
Abstract
Background:
The monkeypox virus (MPXV) has spread globally, causing an infection similar to that of smallpox. In July 2022, MPXV was declared an international public health emergency by the World Health Organization. Although the prodromal and cutaneous symptoms are described, the literature is lacking with regard to the upper airway manifestations of the disease.
Methods:
This case report describes a 39-year-old gentleman with a history of human immunodeficiency virus who presented to the emergency department with fever, sore throat, and cough. A literature review was also performed to determine the clinical presentation and physical examination findings of patients presenting with MPXV.
Results:
The patient underwent flexible laryngoscopy on two separate occasions due to his symptoms of fever and sore throat. He was noted to have white plaque-like lesions throughout the upper aerodigestive tract that could not be excised with manipulation. Ultimately, he tested positive for MPXV and was treated with full recovery.
Conclusions:
To our knowledge, this is the first report describing upper airway manifestations of MPXV. Since patients with MPXV often present initially with pharyngitis, understanding the physical examination findings of MPXV in the upper airway is imperative for early diagnosis and public health awareness.
Introduction
As the global community begins to emerge from the devastating impact of the COVID-19 pandemic, a new public health crisis, the monkeypox virus (MPXV), has emerged. From May through September 2022, monkeypox cases climbed to >58,000 across 103 countries, with ∼22,000 cases in the United States alone. 1 In July 2022, the World Health Organization officially declared the current monkeypox outbreak a public health emergency. 2
Monkeypox is an orthopoxvirus, closely related to variola (smallpox), both of which are within the poxviridae family. 3 Vaccination to smallpox is up to 85% protective against monkeypox. 4 However, the recent global monkeypox outbreak is thought to be largely due to the waning global immunity to smallpox with cessation of routine vaccination since its eradication in 1980. 4 Within endemic regions, the MPXV is spread primarily to humans through ingestion or contact with infected wildlife, particularly rodents.3,5
In the current outbreak, the majority of transmissions occur between humans through respiratory droplets, direct contact with skin lesions, exchange of bodily fluids, and fomites on contaminated surfaces.5,6 Men who have sex with men appear to be at highest risk for contracting monkeypox.5,7–9 Research is ongoing as to the influence of human immunodeficiency virus (HIV) on disease severity. 8
Patients with monkeypox infection often present with fever, sore throat, malaise, muscle aches, and headache followed by mucocutaneous eruptions 2–4 days later.3,8,9 With regard to otolaryngological symptoms and signs, patients with MPXV may develop perioral ulcers, pharyngitis, odynophagia, and epiglottitis.5,7–9 Severe otolaryngological complications of monkeypox, such as pharyngeal edema, can compromise the airway and may require endotracheal intubation.8,9
Despite the frequent pharyngeal symptoms that MPXV patients endorse, the clinical manifestations of MPXV in the upper airway have yet to be described in the literature. This report documents the laryngoscopic findings in a patient who presented to the emergency department (ED) with MPXV. In addition, a literature review was performed regarding the classic monkeypox presentation, disease course, otolaryngological manifestations, preventive measures, and treatment.
Case
Ethical Statement
All case reports are considered exempt from review by Medstar Health IRB and the patient presented herein gave written consent for this study.
A 39-year-old African American gentleman presented to the ED complaining of a dry cough, fever, fatigue, body aches, hoarseness, left ear fullness, shortness of breath on exertion, and worsening sore throat for 3 days. He also noted a new nonpainful ulcer on his penile shaft and left hand, which appeared 24 hours prior. The patient's medical history was significant for antiretroviral-controlled HIV for 4 years with undetectable viral load and a 2.5 pack-year smoking history. His social history was notable for multiple recent male sexual partners. He denied any illicit drug use, recent sexually transmitted diseases, or recent sick contacts.
On presentation, his vital signs were notable for a temperature of 103.7°F and tachycardia. Physical examination was significant for uvular deviation, bilateral tonsillar erythema, and oropharyngeal edema. Noncontrast neck computed tomography showed asymmetric left tonsillar, supraglottic, and lateral pharyngeal fullness with rightward deviation of the aerodigestive tract and partial effacement of the left pyriform recess. Laboratories were significant only for a white blood cell count elevated to 11,400 × 109/L. He tested negative for COVID-19 and was treated supportively with acetaminophen, dexamethasone, and intravenous ampicillin/sulbactam in the ED.
Otolaryngology was consulted for upper airway evaluation due to the radiographic evidence of airway narrowing. At the time, his physical examination was significant for bilateral acute tonsillitis (left greater than right), with no evidence of drainable peritonsillar collections. Flexible fiberoptic laryngoscopy revealed mild diffuse left pharyngeal fullness, extending to the left pyriform sinus with no notable lesions (Fig. 1). There was no evidence of significant airway compromise or notable oropharyngeal lesions.

Flexible laryngoscopy (during the patient's initial visit) showing a patent airway with mild diffuse left pharyngeal fullness, extending to the left piriform sinus.
During that ED visit, he was also examined by the infectious disease service and noted to have new pruritic penile lesions and a pustule on his left hand. The lesions raised suspicion for a diagnosis of MPXV versus syphilis, prompting empiric treatment with intramuscular benzathine penicillin. Both lesions were swabbed for nonvariola orthopoxvirus real-time PCR testing and the patient was advised to self-isolate. He was discharged home on a 14-day course of amoxicillin/clavulanate potassium.
However, he returned to the ED 3 days later with worsening odynophagia, muffled voice, headache, and a temperature of 101.6°F. Otolaryngology was reconsulted for upper airway evaluation. Repeat laryngoscopy revealed white plaque-like lesions throughout the mucosa of the upper aerodigestive tract (Fig. 2a, b) and left pyriform sinus (Fig. 3) that could not be excised with manipulation. His airway was patent and the lesions were nonobstructive and nonfriable (see Supplementary Video S1).
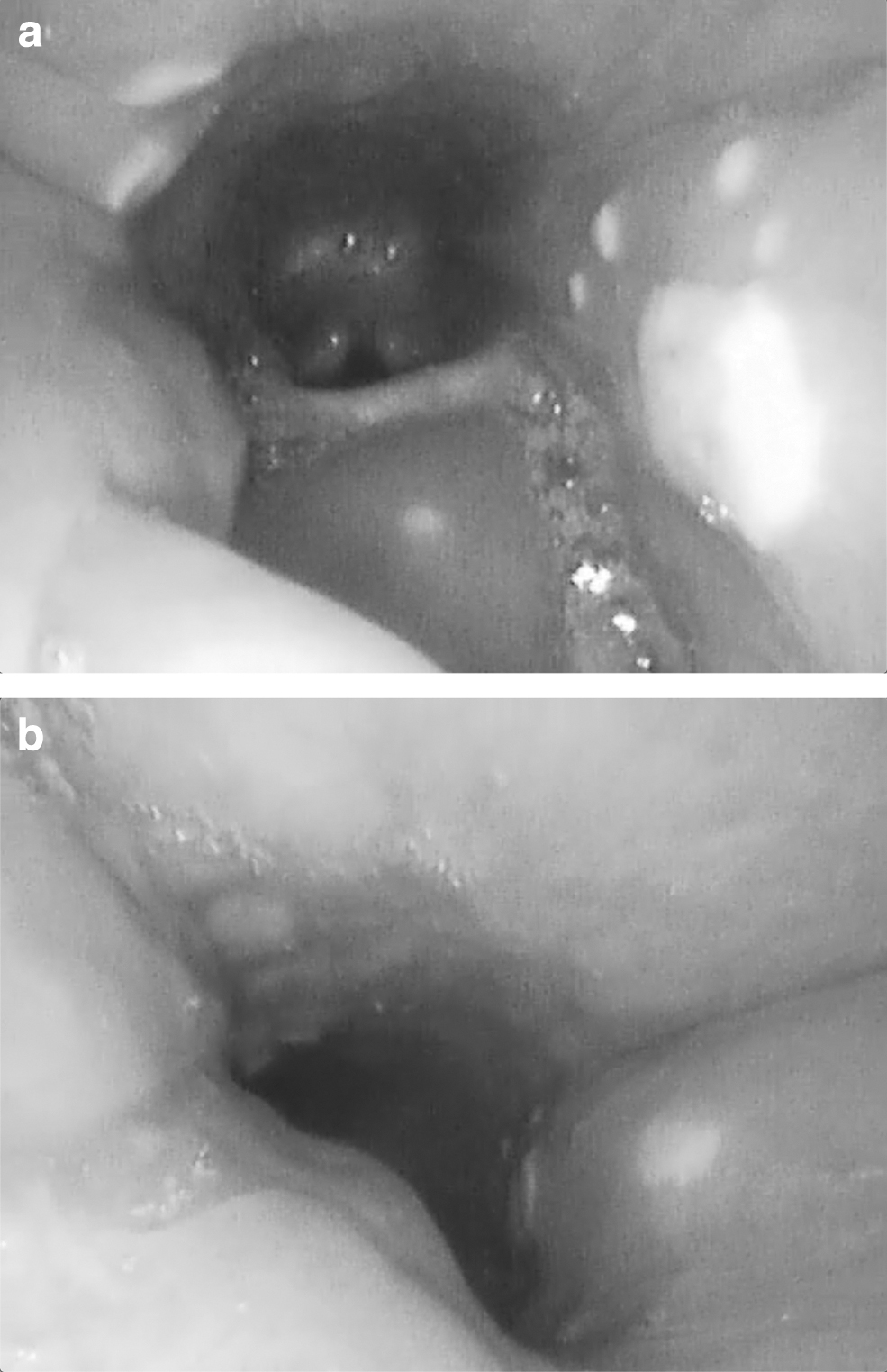
Flexible laryngoscopy (during the patient's return visit 3 days after initial presentation) showing white nonfriable plaque-like lesions in the left piriform sinus.
He was transitioned to clindamycin and discharged home from the ED. Several days later, his monkeypox test returned positive and he was notified through telephone and advised to self-isolate until all symptoms (including his rash) resolved. On follow-up, his symptoms were significantly improved and he was encouraged to obtain MPXV vaccination.
Discussion
To our knowledge, this is the first report of upper airway manifestations of MPXV. The majority of patients with MPXV present initially with fever, skin lesions, proctitis, and pharyngitis.8,9 Therefore, understanding the appearance of monkeypox lesions in the upper airway mucosa is critical for both early diagnosis and treatment as well as public health awareness.
Our patient presented with a known history of antiretroviral-controlled HIV and multiple recent male sexual partners. This population is known to be a high-risk group in the current monkeypox outbreak.5,7–9 In a prospective cross-sectional study of 185 patients with monkeypox, Catala et al found that 42% of those infected were HIV positive with an undetectable viral load in the vast majority (90%). 8 They found no significant difference in disease severity among patients with HIV compared with those without HIV. 8 Understanding the populations most vulnerable to MPXV is vital to inform clinicians, public health officials, and policy makers as they target limited preventive resources and vaccination efforts.
Initially, respiratory droplet exchange, direct lesion contact, and fomite-associated surface spread were suggested as the primary means of MPXV transmission.5,6 However, recent studies increasingly advocate that sexual interactions—through direct lesion contact and fluid exchange—play a significant role.7,8 This assertion is supported by the fact that most lesions involve the genital, anal, and oral mucosa region. 7 These lesions were observed in our patient. Among 528 MPXV infections across 43 sites, Thornhill et al estimated as many as 95% of patients were infected through close sexual contact. 7 Moreover, one study found that 76% of patients with MPXV also had a concomitant sexually transmitted infection (STI) on screening, raising the possibility of STIs serving as a facilitator for monkeypox infection. 8
Our patient experienced prodromal symptoms 2 days before the appearance of his throat, hand, and genital lesions. This timeline echoes the majority of cases presented in the literature.5,7–9 In one study of 197 patients, 61.5% had prodromal systemic symptoms before lesion onset, 38.5% afterward, and 13.7% experienced solely mucocutaneous manifestations. 5 Fever is the most common symptom, along with lymphadenopathy, lethargy, myalgia, and headache. 7 As for rash symptoms, Patel et al found that 88.3% of patients developed mucocutaneous lesions on the genital, anal, or perianal region. 5 The rash appears to evolve in the following sequence: maculopapular, vesicular, pustular, and finally crusted blisters. 8
Otolaryngological symptoms are also common in the disease presentation, as was evident in our patient. In one case series, 18% of patients presented with sore throat. 8 Pharyngitis, epiglottitis, and odynophagia are other common otolaryngological features of MPXV infection. 9 Thornhill et al found that ∼10% of patients presented with only mucosal oropharyngeal lesions. 7 However, to our knowledge, there is no current literature that demonstrates the appearance of oropharyngeal and laryngeal lesions in patients with MPXV. In our patient, the initial laryngoscopy demonstrated nonspecific erythema and fullness of the pharyngeal wall.
Repeat laryngoscopy 2 days later revealed white lesions over the left tonsil, uvula, right lateral pharyngeal wall, and left pyriform sinus that could not be excised with manipulation. In the context of other characteristic disease findings, practicing otolaryngologists who note similar findings in their patients should consider MPXV.
Overall, the rate of hospitalization from monkeypox infection is low, ranging from 2% to 13% in published studies.5,7,8 However, otolaryngological complications, such as severe odynophagia, dysphagia, poor oral intake, airway edema, and tonsillar abscesses, are a significant cause of admission among these patients.5,7,8 Monkeypox is typically self-limited, lasting 2–4 weeks, and requires only symptomatic control. 5 Per the Centers for Disease Control (CDC), there is currently no treatment approved specifically for monkeypox. 10 However, tecovirimat—an antiviral utilized for smallpox treatment—is approved by the United States Food and Drug Administration for severe cases or immunocompromised patients at high risk for severe disease.3,10
Various preventive measures should be undertaken to curb the spread of MPXV. Currently, two vaccines are recommended by the CDC. JYNNEOS is specifically approved for monkeypox, whereas the smallpox immunization, ACAM2000, is available under an Expanded Access Investigational New Drug protocol.10,11 As for personal protective equipment, the CDC recommends utilizing a gown, gloves, eye protection, and an N95 mask when treating patients with MPXV. 12
Conclusion
We present unique laryngoscopic findings of MPXV infection in an HIV-positive male patient who presented with fever and sore throat. Although MPXV is self-limited with a low mortality rate, a knowledge of the appearance of these flat white lesions in the upper airway is critical for the otolaryngologist and medical community at large. This case report and literature review informs otolaryngologists and practicing clinicians of the upper airway manifestations of MPXV to facilitate early diagnosis and public health awareness.
Footnotes
Authors' Contributions
A.M.H. contributed to investigation, writing—original draft, and writing—review and editing. J.D.J. was involved in conceptualization, data curation, writing—review and editing. A.H. was in charge of conceptualization, resources, and writing—review and editing. J.H.M. carried out conceptualization, methodology, writing—review and editing, and supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.