
Abstract
Background:
Our objective in this study is to compare the early outcomes of patients who underwent technical resection of non-small cell lung cancer (NSCLC) with video-assisted thoracoscopic surgery (VATS) with multi-joint wristed instruments, also known as surgeon-powered robotic surgery (SpRS) and conventional VATS.
Methods:
One hundred twenty-two thoracoscopic lung resections were performed in our hospital for NSCLC between March 2021 and March 2022. Of these resections, 95 were performed with VATS, while 27 patients underwent the SpRS technique.
Results:
Lobectomy was performed in 112 patients (91.8%), and segmentectomy was performed in 10 patients (8.2%). The median duration of hospitalization was 5 days in patients who underwent VATS, while the median duration of hospitalization was 4 days in patients who underwent the SpRS technique. No significant difference was found between the groups when demographic characteristics were compared with surgical techniques. The median drainage was 125 mL in the SpRS technique, while 150 mL of drainage occurred in patients who underwent resection by VATS (0.165). While an average of 12 lymph nodes was dissected in the VATS group, an average of 14 lymph nodes was dissected in the SpRS group (0.602). Complications occurred in 17 patients (13.9%). Complications were observed at a rate of 16.8% in the VATS group, while complications were observed at a rate of 3.7% in the SpRS group (P = .116).
Conclusion:
As a result, our study shows that it is an effective and reliable method with early results similar to thoracoscopic surgery. Registration Number: 2022-194.
Introduction
Video thoracoscopic surgery is developing rapidly. Besides, it is effectively performed as the gold standard treatment method in early-stage lung cancers.1,2 Yet, one of the most notable challenges in video-assisted thoracoscopic surgery (VATS) is movement limitation in the surgery due to the rigidity of the thoracoscopic instruments utilized. Due to these movement limitations, additional thoracoport incisions are needed during the procedure, and multiportal approaches are required.
Thus, nowadays, robotic surgery techniques are becoming more popular as they allow more flexibility in movement in a small area. However, one of the most important problems in robotic surgery is that the surgeon is away from the operating table, there is no sense of tactile feedback, and it is only available in limited centers due to its cost. 3 This, in turn, makes it difficult to learn these new surgical instruments and requires an assistant surgeon at the table during the operation.
For all these reasons, the use of angled endoscopic instruments has begun to increase. The first publication on the use of these instruments in thoracic surgery was made by Trevis et al. 4 These instruments are a combination of VATS and robotic surgery. Trevis et al. 4 also used the definition of surgeon-powered robotic surgery (SpRS) for these instruments. However, there are few publications in the literature regarding the early outcomes of these instruments.4,5
Our aim in this study is to compare the early oncological outcomes of patients who underwent technical resection with multi-joint wristed instruments and conventional VATS for non-small cell lung cancer (NSCLC).
Materials and Methods
One hundred twenty-two thoracoscopic lung resections were performed in our hospital for NSCLC between March 2021 and March 2022. Of these resections, 95 were performed with VATS, while 27 patients underwent the SpRS technique.
To ensure homogeneity in the study, patients in the VATS group who underwent neoadjuvant lung resection, sleeve resections, and pneumonectomy by the SpRS technique were excluded. Eleven patients, who were converted from VATS to thoracotomy, and 2 patients, who were converted from SpRS to thoracotomy due to bleeding, were not included in the study. In the study, only 1 surgeon used the SpRS technique in lung resections, while the other 5 surgeons used the VATS technique for lung resection.
In the study, patients' demographic characteristics, histopathological characteristics, surgical techniques, operation duration, the number of lymph nodes dissected, and the amount of bleeding were compared. The ethics committee approval of the study was obtained from the local ethics committee of our hospital (Decision No: 2022-194).
Preoperative evaluation
Contrast-enhanced thorax computed tomography (CT) was ordered for all patients. Positron emission tomography (PET-CT) and cranial magnetic resonance imaging were ordered to evaluate the distant metastases and mediastinal clinical staging of patients. The mediastinal staging was performed by endobronchial ultrasonograph and/or mediastinoscopy in patients with adenocarcinoma with mediastinal lymph nodes of ≥1 cm or with positivity in hilar or mediastinal lymph nodes on PET-CT, with a tumor diameter of ≥3 cm and with adenocarcinoma. Mediastinoscopy was applied to patients with suspected PET positivity in mediastinal lymph nodes.
The preoperative respiratory capacity of patients was evaluated using the pulmonary function test and/or carbon monoxide diffusion capacity. The cardiac electrocardiogram and, if necessary, echocardiographic examination were performed. All patients were ordered to have a PCR swab before the operation due to COVID-19 pneumonia. Patients with negative swabs were operated on, whereas patients with positive swabs were re-evaluated for operation after the treatment process. Charlson comorbidity index was used to assess the comorbidities of patients. The operation decisions of patients were taken by the oncology council.
Surgical technique
The wristed articulated instruments (ArtiSential®) were started to be used in our hospital in March 2021. Surgeons were primarily trained in the dry laboratory. ArtiSential is Food and Drug Administration approved and has a Conformité Européenne mark.
Multiportal and uniportal surgical approaches were used in the VATS technique. Lung resections have been performed with VATS in our clinic since 2013. In the multiportal approach, a 3–5 cm utility incision is made from the fourth anterior intercostal space, while a 2 cm camera port is opened from the posterior seventh intercostal space. In surgeries, vascular structures are cut with the help of an endovascular stapler after being ligated and dissected. A 45 mm endolinear parenchymal stapler was used for parenchyma and bronchial structures. After the operation, the resection material was removed by an endo bag. Systematic lymph node dissection was performed on the patients. Meanwhile, in the uniportal approach, a 3–5 cm utility incision was made in the midaxillary 4th or fifth intercostal space on the right, while a utility incision was made in the fifth intercostal space on the left side (Fig. 1).
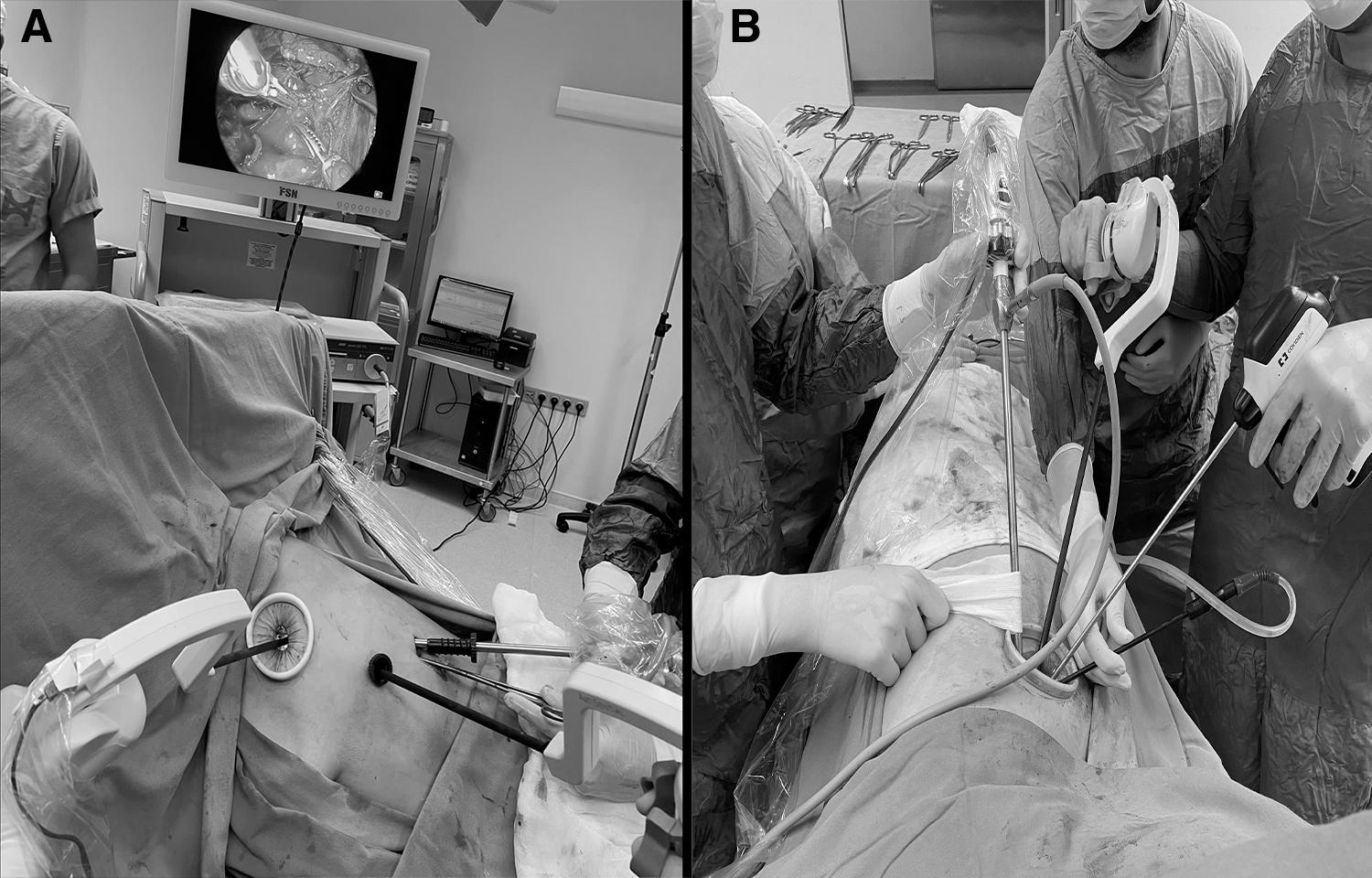
Besides, in the SpRS technique, the single-incision approach and the multiple-incision approach were used. Operations were performed with 3 ports of the multiple-incision approach. Two wristed articulated instruments measuring roughly 2 cm from the anterior axillary line from the fourth intercostal and seventh intercostal spaces were used (ArtiSential; LivsMed) (Fig. 2A). In 5 patients who underwent a multiportal approach on the right side, there were also patients who underwent a subcostal 3 cm incision instead of the seventh intercostal space.
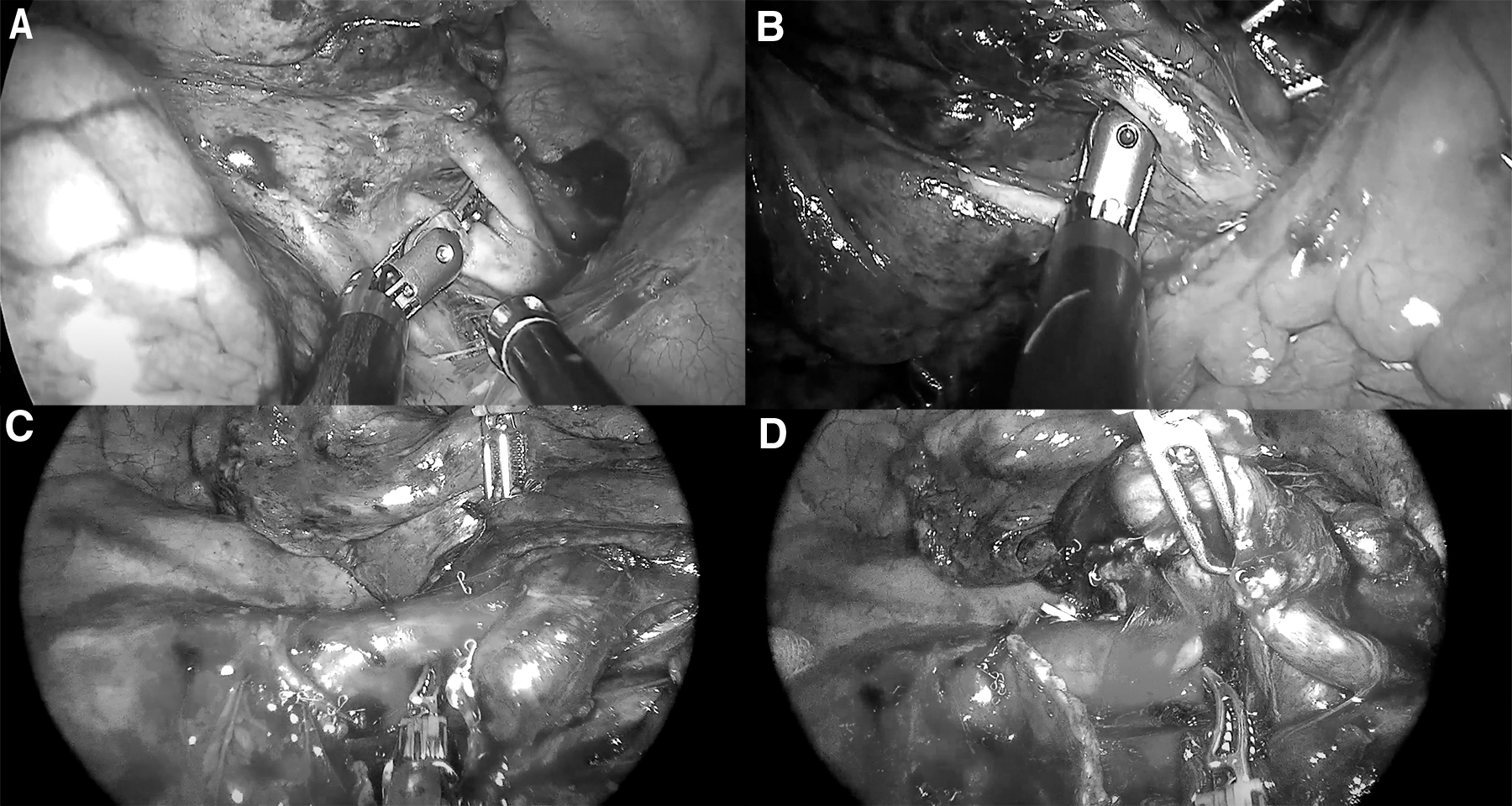
Exposure was achieved from the posterior axillary line with a 30-degree 10 mm optic. Bipolar forceps and bipolar Maryland were used in the operations. In the Uniportal SpRS technique, a utility incision of nearly 3–5 cm was made from the fifth intercostal midaxillary space on the right and left sides (Fig. 2B). In the operations, bipolar forceps and one of the bipolar Maryland instruments were used depending on the surgeon's preference. Similar to VATS, endoscopic staplers were used. Systematic lymph node dissection was performed on the patients.
Postoperative follow-up
Prolonged air leak (>5 days), empyema, wound infections, atrial fibrillation, and hemorrhage that occurred in the first 30 days postoperatively were considered to be complications, while deaths that occurred in the first 30 days were considered to be mortality. Major complications were accepted as pneumonia and hemorrhage, while minor complications were accepted as prolonged air leak, atrial fibrillation, and wound infections.
Statistical analysis
Numerical variables were evaluated using the mean and standard deviation or median, interquartile range; categorical variables were evaluated using numbers and percentages. Parametric assumptions (normality and homogeneity of variances) were tested before comparing numerical variables between the groups. Continuous variables were compared using the Mann–Whitney U test. Statistical analyses were performed using IBM SPSS for Windows version 22.0. The level of significance was accepted as P < .05.
Results
Of the 122 patients included in the study, 76 (62.3%) were female and 46 (37.7%) were male. The mean age of patients was 60.9 ± 9.7 years. There were 41 (33.6%) patients ≥65 years of age. Lobectomy was performed in 112 patients (91.8%), and segmentectomy was performed in 10 patients (8.2%). While 60 (49.2%) patients were operated on the right side, 62 (50.8%) patients were operated on the left side. The mean hospitalization duration of patients was 5.80 ± 3.7 days. The median duration of hospitalization was 5 days in patients who underwent VATS, while the median duration of hospitalization was 4 days in patients who underwent the SpRS technique. No significant difference was found between the groups when demographic characteristics were compared with surgical techniques. A comparison of demographic and clinical characteristics of patients included in the study is presented in Table 1.
Comparison of Demographic Characteristics
CCI, Charlson comorbidity index; IQR, interquartile range; SpRS, surgeon-powered robotic surgery; VATS, video-assisted thoracoscopic surgery.
While 27 (22.1%) patients were operated on with the uniportal approach, 79 (64.8%) were operated on with the biportal approach. Resection was performed from 3 ports in 16 (13.1%) patients. While 11 patients who underwent SpRS were operated on with the uniportal approach, 16 patients were operated on with the triportal approach. Patients who were operated on by VATS were most frequently operated on with the biportal approach, while patients who underwent resection by SpRS were most frequently operated on with the triportal technique (P < .001).
There were 67 patients in the VATS group with stage 1, while there were 23 patients in the SpRS group (P = .309). The median drainage was 125 cc in the SpRS technique, and it was 150 cc in patients who underwent resection by VATS (P = .165). No difference was detected between the groups in terms of histopathological characteristics (Table 2). The mean operation time is 110.4 ± 37.7 minutes. While the mean operation time was 108.3 ± 38.8 minutes in the VATS group, it was 117.4 ± 33.2 minutes in the SpRS group (P = .154). All patients underwent complete resection.
Comparison of Surgical and Histopathological Features
IQR, interquartile range; pStage, pathological stage; SpRS, surgeon-powered robotic surgery; VATS, video-assisted thoracoscopic surgery.
Twenty-three complications were detected in 17 patients (13.9%). Major complications occurred in 3 patients (25%), while minor complications occurred in 14 patients (11.5%). Atrial fibrillation occurred in 4 patients, which improved with medical treatment, wound infection in 3 patients, a persistent air leak in 8 patients, pneumonia developed on the fifth postoperative day in 1 patient, and hemorrhage requiring revision occurred in 2 patients. While 8 of 13 persistent air leaks resolved spontaneously, air leaks were stopped in 5 after blood pleurodesis. No significant difference was found between the groups in terms of complications. Table 3 shows a comparison of complications. Mortality was observed in the first 90 days in 2 patients who underwent VATS. One patient died due to COVID, and 1 patient died due to pneumonia during chemotherapy.
Comparison of Complications between the Groups
SpRS, surgeon-powered robotic surgery; VATS, video-assisted thoracoscopic surgery.
Discussion
Robotic surgery provides solutions to many limitations of VATS. The most notable advantage of this technique is that multi-joint robotic instruments have much greater mobility, allowing more comfortable surgery in narrow spaces.6,7 On the other hand, robotic systems are still not considered cost-effective since they are remarkably expensive for many hospitals and patients. 3 Yet, in numerous studies on lung cancer, the superiority of the robotic system over VATS could not be determined.8,9 Angled endoscopic instruments have been developed to provide both the advantage of VATS in terms of patient-side working opportunity and cost for the surgeon, as well as the ability and maneuver advantages in robotic systems. In the literature, there is only the review by Trevis et al. 4 Hence, we are of the opinion that this article is the first to compare VATS and robotic surgery in thoracic surgery.
They suggested that in the surgeon-assisted robotic surgery technique, these instruments are easier to reach as they are much cheaper than robotic systems and they are more ergonomic. Dissections are performed easier compared to thoracoscopic surgeries, thanks to the 360-degree mobility of the instruments. While we were starting these surgeries, we preferred the multiport technique primarily. Moreover, as Trevis et al. suggested, the use of a subcostal port on the right allows easier extraction of the specimen in patients who underwent lower lobectomy and allows operations to be performed more easily due to the absence of costal rigidity. Furthermore, it has been revealed that postoperative pain is less in the subxiphoid and subcostal approaches.10–12 Likewise, it is easier to extract specimens and control the instruments in patients in whom we applied the subcostal technique on the right side.
We adapted our technique to the uniportal technique after 16 resections owing to the progress in using these instruments and the preference for biportal and uniportal surgeries in our clinic. The most notable disadvantage of these instruments is the need for a pivot point for the movement of instruments. Hence, we used aspirators or endoscopic graspers to fix the instrument in uniportal surgeries. Thus, vascular and bronchial structures can be rotated more easily using a single instrument in uniportal surgery. However, due to the lack of vessel sealing features, energy devices should be used during the operation, notably if there is too much adhesion in the patient.
In our study, we did not find any difference in terms of hospitalization duration, demographic characteristics, or surgical and histopathological characteristics of our patients who underwent SpRS compared to VATS. We did not find a significant difference between VATS and SpRS, particularly when the lymph node dissection numbers were compared. In the study by Jin et al., 13 the number of harvested lymph nodes was higher (32.6 ± 12.2 versus 24.6 ± 7.4, P < .01) in patients who underwent SpRS compared to thoracoscopic surgery patients.
Besides, when evaluated in terms of hospitalization duration, they stated that the hospitalization duration of patients who underwent SpRS was shorter in patients who underwent mesocolic excision in colon cancers (3.0 ± 1.2, 4.1 ± 2.2, P = .01). In our study, however, no significant difference was found in terms of the duration of hospitalization. However, in the study performed by Kim et al., 14 no difference was found between early oncological outcomes in gastric cancers that underwent gastrectomy. There was no significant difference in operative time, in terms of the number of retrieved lymph nodes and length of hospital stay. In addition, when the amount of intraoperative bleeding was compared in our study, no significant difference was found between the groups.
The most remarkable difficulty of the SpRS technique is the inability to use more than one robotic arm at the same time in patients using a single incision. In the study, the biggest problem in operations performed with a single incision was reported as the collision between the instruments. 14 According to our experience, in the uniportal technique, a Maryland dissector for dissection and aspirator or thoracoscopic ring clamp is sufficient for lung traction. However, if two multi-joint wristed instruments are used through a single incision, a severe collision occurs because of the instrument's arch.
The most notable bias in the study is that, although the operator using the instrument has more than 200 VATS lung resection experience, ArtiSential is a new device, and a learning curve cannot be avoided when a new surgical instrument is introduced. Hence, we think that instrument adaptation should be conducted with a dry laboratory or wet laboratory before surgery. When we compare the operation durations of VATS and SpRS techniques, no significant difference was found in terms of operation duration, although the learning curve for new instruments is reported to be 50 cases in the literature.
Study Limitations
This study has several limitations. These limitations are as follows: first, the small number of patients studied; second, it was retrospective; and finally, the fact that more than 1 surgeon performed the operations in the VATS group also causes additional limitations to the study. In addition, the fact that the SpRS technique was used by only 1 surgeon increases the bias in the study.
Conclusions
In conclusion, we think that multi-joint wristed instruments eliminate rigidity and maneuverability problems in thoracoscopic operations. Moreover, our study results show that it is an effective and reliable method with early results similar to thoracoscopic surgery. We think that developing these technologies will help us to operate on patients with small incisions and will lead us to microinvasive surgery instead of the minimally invasive surgery concept in the future. However, additional prospective and extensive studies are still needed.
Footnotes
Authors' Contributions
All authors have agreed to the submission of this article in its present form. There is no conflict concept: C.B.S., M.M., G.T., M.V.D., and S.E. Design: C.B.S., V.E., Y.S., M.V.D., and G.T. Data collection and/or processing: C.B.S., M.M., S.E., and G.T. Analysis and/or interpretation: C.B.S., M.M., and V.E. Literature research: C.B.S., G.T., Y.S., and M.M. Writing: C.B.S., G.T., S.E., and V.E.
Disclosure Statement
The authors do not have any conflict of interests in this article.
Funding Information
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.