess the degree of varicose veins of the esophagus, and laboratory examination to assess the presence and severity of hypersplenism and coagulopathy. The above examination was also carried out as a control examination to assess the effectiveness of treatment. We have the approval of LIEC (local independent ethics committee).
Surgical treatment technique
REX shunt
The operation was performed under conditions of combined endotracheal anesthesia and epidural analgesia. At the stage of the beginning of the formation of a vascular shunt, low molecular weight heparin was administered at a dose of 100 U/kg. The average time of surgical intervention was 90 ± 15 minutes. A median laparotomy was performed. In the course of the round ligament of the liver, a revision of the left branch of the portal vein was made, if it was patency, a clamp was applied to the vein, then the superior mesenteric vein was isolated. An incision in the neck (more often on the left, in the presence of patency of the internal jugular vein according to Doppler data) was used to isolate the internal jugular vein and remove it as an autovenous insert for anastomosis formation. A continuous vascular anastomosis was sequentially applied between the autovenous insert and the superior mesenteric vein, then the autovenous insert and the left branch of the portal vein. Anastomoses were formed using Prolene 7/0–8/0 thread. The diameter of the anastomosis was 1.0–1.5 cm. Thus, the “REX-shunt” was performed (Fig. 1).

Meso-portal “REX-shunt” in a 7-year-old child.
Spleno-renal shunt
In cases of obliteration of the left branch of the portal vein, its lumen was sutured, then the splenic vein was inspected along the posterior-inferior edge of the pancreas. If it was passable and of sufficient diameter, the renal and adrenal veins were isolated, and the vessels were clamped with clamps and a spleno-renal anastomosis was formed side-to-side (31 patients) or spleno-suprorenal (6 patients) without the use of an autoinsert (Fig. 2). The diameter of the anastomosis was 0.8–1.0 cm.

Spleno-renal shunt.
Mesenteric-caval shunt
If it was impossible to perform a spleno-renal anastomosis, a mesenteric-caval anastomosis was performed in the form of an H-shunt or side-to-side with sufficient vascular mobility. The superior sternal and inferior vena cava veins were sequentially isolated, and in case of approach of the vessels without tension, a side-to-side vascular shunt was performed; veins (Fig. 3).

Mesenteric-caval H-shunt.
Results
A good result was obtained in all children, and the risk of bleeding from varicose veins of the esophagus was eliminated. Vascular bypass surgery was performed in all cases: mesoportal bypass in 17 (22.7%) patients, splenorenal bypass in 37 (49.3%) patients, and mesocaval bypass in 21 (28%) patients.
In 10 (13%) cases, repeated bypass surgery was required due to dysfunction or thrombosis of the previously performed bypass. In 14 (18.6%) patients with mesoportal shunts, blood flow in the liver was completely restored (Fig. 4).
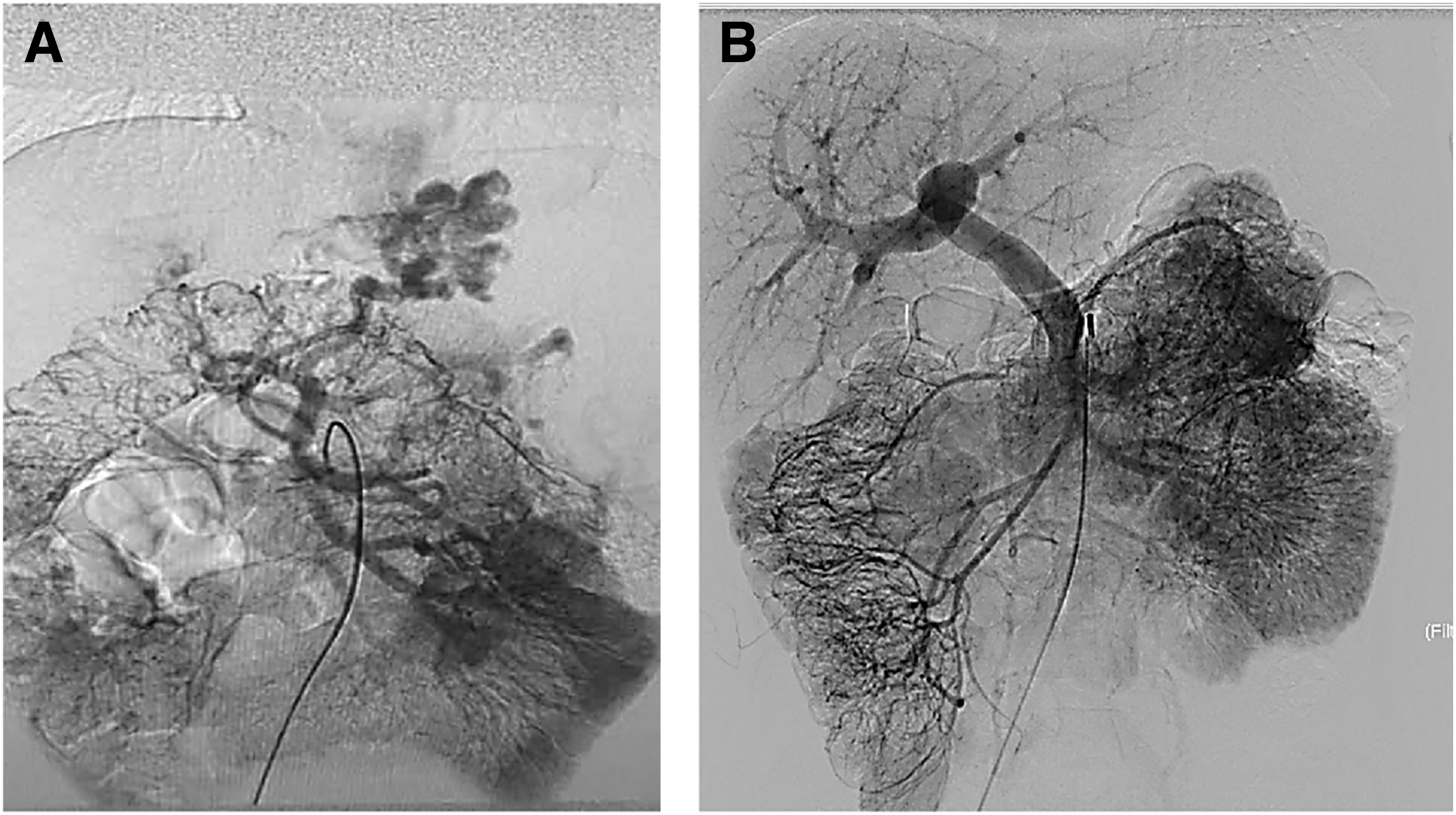
Angiography
Three patients were operated on at the height of bleeding; in patients of this group, vascular bypass surgery was supplemented by endoscopic sclerosis of esophageal varicose veins.
Complications in the early postoperative period were noted in 4 patients (5%): 2 patients had bleeding into the abdominal cavity, which required emergency surgical treatment; 2 patients had bleeding from the place where the autovenous insert was taken. There were no complications from the postoperative wound.
In the early postoperative period, 12 patients (16%) had complete disappearance of esophageal varicose veins.
In all patients, after the application of REX-shunt, parents noted improvements in attention, learning, and general condition, and children achieved great success in their studies. It should also be noted that in children after REX-shunt, the average blood flow velocity in the anastomotic area was 35 cm/s, which practically corresponds to the norm of blood flow in the portal vein in healthy children (29 cm/s). In children, after the application of spleno-renal and meso-qual bypass shunts, the average blood flow rate was 40–45 cm/s, while the blood flow through the hepatopetal collaterals practically stopped.
Discussion
Over the past decades, the possibilities and principles of surgical treatment of portal hypertension in children have changed significantly.
The main reason for the development of portal hypertension in children is the obstruction of the portal vein, either due to thrombosis or as a variant of the malformation. These conditions suggest complete preservation of liver function, in contrast to adults who develop liver failure due to cirrhosis of the liver.3,4 This condition provides a favorable long-term prognosis for life, provided that the threat of bleeding from varicose veins of the esophagus in children is eliminated. 5
If a child has a history of bleeding from varicose veins of the esophagus, the question of indications for surgical treatment is not the subject of discussion. However, in the absence of a threat of bleeding from varicose veins of the esophagus, in the event that portal hypertension manifests itself as hypersplenism, splenomegaly, the question of indications for surgical treatment remains debatable. In our observation, the proportion of such patients was 18%. Performing vascular shunts in this category of patients allows for the prevention of bleeding from esophageal varices, which is especially important if the patient lives in a remote region where access to specialized medical care is difficult.6,7
To date, portosystemic bypass surgery is the most effective treatment for children with portal hypertension, which eliminates the risk of bleeding from esophageal varices. 4 In our observation, in 87% of cases after the first operation, it was possible to achieve complete control over bleeding. After repeated intervention, complete control over bleeding was achieved in 100% of cases.
An undoubted breakthrough in the surgical treatment of portal hypertension in children was the operation of applying a mesoportal shunt REX-shunt, which allows not only to prevent the development of bleeding from esophageal varicose veins but also to completely restore portal blood flow. In our observations, this type of surgical treatment was performed only in 22.7% of patients. This fact is probably associated with a higher frequency of umbilical vein catheterization in developing countries, as well as with a higher incidence of infectious complications such as omphalitis and sepsis. Undoubtedly, this type of surgical treatment is the most preferable, but not always feasible.1,8
Conclusion
Thus, based on the experience of our observations, we can draw the following conclusions: the main method of surgical treatment of portal hypertension today is portosystemic bypass surgery, which effectively prevents bleeding from varicose veins of the esophagus. Mesoportal shunting is a definitive treatment for extrahepatic portal hypertension that restores portal perfusion of the liver.
Footnotes
Acknowledgments
With great gratitude to the director of our Scientific Center, Professor Andrey Fisenko, for the opportunity to conduct and combine our practical work and scientific research for the benefit of the children's population.
Authors' Contributions
A.A.: Conceptualization, methodology. E.K.: Resources, provision of patients, participation in surgery and data collection. S.R.: Resources, provision of patients, participation in surgery, and data collection. M.S.: Writing—original draft. E.R.: Resources, provision of patients, participation in surgery, and data collection. A.G.: Data curation, writing—original draft preparation. M.L.: Resources, provision of study materials, patients, instrumentation, and computing resources. S.Y.: Supervision. E.D.: Resources, provision of patients.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.