
Abstract
Background:
Laparoscopic common bile duct exploration (LCBDE) and endoscopic retrograde cholangiopancreatography (ERCP) are two methods of retrieving common bile duct (CBD) stones. Aspects of CBD stone management, such as sphincterotomy, have been implicated as risks for CBD stone recurrence although evidence is weak. The aim of this study was to compare stone recurrence following LCBDE and/or ERCP.
Methods:
Data were collected retrospectively for patients undergoing LCBDE and/or ERCP for CBD stones at a single center from 2008 to 2018. Primary outcome was stone recurrence (>6 months after duct clearance). Risk factors for recurrence were assessed using univariate and multivariate analyses.
Results:
A total of 445 patients underwent LCBDE-only, 79 patients underwent ERCP-only and 80 patients underwent LCBDE-ERCP. LCBDE-only patients were younger and preoperatively less morbid than ERCP-only patients. Although there was no significant difference for recurrence, there was a trend toward higher recurrence with ERCP-only compared with LCBDE-only and LCBDE-ERCP (5.1% versus 2.0% and 2.5%, P = .280). On univariate comparison, patients with a recurrence were significantly older, had a higher admission white cell count, higher number of ERCPs, increased transampullary stent use, and higher maximum CBD diameter. Total number of ERCP was the only independent predictor of stone recurrence (odds ratio 6.85 [2.55–18.42], P < .001) following multivariate regression.
Conclusion:
Management plan was not associated with stone recurrence. The total number of ERCP was the only independent predictor of recurrence. Within the limitations of case selection and bias toward LCBDE, this study suggests that limiting repeated ERCP may reduce CBD stone recurrence.
Introduction
The ideal treatment algorithm for patients with concurrent cholelithiasis and choledocholithiasis remains debatable.1–3 At present, treatment options include single-stage laparoscopic cholecystectomy (LC) and laparoscopic common bile duct exploration (LCBDE) or endoscopic retrograde cholangiopancreatography (ERCP) before, during, or after LC. Stone recurrence following each of these approaches is not uncommon.4–8 Endoscopic procedures usually require sphincterotomy for stone extraction with stone recurrence being a late complication. 9 Similarly, various adjuncts at endoscopic and/or surgical management including t-tube, transampullary stent, and lithotripsy have also been reported as risk factors for recurrence.10–12 In addition to anatomical factors like stone size and common bile duct (CBD) characteristics, various patient-related factors have also been identified as potential risk factors for recurrence.4,8,13–15
Many studies of recurrence for surgical and endoscopic treatment of CBD stones do not take into account the LC, which in itself can be a risk factor for recurrence. 10 Moreover, there is often selection bias owing to local expertise and availability of resources. 1 The aim of this study was to identify risk factors for stone recurrence when surgical and/or endoscopic approaches were used for stone extraction.
Methods
This study was performed retrospectively at a single center, Northern Health, Victoria, Australia. Patients who underwent LCBDE or ERCP between January 1, 2008 and December 31, 2018 were identified from a prospectively maintained electronic patient registry. ERCP and LCBDE were limited to within 90 days before or after LC (Fig. 1). Although most surgeons were supportive of LCBDE at Northern Health, there were no policies that mandated a treatment algorithm for a patient with concurrent CBD stones. Instead, the operating surgeon decided the management plan and had available a 24-hour on-call LCBDE service, comprising five general and hepatobiliary surgeons trained to perform LCBDE, who could assist or perform the LCBDE. Patients were retrospectively allocated to four groups based on the initial operative plan as identified from the patient consent form: LCBDE, preoperative ERCP, intraoperative ERCP, or postoperative ERCP.
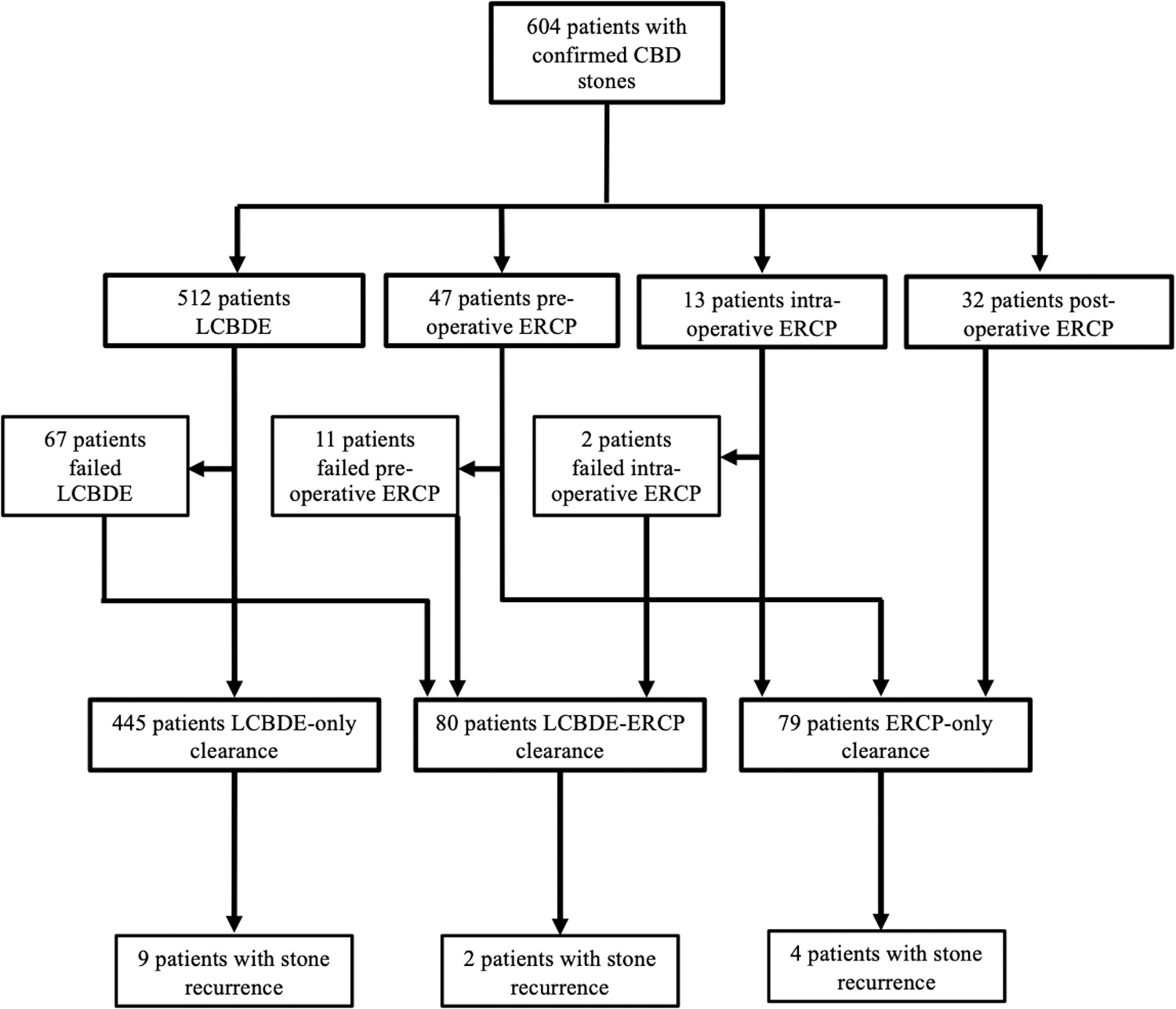
Flow diagram for patient selection.
The operation report was reviewed to determine the eventual management and patients retrospectively allocated into one of LCBDE-only, ERCP-only or LCBDE-ERCP. Stone recurrence was defined as a CBD stone that was identified more than 6 months after index CBD clearance.10,16 All recurrences during the study period (until January 1, 2021) were recorded. CBD stones identified within 6 months of clearance were defined as retained stones. A period of 90 days from index LCBDE or ERCP was set when assessing procedure-related complications, mortality, and additional procedures to clear CBD stones. In addition, if a patient underwent an open cholecystectomy, had postoperative ERCP performed for an indication other than choledocholithiasis, or if LC was performed at another institution, they were excluded from the study (Fig. 1).
Each patient had age, urgency of procedure, reason for procedure, preoperative blood tests, preoperative imaging findings, and initial procedure American Society of Anesthesiologists (ASA) score recorded. The presence of peri-ampullary diverticulum (PAD), CBD diameter, CBD stone size, and number were also reported. In addition to stone recurrence, outcomes assessed included number of admissions and procedures, length of stay (LOS), success at CBD clearance, Clavien–Dindo classification-based complications, 17 and mortality.
Laparoscopic common bile duct exploration
LC was performed using standard four-port technique with the surgeon standing on the patient's left side and routine intraoperative cholangiography was undertaken. Choledochoscopy was performed using a 3 or 5 mm choledochoscope (Olympus, Tokyo, Japan). Access was via an existing port or additional right subcostal margin port. The cystic duct opening was cannulated and transcystic exploration was routinely performed. The decision to perform transductal exploration was at the discretion of the operating surgeon, with choledochoscopy performed after a longitudinal incision along the CBD. Stone extraction was performed using 1.5F, 2.2F NCircle® tipless, or 1.7F NCompass® tipless nitinol stone extractor baskets (Cook Medical, Bloomington, IN). At the discretion of the operating surgeon, repeat choledochoscopy or cholangiography to ensure duct clearance, primary versus t-tube closure of choledochotomy, biliary stent insertion, or subhepatic drain insertion was performed. Following these steps, the cystic duct was clipped and routine cholecystectomy was completed.
Endoscopic retrograde cholangiopancreatography
A 24-hour on-call ERCP service consisting of three consultant surgeons and two consultant gastroenterologists was available at Northern Health. Standard ERCP was performed using a 13.5 mm duodenoscope (TJF-240; Olympus). Although sphincterotomy was routinely performed, endoscopic papillary balloon dilation was not used for stone removal. Using an appropriately sized sphincterotome, wire-guided cannulation of the major papilla was performed. If subsequent cholangiography confirmed a CBD stone, a sphincterotomy was performed. In a few instances a single-use LithoCrushV® mechanical lithotripter (Olympus) was used to break up stones.
The CBD was trawled using an Extractor® Pro RX balloon (Boston Scientific, Boston, MA) to remove stones. Subsequent cholangiography was performed to check for CBD clearance, at which point the procedure was deemed successful. An appropriately sized transampullary stent (Zimmon® stent, Cook Medical or Advanix® stent; Boston Scientific) was placed when stone removal was unsuccessful or sphincterotomy was not possible. When transampullary stenting was used, repeat ERCP was performed 4–6 weeks later for stent removal.
Statistical analysis
Descriptive analysis was undertaken to provide a comparative profile of patients based on their eventual management. Normally distributed variables were presented as mean and standard deviation, and non-normally distributed variables were presented as median and interquartile range. Chi-squared test or Fisher's exact test was performed for categorical variables. For continuous variables, Student's t-test was used for normally distributed data and Kruskal–Wallis test used for non-normally distributed data, with one-way analysis of variance (ANOVA) test used for multiple groups.
Multinomial logistic regression analysis was conducted to test for the association between stone recurrence and various patient factors. Variables included in the multivariable analysis were selected if the P values were <.1 on univariate analyses. Manual backwards step-wise regression techniques were used to obtain the final multivariable models.
All P values were two-sided and P < .05 indicated a statistically significant difference. Statistical analysis was performed using SPSS (IBM, Armonk, NY). This study was approved by the local research and ethics committee (ALR 35.2017).
Results
A total of 604 patients had confirmed CBD stones, with 445 patients undergoing LCBDE-only, 79 patients ERCP-only, and 80 patients LCBDE and ERCP (Fig. 1).
Patients who underwent LCBDE-only were significantly younger and more likely to be women, whereas patients undergoing ERCP in their management were more likely to be suspected to have choledocholithiasis (Table 1). In addition, LCBDE-only patients were preoperatively less morbid. In contrast, ERCP-only patients were more likely to be older, have higher ASA scores, and have preoperative blood results that were similar to or significantly worse than LCBDE-ERCP patients, suggesting this could be a higher operative risk group.
Patient Characteristics
ASA, American Society of Anesthesiologists; CBD, common bile duct; ERCP, endoscopic retrograde cholangiopancreatography; IQR, interquartile range; LCBDE, laparoscopic common bile duct exploration; LFT, liver function test; SD, standard deviation; WCC, white cell count.
When comparing outcomes, LCBDE-only patients had significantly lower number of admissions, procedures, LOS, and the shortest operating times (Table 2). Similarly, LCBDE-only patients had significantly lower missed stones, minor and major complications, and mortality compared with ERCP-only and LCBDE-ERCP groups. In contrast, the ERCP-only group had the highest CBD clearance rate and unsurprisingly the highest sphincterotomy rate. Transampullary stent use was also significantly higher in the ERCP-only and LCBDE-ERCP groups. Although there was no significant difference for stone recurrence, there was a trend toward higher recurrence with ERCP-only group. The median time to recurrence was much longer for the combined LCBDE-ERCP group compared with the LCBDE-only and ERCP-only groups, although it was not statistically significant (1140 versus 358 and 446 days, P = .203) (Fig. 2).
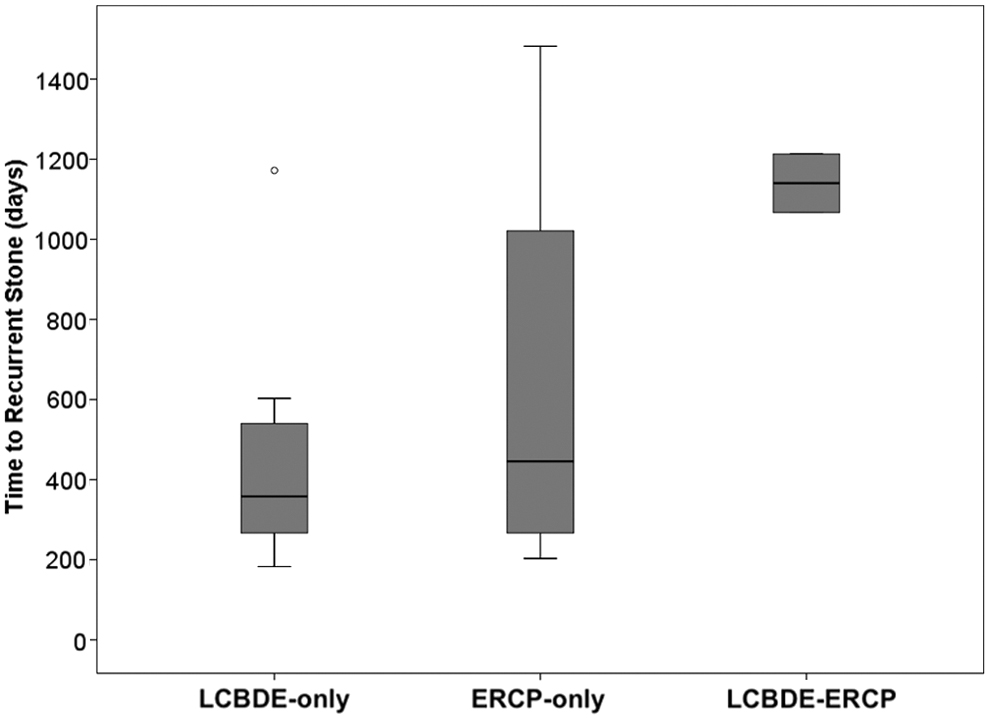
Box and whisker plot showing time to stone recurrence.
Outcomes
ASA, American Society of Anesthesiologists; CBD, common bile duct; ERCP, endoscopic retrograde cholangiopancreatography; IQR, interquartile range; LCBDE, laparoscopic common bile duct exploration; LOS, length of stay.
On univariate comparison, patients with a recurrence were significantly older, had a higher number of ERCPs, higher admission white cell count (WCC), higher transampullary stent use, and maximum CBD diameter (Table 3). Of interest, number of stones, success at CBD clearance, presence of PAD, and lithotripter use were not significantly different among recurrence and nonrecurrence patients. Furthermore, both the initial and eventual operative plan and presence of a minor or major complication were not significantly different between recurrence and nonrecurrence groups. Although sphincterotomy was more likely in a patient who had a recurrence, this was not significant when compared with nonrecurrence patients.
Factors Associated with Common Bile Duct Stone Recurrence
ASA, American Society of Anesthesiologists; CBD, common bile duct; ERCP, endoscopic retrograde cholangiopancreatography; IQR, interquartile range; LCBDE, laparoscopic common bile duct exploration; LOS, length of stay; PAD, peri-ampullary diverticulum; SD, standard deviation; WCC, white cell count.
With logistic regression analysis on all factors significant to P < .1, only number of ERCP and transampullary stent use were significant on univariate analysis (Table 4). On multivariate analysis, only total number of ERCP remained significant as an independent predictor of stone recurrence (odds ratio 6.85 [2.55–18.42], P < .001).
Logistic Regression Analysis for Independent Predictors of Recurrence
Analysis carried out on all variables with a P < .1, except ASA as logistic regression was not possible with values of 0 in some subgroups.
CBD, common bile duct; ERCP, endoscopic retrograde cholangiopancreatography; OR, odds ratio; WCC, white cell count.
Discussion
This study compared recurrence rates between LCBDE directly with ERCP, taking into account the accompanying LC, from the viewpoint of a health service that promotes LCBDE. Although several factors were associated with CBD stone recurrence, interestingly the management plan (LCBDE based or ERCP based) was not one of them. The only factor strongly associated with a recurrence on logistical regression analysis was the number of ERCP and thus was the only independent predictor of recurrent CBD stones.
Stone recurrence rates in LCBDE and ERCP groups were both low, and although it was statistically not significant, there was a trend toward higher recurrence in the ERCP-only group. Recurrence rates for ERCP were comparable (5.0% versus 4%–24%), 7 but lower for LCBDE compared with the literature (2.0% versus 5.4%–17.6%).4–6,8 It is not surprising that the sphincterotomy rate was highest in the ERCP-only group. Performing a sphincterotomy leaves a wide opening at the ampulla and theoretically allows an easy passage for bile to flow, however may also allow reflux of duodenal contents into the CBD. Although some studies have shown endoscopic sphincterotomy is not a risk factor for recurrent choledocholithiasis,4,13,18–20 others have shown it as an independent risk factor for recurrent choledocholithiasis.5,10
Observational studies with long-term follow-up have shown stone recurrence mostly occurring within 3 years following sphincterotomy, 9 with a cumulative incidence of 11.8, 16.1, and 22.9 at 5, 10, and 15 years, respectively. 21 It is thought that sphincterotomy permanently damages the one-way valve mechanism of the sphincter of Oddi, leading to biliary reflux and bacterial colonization of the tract. 22 Alteration to the biliary microbiome,23–25 changes to stone composition,22,26 as well as duodenal reflux 27 may be contributing factors to recurrent CBD stones. In addition, endocrine cell hyperplasia in the lower biliary tract owing to longstanding inflammation has also been linked to choledocholithiasis via disturbed bile flow, increased mucous secretion, and fibrosis. 28 Repeat ERCP is thought to further mechanically damage the sphincter mechanism and propagate this chain of events. 7
Comparing surgical with endoscopic and combination treatment, there was no significant difference in recurrence rates in this study. Meta-analyses have shown either no significant difference between LCBDE and preoperative ERCP 3 or significantly lower recurrence rates for LCBDE over preoperative ERCP. 2 In this study, given the trend toward higher recurrence rate in ERCP-only patients, the numbers in the ERCP-only cohort may have been too low to show a difference between LCBDE-only and ERCP-only groups (Type II error). Power calculations, just looking at these two groups and using the outcomes and ratios from this study, reveal that a study population of >1850 patients would be required to confirm over a 2.5 × higher rate of recurrence in the ERCP-only group. Rather than the method of stone removal, the repeated disruption to the sphincter complex may be more important in predicting stone recurrence.
Leaving a transampullary stent may also be a contributing factor. Although the evidence surrounding transampullary stenting is conflicting, with some studies identifying it as an independent predictor of recurrence,11,19 others have shown that it is an independent predictor of reduced long-term recurrence 7 or is not associated with recurrence. 8 Another study has shown that longer stent indwelling time is significantly associated with biliary sludge formation, a precursor to stone formation. 29 This study found a strong univariate correlation between stent placement and stone recurrence; however, this was related to repeated ERCP and thus became nonsignificant in multivariate analysis. In addition to the method of treatment chosen, there were also numerous patient- and pathology-related factors that may have contributed to eventually requiring multiple ERCPs.
In this study, recurrence was associated with patients who were significantly older, had a higher WCC on admission, or maximum WCC. These factors may have been indirect markers of preoperative morbidity. Only one study has shown that elevated preoperative WCC is an independent predictor of CBD stone recurrence. 6 The preoperative WCC may be a marker for biliary inflammation and oxidative stress, key components of primary choledocholithiasis.6,30 A meta-analysis of elderly patients (>65 years old) undergoing LCBDE showed no significant difference in recurrence with age. 31
Similarly, two single-center retrospective studies comparing LCBDE with preoperative ERCP in elderly patients (>80 years old) showed no significant difference in recurrence.32,33 However, following multivariate regression analysis, there are conflicting reports for age as an independent risk factor for recurrence with LCBDE4–6,10,15 and ERCP.7,11,13,19,20 The differing results may in part relate to heterogeneity in age criteria between studies and the bias toward performing LCBDE in younger patients, similar to this study. Furthermore, CBD stone recurrence is only one complication from CBD stone extraction, and these factors may also have been important in determining the method of treatment that was safest in short term.
Conclusion
In conclusion, this study showed that there was no difference in CBD stone recurrence rate between different management plans. Although numerous patient-, anatomical-, and procedure-related factors were associated with recurrence of CBD stones, only total number of ERCP was an independent predictor of recurrence. Within the limitations of case selection and bias toward LCBDE, this study suggests any management paradigm that limits repeated ERCP (such as LCBDE) may reduce CBD stone recurrence.
Footnotes
Authors' Contributions
H.M.D.S.: Investigation (lead), data curation (lead), writing—original draft, writing—review and editing; T.H.: Investigation, data curation, writing—review and editing; T.Y.: Supervision, writing—review and editing; R.H.: Conceptualization, supervision (lead), formal analysis, writing—review and editing (lead).
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.