
Abstract
Background:
Common bile duct (CBD) stones associated with cholecystitis can be treated by single-stage CBD exploration at the time of cholecystectomy or a two-stage approach with endoscopic stone extraction before or after cholecystectomy. The ideal management remains a matter of debate. The aim of this study is to analyze our outcomes with transcystic laparoscopic common bile duct exploration (LCBDE).
Material and Methods:
A retrospective review of patients who underwent transcystic LCBDE between 2015 and 2019 was performed.
Results:
A total of 106 patients underwent transcystic LCBDE over 5 years. We performed 1192 laparoscopic cholecystectomies with cholangiograms from March 2015 to December 2019. Fifteen patients had a preoperative endoscopic retrograde cholangiopancreatography (ERCP) for CBD stones seen on magnetic resonance cholangiopancreatography that during laparoscopic cholecystectomy with intraoperative cholangiogram (IOC), there were stones and/or sludge found in the CBD, which required clearance through a transcystic approach. Of the 91 patients who did not have a preoperative ERCP, clearance of the CBD was successful through a transcystic approach in 78 patients (86%). In the 13 patients that intraoperative clearance was not achieved (n = 13, 14%), a postoperative ERCP was performed. A total of 28 patients underwent either pre- or postoperative ERCP (n = 28, 26%). Choledochotomy was not performed in any of the patients. The mean operative time was 127 minutes (127 ± 48). The mean hospital length of stay (LOS) was 4 days (3.9 ± 2.8) with a median LOS of 3 days. Complications observed include wound infection (n = 2, 2%), pancreatitis after ERCP (n = 1, 1%), pneumonia (n = 1, 1%), and right hepatic duct injury (n = 1, 1%).
Conclusion:
Transcystic LCBDE is an effective and safe option for treatment of CBD stones. While a transcystic approach does not guarantee clearance of the CBD, it avoids the morbidity associated with a choledochotomy and can often prevent patients from having to undergo an additional procedure.
Introduction
Cholecystectomies are one of the most common surgeries performed in the United States with over 750,000 performed per year, at a cost to the health care system of U.S. $6.5 billion. 1 It is estimated that 10%–20% of patients with cholelithiasis have common bile duct (CBD) stones and this increases to 33% in patients with biliary pancreatitis.2–4 Incidentally found choledocholithiasis in patients with normal liver function tests (LFTs) and normal CBD size on preoperative imaging is reported as 3%–7%. 5 Often choledocholithiasis is managed with a two-stage procedure beginning with preoperative stone extraction through endoscopic retrograde cholangiopancreatography (ERCP) followed by laparoscopic cholecystectomy during the same hospitalization. However, as surgeons become more experienced in laparoscopic procedures, single-stage laparoscopic common bile duct exploration (LCBDE) is becoming more common. 6 The optimal management of CBD stones remains debated, yet the aforementioned procedures are the two most common methods used to treat CBD stones.6,7
Given the routine use of intraoperative cholangiogram (IOC), we are able to identify and treat choledocholithiasis at the time of surgery. In this retrospective study, we aim to evaluate our experience with transcystic LCBDE. Primary outcomes include success in stone extraction and clearing of the CBD. Secondary outcomes were length of stay, number of procedures, and complications.
Materials and Methods
All cases performed at our institution follow the six-step SAGES protocol for safe laparoscopic cholecystectomy that includes an IOC. 8 This study was approved by the Institutional Review Board (IRB) at Mount Sinai Medical Center. All patients who underwent laparoscopic cholecystectomy with cholangiography with CBD exploration (CPT code 47564) were retrieved from our Electronic Medical Record between March 2015 and December 2019. We performed 1192 laparoscopic cholecystectomies with cholangiography (CPT code 47563) during the same period. Patients were included for analysis if they underwent transcystic LCBDE.
Patient selection
Patients who presented with acute cholecystitis underwent routine preoperative work-up, including a complete history and physical examination and blood work, including a complete blood count, hepatic profile, basic metabolic panel, and coagulation profile. All patients had a preoperative abdominal ultrasound. When patients presented with an elevation in the direct bilirubin, magnetic resonance cholangiopancreatography (MRCP) was performed to assess for choledocholithiasis. Preoperative ERCP was performed in patients when choledocholithiasis was visualized on MRCP. Transcystic LCBDE was performed in all patients whose IOC revealed stones or debris in the CBD, or otherwise abnormal passage of contrast into the duodenum.
Statistical analysis
Data are expressed as n, percentage or as the mean ± standard deviation. Data were analyzed using Microsoft Office Excel (Microsoft, Redmond, WA, USA).
Operative technique
Procedure is performed with the patient in the supine position, arms tucked in mild reverse Trendelenburg and right side up. A standard four-port laparoscopic cholecystectomy with cholangiogram was performed on all patients. The cholangiogram is performed using an Olsen endoscopic catheter (Cook Medical, Bloomington, IN, USA) through the subxiphoid trocar. A transcystic LCBDE is performed if stones, debris, or lack of filling of contrast into the duodenum are identified on the IOC. A separate, 3 mm right upper quadrant incision is made and the Appel-Berci cystic duct introducer and dilator (Cook Medical) are advanced into our cystic ductotomy. A hydrophilic coated 0.035 glidewire (Terumo Medical, Somerset, NJ, USA) is then passed under fluoroscopic visualization into the duodenum. One milligram of glucagon is administered intravenously. Depending on the size of the CBD and based on surgeon discretion, either a 6 or 8 × 40 mm percutaneous transluminal angioplasty Balloon Dilatation Catheter (Boston Scientific, Marlborough, MA, USA) is used to dilate the ampulla.
An Encore 26 high-pressure insufflation device (Boston Scientific) is used to dilate the ampulla. The balloon is inflated for 1 minute at the level of the ampulla, with the purpose of dilating it and further facilitating passage of the stones, then deflated and repositioned in the cystic duct and reinflated. Several vigorous flushes with saline are administered and a completion cholangiogram is performed confirming clearance of the CBD.
Representative images from an IOC from a patient with a filling defect at the ampulla and subsequent clearing of the duct using the aforementioned technique can be seen in Figures 1–4. If the CBD is not cleared, we then deflate the balloon and perform several sweeps of the bile duct with the balloon; a completion cholangiogram is repeated. On rare occasions, we use basket retrieval and choledochoscopy for stone extraction. The cystic duct is then occluded with 5 mm clips or an endoloop (Ethicon, Somerville, NJ, USA) and the gallbladder extracted from the abdomen.

Cholangiogram revealing a filling defect at the ampulla.

Cholangiogram with glidewire and balloon placed at the ampulla.
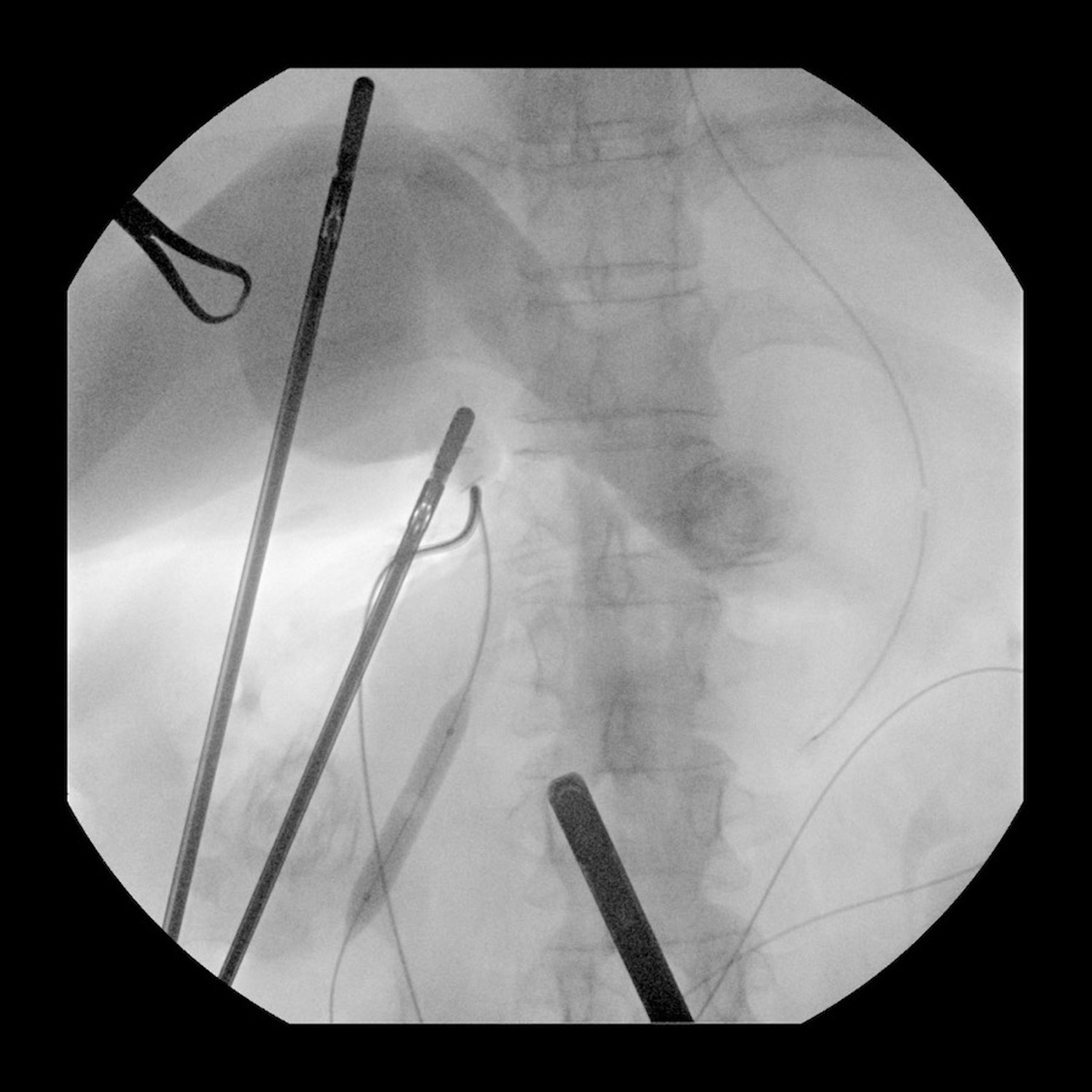
Cholangiogram with inflated balloon at the ampulla.

Completion cholangiogram with contrast flowing freely into the duodenum.
Follow-up
All patients were seen in the outpatient setting approximately 1 week after surgery. No patient was lost to follow-up.
Results
Over a 5-year period, a total of 106 patients underwent transcystic LCBDE. All patients presented with right upper quadrant pain and found to have symptomatic cholelithiasis. There was a predominance of females (64%). The mean age was 58 years (58 ± 18), the average body mass index was 30 kg/m2 (29.5 ± 6), and the mean American Society of Anesthesiologist class was 2 (2.1 ± 0.8). A total of 37 patients (35%) had LFTs, including ALT and AST within the normal range (alanine transaminase [ALT] 13–56 U/L and aspartate transaminase [AST] 13–37 U/L); 63 patients (59%) had a normal total bilirubin (total bilirubin 0.2–1.0 MG/DL). The most prevalent medical comorbidities included hypertension 47 (44%), diabetes mellitus 18 (17%), heart failure 10 (9%), and current tobacco use 8 (8%). Forty-three (41%) patients had prior abdominal surgery. Preoperative patient characteristics are listed in Table 1.
Perioperative Patient Characteristics
ALK, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; WBC, white blood count.
Thirty-nine (37%) patients had an MRCP preoperatively. Of these 39 patients, MRCP confirmed choledocholithiasis in 14 patients (36%). A total of 15 patients underwent ERCP before cholecystectomy when choledocholithiasis was confirmed through MRCP preoperatively or when the index of suspicion was high enough to warrant ERCP without MRCP. Of the 91 patients who did not have a preoperative ERCP, clearance of the CBD was achieved intraoperatively in 78 patients (86%). No choledochotomies were performed. Rather, if intraoperative clearance of the CBD was not possible, then patients underwent postoperative ERCP. Two transcystic LCBDE were aborted due to a friable cystic duct (n = 1) and a necrotic gallbladder (n = 1). A total of 13 patients required postoperative ERCP given inability to clear the common duct intraoperatively through a transcystic approach. In these patients where a transcystic LCBDE failed, the most common reasoning was due to multiple stones, large stones >10 mm, or a small cystic duct <3 mm.
The mean operative time was 127 minutes (127 ± 48). For those patients who underwent a single-stage procedure, the mean hospital length of stay (LOS) was 4 days (3.8 ± 2.9); this is in comparison to those patients who required either preoperative or postoperative ERCP, and whose mean LOS was 5 days (4.9 ± 2.3). Mean LOS was 4 days for two-stage procedure (4.1 ± 2.7) and a median LOS of 3 days for single-stage procedure. These data can be visualized in Table 2.
Mean Operative Time for Transcystic Laparoscopic Common Bile Duct Exploration and Hospital Length of Stay for Patients Undergoing Only Transcystic Laparoscopic Common Bile Duct Exploration (Single-Stage) or Transcystic Laparoscopic Common Bile Duct Exploration in Conjunction with Endoscopic Retrograde Cholangiopancreatography (Two-Stage)
Complications observed include wound infection (n = 2, 2%), pancreatitis after ERCP (n = 1, 1%), pneumonia (n = 1, 1%), and right hepatic duct injury (n = 1, 1%). The patient who sustained a right hepatic duct injury had a chronically diseased gallbladder that distorted the normal tissue planes and precluded dissection of the triangle of Calot, thereby requiring a subtotal cholecystectomy. A cholangiogram was performed using a Foley catheter through the infundibulum of the gallbladder that revealed a large obstructing stone in the distal CBD. A transcystic approach was used to clear the CBD. Postoperatively it was noted that he developed a bile leak and an ERCP revealed an injury to a right sectoral bile duct. We suspect that this likely occurred during the dissection of Calot's triangle. This injury was not identified during the intraoperative cholangiogram and we believe this injury was unrelated to the transcystic LCBDE. This was managed with biliary stent placement on postoperative day 1 through ERCP and subsequent removal 3 months later. There were no mortalities at the 30-day mark and all procedures were completed laparoscopically with no conversions to open surgery.
Discussion
Given that up to 20% of patients who present with cholecystitis have concomitant CBD stones, 2 correct diagnosis and treatment is critical. The Swedish GallRiks trial found high rates of unfavorable outcomes in patients that were found to have CBD stones that were left untreated. 9 There are many options for treating CBD stones, including open CBD exploration, laparoscopic cholecystectomy with pre- or postoperative ERCP and LCBDE. There is no consensus on the optimal strategy for treatment of concomitant CBD. An increasing number of peer-reviewed articles suggest that routine IOC during laparoscopic cholecystectomy helps prevent major biliary tract injuries.10–12 An advantage of routine IOC is accurate diagnosis of concomitant CBD stones at the time of cholecystectomy. While transcystic LCBDE can seem to be technically demanding, it has been demonstrated as a feasible first-choice treatment option for patients with choledocholithiasis.1,13,14 Given that transcystic LCBDE eliminates the need to perform a ductotomy on the CBD, it reduces the risk of CBD stricture and postoperative bile leak. 14
In this study, we present our experience over 5 years in treating choledocholithiasis with LCBDE.
Our success rate of clearing the CBD through a transcystic approach is 86% and this appears comparable to what is reported in the literature, with reported rates ranging from 71% to 95%.13,14 In our experience, favorable conditions for successful transcystic LCBDE include few stones in the CBD (<5), small stones (<10 mm), adequate cystic duct size (>3 mm), and stones distal to the cystic duct–CBD junction. While transcystic LCBDE avoids the morbidity associated with a choledochotomy and the increased length of stay associated with a two-stage procedure, choledochotomy may be necessary when a transcystic approach fails. Our learning curve is ∼10–20 cases with the caveat that performing routine cholangiography helps obtain the skills necessary to perform transcystic explorations under fluoroscopy, which is our preferred route.
We recognize the limitations of our study given that it is retrospective, nonrandomized, and includes a relatively small sample size of patients. Additionally, while cost analysis was not within the scope of this study, future investigations standardizing the usage of transcystic LCBDE and cost-savings analysis would be of use to general surgeons. Our learning curve also improved over the years and we expect that as we continue to gain more experience our success rate will also increase. Establishment of a reliable minimally invasive transcystic approach to acute biliary obstructive disease increases the volume of procedures performed effectively, with lesser risks of complications, lower mortality and readmission rates, and improved hospital costs in the long term.
Conclusion
The results of this study demonstrate that transcystic LCBE is a feasible first-line approach to the treatment of CBD stones. A single-stage procedure can be successful in managing CBD stones thus reducing the LOS, overall costs, and morbidity associated with ERCP. We encourage surgeons performing laparoscopic cholecystectomy to perform routine IOC and develop skills to address CBD stones at the time of cholecystectomy.
Footnotes
Authors' Contributions
J.E.W. and T.W.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, writing—original draft, writing—review and editing.
R.B., K.K., and L.E.R.: Data curation, investigation, writing—review and editing.
J.D., S.W.U., D.J., and I.J.: conceptualization, writing—review, and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.