
Abstract
Background:
The main purpose of this study was to analyze patient-related factors that may influence the risk of hernia recurrence following laparoscopic incisional hernia repair (LIHR), including the potential role of chosen materials.
Materials and Methods:
A multicenter, retrospective cohort study was conducted on all patients who were aged >18 years and who underwent elective laparoscopic incisional hernia mesh repair at the Departments of Surgery of the S. Anna University Hospital in Ferrara and Sassuolo Hospital in Modena, Italy. Exclusion criteria were as follows: patients undergoing an open or emergency incisional hernia repair or with primary ventral hernia. All hernia and operative variables that may favor hernia recurrence were collected and analyzed. Follow-up was conducted through a standardized telephone interview, followed by an outpatient visit and diagnostic imaging if needed.
Results:
From September 2002 to September 2017, 312 consecutive patients underwent elective laparoscopic incisional hernia mesh repair. At a mean 22-month follow-up, 273 patients presented no recurrence of incisional hernia and 39 had relapsed. Intra- and postoperative complications were similar between groups. Unadjusted Cox regression analysis showed a statistically significant association between both the partially absorbable mesh (P < .0001) and absorbable tacks (P = .001) and recurrence, while after adjusting for potential confounders, only the partially absorbable mesh was significantly associated with recurrence (P = .007).
Conclusions:
The laparoscopic approach may be considered safe for incisional hernia mesh repair. In this multicenter, retrospective cohort study, the use of a partially absorbable mesh in LIHR was the only predictor of hernia recurrence. The partially absorbable mesh that was investigated, however, has been withdrawn from the market.
Introduction
Incisional hernias represent one of the most common complications after abdominal surgery and occur in up to 20% of patients following a midline laparotomy. 1 Abdominal wall surgery techniques are increasingly tailored to the wall defect characteristics and patient's health condition. Elective laparoscopic incisional hernia repair (LIHR) is comparable (in terms of safety and efficacy) with the open procedure; in patients with a wall defect of limited size (<10 cm) and few comorbidities, it allows reduction of operating times and institutional costs.2,3
The choice of the best surgical technique is influenced by awareness of its safety and by a balance of the risks related to efficacy; recurrence represents medium- to long-term adverse events that surgeons should consider when planning the hernia repair for each patient.4,5
In a large, registry-based, Danish cohort study on 3242 patients, Kokotovic et al 6 reported most recurrences within 24–36 months, with an average overall follow-up of 5 years. The authors also suggested that with long-term follow-up, the benefits attributable to mesh repair are offset, in part, by mesh-related complications. 6 To date, there is no exact definition of the time in which it is possible to observe a reduction of the diagnostic risk of recurrence during the follow-up after incisional hernia repair.
Patient-related predictors of recurrence are known and similar in the laparoscopic and open techniques: obesity, recurrent hernias, and defect size >10 cm.2,4,7 Technical factors may also be involved in potential recurrence risk and they are related to the mesh type, fixation technique, and overlapping in the surgical defect.
In a systematic review, Khan et al 8 found no differences in clinical outcomes and recurrence rates between absorbable and nonabsorbable tacks, and no differences in mesh types could be detected in a recent meta-analysis of randomized controlled trials (RCTs) investigating surgical and postsurgical outcomes of elective incisional hernia repair by the open versus laparoscopic approach. 9
Among the predictive factors for recurrence, in addition to suitable overlap, the relationship between the mesh area and defect (i.e., mesh-to-defect area ratio, M/D ratio) was identified as a potential predictive factor for recurrence with the choice of LIHR. 10 If a satisfactory M/D ratio cannot be achieved, another surgical repair approach should be proposed to the patient.
The main purpose of this study was to describe our experience by analyzing the patient-related factors that could influence the risk for recurrence and the potential role of chosen materials in the LIHR technique. The secondary outcome was to compare postoperative complications between patients with hernia recurrence and those without hernia recurrence at clinical follow-up.
Materials and Methods
Study design, setting, and participants
A multicenter, retrospective cohort study was conducted on consecutive patients who were aged >18 years and who underwent elective laparoscopic incisional hernia mesh repair from September 2002 to September 2017 at the Department of Surgery of the S. Anna University Hospital in Ferrara and at the Department of Surgery of Sassuolo Hospital in Modena, Italy.
Exclusion criteria were as follows: patients undergoing an open or emergency incisional hernia repair or who had a primary ventral hernia.
Variables and data sources
Patients' data were retrospectively collected from the hospital electronic medical records as well as medical charts by using a specific case report form. Based on the occurrence of hernia recurrence, patients were divided into two groups: recurrence group and nonrecurrence group.
Patients' demographic and baseline characteristics (body–mass index, American Society of Anesthesiologists [ASA] score, comorbidities, and previous surgery); intraoperative data (operative time, degree of adhesions according to Zuhlke classification, 11 conversion to open surgery, type, number and size of mesh, mesh overlap, M/D ratio, and type of tack); hernia site and type; perioperative complications; reoperations; hospital length of stay (LoS); and postoperative hernia recurrence were reviewed and recorded in an electronic database.
Hernia type was defined according to the European Hernia Society (EHS) classification. 12
Outcome measures
Postoperative complications were divided according to the Clavien–Dindo classification. 13 In brief, the complications were classified as follows: any deviation from the normal postoperative course not requiring pharmacological treatment or surgical, endoscopic, or radiological intervention (Grade I); complications requiring drug treatments other than those allowed for Grade I (Grade II); complications requiring surgical, endoscopic, or radiological intervention (Grade III); life-threatening complications requiring intensive care (Grade IV); and death of the patient (Grade V).
The follow-up was conducted through a standardized telephone interview by one investigator (A.D.T.) and consisted of simple questions about the presence of persistent abdominal pain, palpable mass, bulging, constipation, and cosmetic concerns after the surgical hernia repair. All patients revealing any of the abovementioned problems were invited for a visit to the outpatient clinic.
Patients who had been visited by a surgeon for any abdominal complaint after the hernia repair were also invited. Diagnostic imaging studies (parietal ultrasound or abdominal computed tomography scanning) were then requested after the outpatient visit if deemed necessary.
LIHR, intraperitoneal onlay mesh technique
Pneumoperitoneum was established with a Veress needle in the left subcostal space or by open laparoscopy and introducing a 12-mm blunt-tip trocar in the lower flank and selecting the side and site on the abdominal wall allowing the greatest distance from the hernia defect. A 30-degree optic laparoscope was always used for an optimal intraoperative view of the peritoneal cavity.
Two additional blunt-tip trocars, 5 and 12 mm, were placed on the same side of the abdomen cranially and caudally, respectively; for large-sized defects, two to three blunt-tip trocars (5 or 12 mm) were placed on the opposite side to fix the mesh to the anterior abdominal wall.
Adhesiolysis was performed by blunt and sharp dissection, employing bipolar scissors for hemostasis. The entire defect was exposed, as well as the surrounding surface of the anterior abdominal wall, to allow adequate mesh overlap. The hernia sac was not removed. The intraperitoneal onlay mesh (IPOM) technique was performed. The wall defect was not closed. The mesh was rolled and introduced into the abdominal cavity through the 12-mm trocar and then unrolled.
Mesh types are summarized in the following available products: ePTFE (Dual Mesh®), composite (Composix® Bard, Relimesh® Herniamesh, and DynaMesh®-IPOM DynaMesh), coated (Proceed® Ethicon, Parietene® Medtronic, Sepramesh®, and Ventralight® Bard), and partially absorbable (Physiomesh® Ethicon).
The mesh was fixed by two crowns of absorbable (AbsorbaTack® Medtronic, SorbaFix® Bard, Securestrap® Ethicon, and PermaSorb® Bard) or nonabsorbable (CapSure® Bard, ProTack® Medtronic, PermaFix® Bard, EndoAnchor®, Salute II® Bard, and Endopath® EMS Ethicon) tacks or both.
The tacks were fired to obtain a complete 4–5-cm mesh overlap beyond the edges of the fascial defect. The outer crown was placed at least 1 cm away from the mesh border, while the inner crown was positioned 1–2 cm inside from the outer crown. No abdominal drainage was ever placed.
Compliance with ethical standards
The study was carried out in accordance with the International Ethical Guidelines and Declaration of Helsinki. All patients signed a written informed consent before surgery. The study protocol was approved by the local Ethics Committee (Comitato Etico Area Vasta Emilia Centro–CE-AVEC, 913/2021/Oss/AUSLFe).
Statistical analysis
Data are expressed as median (interquartile range 25–75) according to the distribution, which was evaluated by the Shapiro–Wilk test. Categorical data are presented as number (%). Data were analyzed using the chi-square and Mann–Whitney tests to compare percentages and nonparametric data, respectively.
A Cox regression analysis was performed to evaluate predictors of recurrence. The recurrence-free survival was estimated using the Kaplan–Meier product limit method. A log-rank test was run to determine if there were differences in recurrence-free survival according to the type of mesh.
This report complies with the reporting standards established by STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines for reporting observational studies. 14
Results
From September 2002 to September 2017, 312 consecutive patients underwent elective LIHR with a mesh at the Department of Surgery of the S. Anna University Hospital in Ferrara and Department of Surgery of Sassuolo Hospital in Modena, Italy.
At a median 22-month follow-up with a standard telephone interview and appropriate clinical checks, 273 patients (nonrecurrence group) presented no recurrence of incisional hernia, while 39 (recurrence group) had relapsed. In the group of 39 patients with recurrence, 15 patients were reoperated, 4 of which were in the other hospitals.
Among 312 patients, 240 responded to the telephone interview during the follow-up period, 28 did not respond, and 44 died. Among respondents, 48 patients were also invited for a clinical examination in the outpatient clinic.
The demographic and baseline characteristics of patients are illustrated in Table 1. No difference was found in terms of demographic and baseline characteristics (Table 1), type of wall defect, and adhesions (Table 2). No difference was found in the M/D area ratio (Table 3).
Demographic Data and Baseline Characteristics
Types of Wall Defects and Adhesion Scores
Types of Meshes and Tacks
Meshes:
ePTFE meshes (Dual Mesh)
Composite meshes (Bard Composix, Herniamesh Relimesh, and Dyna Mesh)
Coated meshes (Proceed, Parietene Covidien, Bard Sepramesh, and Bard Ventralight)
Partially absorbable (Physiomesh)
Tacks:
Nonabsorbable (Capsure, Protack, Permafix, Endoanchor, Q-ring Salute II Disposable fixation device Bard, Erniagraphes, and EMS Ethicon)
Absorbable (Absorbatack, Sorbafix, Securestrap, and PermaSorb)
1 Missing in the recurrence group and 1 missing in the nonrecurrence group.
IQR, interquartile range.
In the univariate analysis, in the recurrence group, the use of partially absorbable meshes (P < .0001) and use of absorbable tacks (P = .003) were identified as potential predictive factors for recurrence (Table 4).
Intra- and Postoperative Outcomes and Variables
One bowel perforation sutured by the laparoscopic approach.
Two severe bowel perforation cases and three important abdominal adhesion cases (Zuhlke score = 4).
Clavien–Dindo Classification V: one death due to postoperative septic acute cholecystitis in an elderly patient aged 84 years.
One reintervention for uncontrolled bleeding of hepatic round ligament.
IQR, interquartile range; pts, patients.
Intra- and postoperative complications were similar in both groups; two of the three surgical procedures complicated by intestinal perforation were converted into open procedure, while in the other case, a laparoscopic intestinal suture was performed. One severe adverse event (Grade V) occurred, which was related to sepsis due to acute postoperative cholecystitis in an 84-year-old patient.
Reintervention was needed in one case due to bleeding from the round hepatic ligament. No difference between groups was detected in the median hospital LoS (P = .642); patients were discharged a median of 3 days after surgery in both groups. The median interval to recurrence from the surgical procedure was 24 months.
The unadjusted Cox regression analysis showed a statistically significant association between the partially absorbable mesh (P < .0001), absorbable tacks (P = .001), and recurrence, while after adjusting for potential confounders, only the partially absorbable mesh (P = .07) was significantly associated with recurrence (Table 5).
Association Between Characteristics of Patients, Wall Defect, Types of Meshes and Tacks, and Recurrence According to Cox Regression Analysis Adjusted for Potential Confounders
As reported in Figure 1, the partially absorbable mesh, as opposed to the nonabsorbable mesh, was associated with more relapses, which occurred earlier, and therefore the recurrence-free survival period was shorter (log-rank test P < .0001).
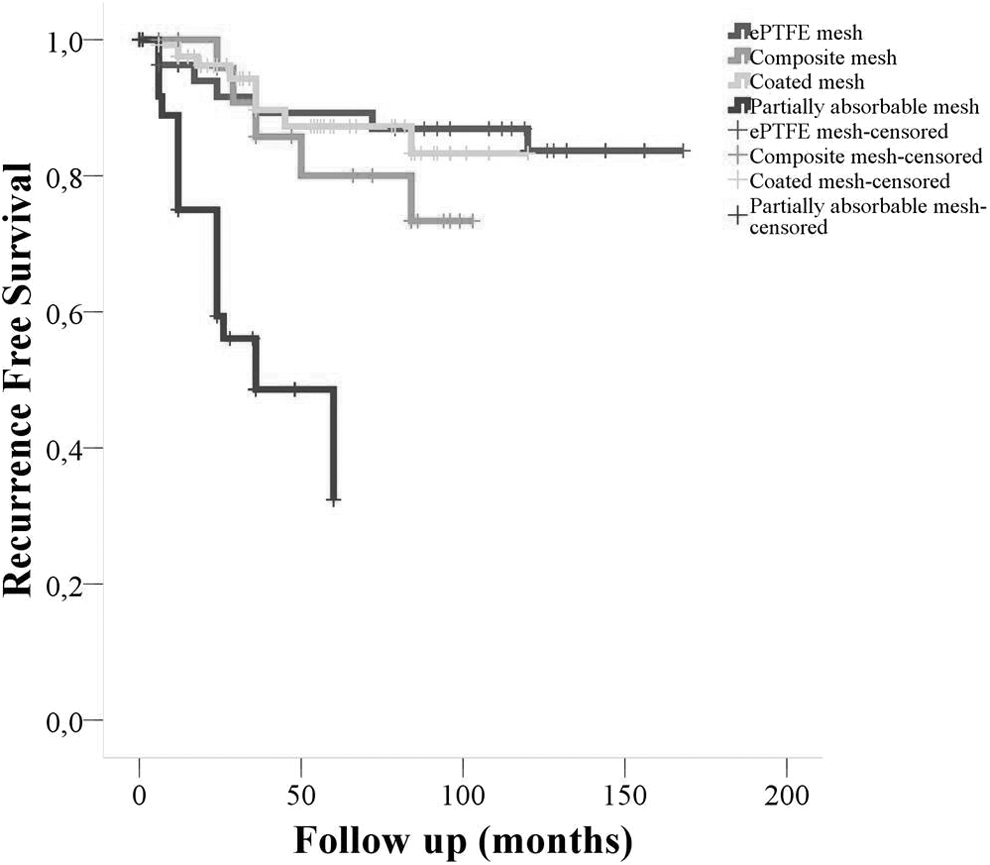
Recurrence-free survival according to the type of mesh (log-rank test P < .0001 for ePTFE meshes, composite meshes, coated meshes, and partially absorbable meshes) (log-rank test P = .605 for ePTFE meshes, composite meshes, and coated meshes).
Comparison of the other three mesh types (ePTFE mesh, composite mesh, and coated mesh) showed no significant difference in recurrence-free survival (P = .605).
Discussion
In this multicenter, retrospective cohort study, the use of a partially absorbable mesh in LIHR was the only predictor of hernia recurrence. On the other hand, the M/D area ratio and use of absorbable tacks were not associated with increase in recurrence. The median time from surgical repair to recurrent hernia detection was 24 months.
Finally, the laparoscopic approach was safe in terms of perioperative morbidity and mortality, with a short hospital LoS.
Does the partially absorbable mesh affect recurrence?
The recurrence rate in our study population was 12.5% (39 of 312 patients); in 46% of patients in the recurrence group (18 of 39 patients), a partially absorbable mesh was used. The multivariate analysis showed that the association between the mesh material and hernia recurrence was influenced by the role of the partially absorbable mesh in the relapse as with the use of other types of meshes, recurrences were evenly distributed.
However, it should be noted that the partially absorbable mesh used in this entire study was the Physiomesh Flexible Composite, which was withdrawn from the market in May 2016 following analysis of data from two, large, independent hernia registries that showed higher than average rates of recurrence after laparoscopic ventral hernia repair compared with other meshes. 6
Köckerling F et al 15 analyzed data from a multicenter internet-based registry and they demonstrated that the use of Physiomesh correlated with a significant increase in recurrence rate after 1-year follow-up compared with the other mesh types recommended in current guidelines (12.5% versus 5%, P < .0001). The authors speculated that the lower burst strength, reduced tissue incorporation due to double antiadhesive coverage, and estimated 30% mesh shrinkage at 90 days were all possible explanations for such a high recurrence rate. 15
Does the M/D area ratio predict recurrence?
In our study, although not statistically significant in the multivariate analysis, 66% of patients (26 of 39 patients) who showed a recurrent hernia had a W2 incisional hernia preoperatively, while mesh overlap was homogeneous in both groups and ≥5 cm, according to current clinical guidelines. 5 To correctly assess other factors related to the size of the defect, we also analyzed the M/D ratio, 10 but no difference between groups was detected.
In a retrospective study on 213 patients, Hauters et al 10 found a correlation between the M/D ratio and risk of recurrence; however, in our study, the M/D ratio was not associated with recurrence in both univariate and multivariate analyses.
Further studies are therefore necessary to validate the M/D ratio as a tool to choose the size and surgical technique in incisional hernia repair and to determine its association with recurrence.
Does the tack type influence the risk of recurrence?
In accordance with the literature, we found no correlation between the mesh fixation method and the recurrence rate in the multivariate analysis (1.09 [0.37–3.22]; P = .07).4–6
In a national cohort study on 816 patients from the Danish Ventral Hernia Database, recurrence-free survival was lower among patients in whom absorbable tacks were used compared with nonabsorbable ones (71.5% versus 82%; P = .007). 16 The follow-up, however, was shorter with absorbable tacks (34 months versus 44 months) and hernia defects were larger with nonabsorbable tacks (median diameter 9 cm versus 7 cm). In addition, there was no difference in the chronic pain rate. 16
A recent systematic review, including five studies (three RCTs and two observational studies), 8 showed no difference between the two mesh fixation techniques in terms of recurrence (risk difference [RD] 0.03, 95% confidence interval [CI] −0.04 to 0.09, P = .47), chronic pain (Odds ratio [OR] 0.91, 95% CI 0.62–1.33, P = .64), seroma (OR 0.98, 95% CI 0.37–2.60, P = .96), hematoma (RD −0.00, 95% CI 0.04–0.04, P = .99), prolonged ileus (OR 0.99, 95% CI 0.24–4.03, P = .99), hospital LoS (mean difference [MD] 0.10, 95% CI −0.36 to 0.56, P = .68), and port-site hernia (OR 0.98, 95% CI 0.13–7.16, P = .98), while the operative time was longer with absorbable tacks (MD 7.53, 95% CI 1.49–13.58, P = .01).
Of note, the results remained consistent when analyzing the three RCTs separately.
Strengths and limitations of the study
This is a large retrospective study that investigated the recurrence rate in LIHR. The study population was more homogeneous with respect to the abdominal defect (e.g., size, site) and peritoneal adhesions, as only patients who underwent elective laparoscopic incisional rather than ventral hernia repair were included.
However, some limitations exist and therefore the results should be interpreted with caution. This is a retrospective study including a large cohort of patients over 15 years (chronological bias). Among patients with a W1 defect, the vast majority was operated in the first period of the study and characterized by a small defect (≤3 cm).
The results of the study may also be affected by the use (in our series) of a mesh (i.e., Physiomesh) that has been withdrawn by the manufacturer due to the high recurrence rate detected at 1-year follow-up. As this mesh represented all the partially absorbable mesh types employed in this study, the higher risk of recurrence conferred by its use cannot be attributed to other partially absorbable meshes.
Unfortunately, due to the retrospective design of our study, we could not evaluate other variables such as postoperative pain and discomfort and we may have experienced an increased rate of loss to follow-up.
Conclusions
LIHR is a safe and effective surgical technique that (in terms of hernia recurrence) is not influenced by the type of material, provided that well-tested partially absorbable mesh materials are used. Further studies are needed to clarify the role of the type of mesh used and the M/D area ratio in prevention of hernia recurrence.
Ethical Approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments.
Informed Consent
Written informed consent was obtained from all patients reported in this study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.