
Abstract
Purpose:
Left-handed (LH) surgeons face unique challenges in their training and practice. Contrary to the historical and unjust perception of technical inferiority, LH surgeons can thrive under appropriate mentorship and support. Here, we describe modifications to pediatric minimally invasive surgeries to benefit the LH surgeon.
Methods:
The surgical approaches to common and complex pediatric surgical operations were modified to facilitate training of an LH pediatric surgical fellow.
Results:
Preoperative preparation, including communication with the operating room team, patient positioning, and provision of appropriate equipment, allowed the procedures to be accomplished in a safe and efficient manner.
Conclusions:
Modifying complex minimally invasive surgery to allow for use of the dominant hand is feasible and safe.
Introduction
Approximately 10
LH medical students, residents, and surgeons report frustration or perceptions of discrimination during their training and beyond.2,4,8–10 Most material components that are used in surgery are designed with a lateral bias toward the right-handed (RH) operator.2,6,8,10–13 Whereas previously it was thought that laparoscopy somewhat mitigated these disadvantages, this has not proven to be the case.14–16 Previous reports have demonstrated a need for mentorship and education for LH surgery trainees. 4
Despite growing literature to address handedness in surgical training, there are no reports of modifications to standard pediatric surgery operations for the LH surgeon. In a field where laparoscopy and thoracoscopy are performed in neonates as small as 1–2 kg, dexterity, fine motor movements, accuracy, and precision are of utmost importance. Therefore, it would be advantageous to adjust port placement and the surgical approach to facilitate dissection and suturing utilizing the surgeon's dominant hand. In this study, we describe LH approaches to both common and complex pediatric minimally invasive procedures.
Methods
Modifications for pediatric surgery
The LH pediatric surgery fellow was mentored during a 2-year fellowship to modify simple and complex cases to facilitate the primary use of the left hand for intricate movements and dissection. We began with simpler cases such as laparoscopic appendectomy and pyloromyotomy, which were modified simply by utilizing the dominant hand for dissection and the nondominant hand for retraction. Positioning and port placement were adjusted to an LH approach for more complex cases such as fundoplication, intestinal anastomoses, and hepatobiliary cases. We consider antireflux surgery one of the milestones in minimally invasive pediatric surgery training, as it combines dissection, cautery, and intracorporeal suturing and knot-tying in an infant. These skills can be modified and translated to other complex minimally invasive operations.
Staged approach
As a methodical approach with increasing difficulty, we chose to start the program with high-frequency, low-complexity procedures such as laparoscopic pyloromyotomy and appendectomy. Over the course of the program, the complexity of the procedures increased and peaked at the level of thoracoscopic repair of esophageal atresia, lung lesions for lobectomy, and laparoscopic resection of cystic biliary disease with intracorporeal reconstruction of the biliary tract.
We present the modifications necessary for the LH surgeon for each of the procedures. For each procedure, we describe the port placement, RH approach, and LH modifications, followed by tips and pearls. Adjustments range from simply switching the instrument into the dominant hand to shifting of approach angles to improve ergonomics.
Results
Laparoscopic appendectomy
Description of technique for the RH surgeon
There are a large variety of port options used by surgeons to perform multiport or multi-instrument single-incision laparoscopic appendectomies. The commonality of these approaches for the RH surgeon lies in that the RH surgeons typically retract the appendix with the left hand and dissect with the RH.
Modifications for the LH surgeon
Port placement: Same as RH surgeon
Dissection: The appendix is retracted with the RH and the dissection performed with the LH in a crossed manner.
Pearls and tips:
The single-site approach is advantageous and intuitive for the LH trainee in this situation, as this technique already requires the crossing of instruments.
Laparoscopic pyloromyotomy
Description of technique for the RH surgeon
Positioning: Frog-leg position at the foot of the bed or transverse to allow the operating surgeon to stand at the patient's feet.
Port placement: 3–5 mm umbilical port with stab incisions in the right upper quadrant (RUQ) and left upper quadrant (LUQ).
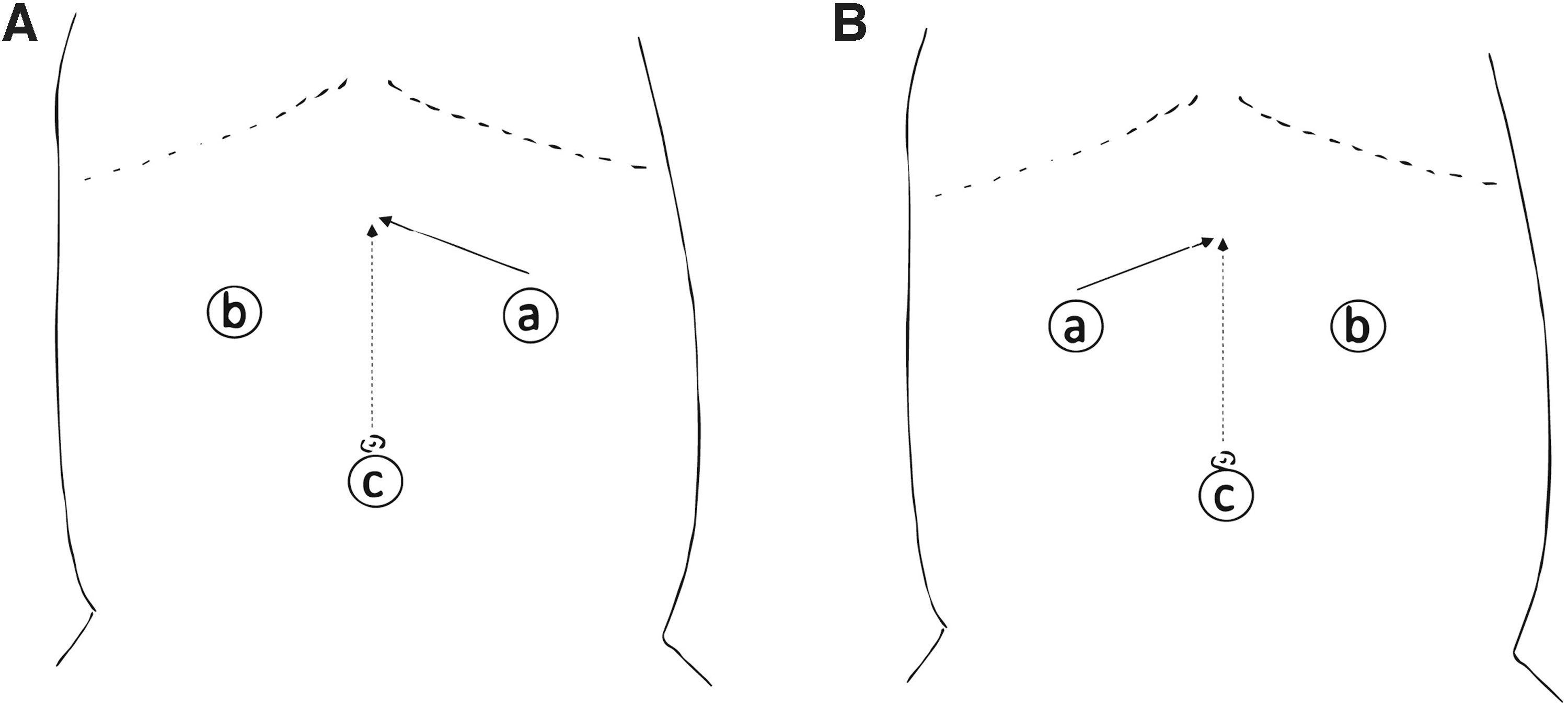
Dissection: The pylorus is grasped and stabilized from the duodenal side using an atraumatic clamp inserted into the RUQ incision. A shielded electrocautery device is inserted through the LUQ incision. Following the initial myotomy, the electrocautery device is exchanged for a pyloric spreader (Fig. 1A).
Positioning and port placement for
Modifications for the LH surgeon
Positioning and port placement: Same as RH surgeon
Dissection: The instruments are reversed, with the cautery/spreader inserted into the RUQ incision and the atraumatic clamp into the LUQ incision to grasp from the stomach side (Fig. 1B).
Pearls and tips:
Switching the grasper into the surgeon's right hand can sometimes leave the liver obscuring the view. Adjusting by pulling the pylorus out toward the anterior abdominal wall in the LUQ or toward the patient's feet can improve the view. Alternatively, a transcutaneous stitch to retract the falciform ligament and suspending the liver anteriorly can be beneficial.
Laparoscopic Nissen fundoplication
Description of technique for the RH surgeon
Positioning: Frog leg in infants/small children, or lithotomy in an older child. Patient at the foot of the bed with surgeon and assistant on surgeon's right side.
Port/instrument placement: Camera port in the umbilicus, with working ports along the left and right midclavicular lines to facilitate retraction and dissection by the primary surgeon. A flexible tip retractor is inserted via a lateral RUQ stab incision just below the liver edge and used to elevate the left lobe of the liver. An additional working port is then inserted into the left lower quadrant (LLQ) for retraction by the assistant surgeon.
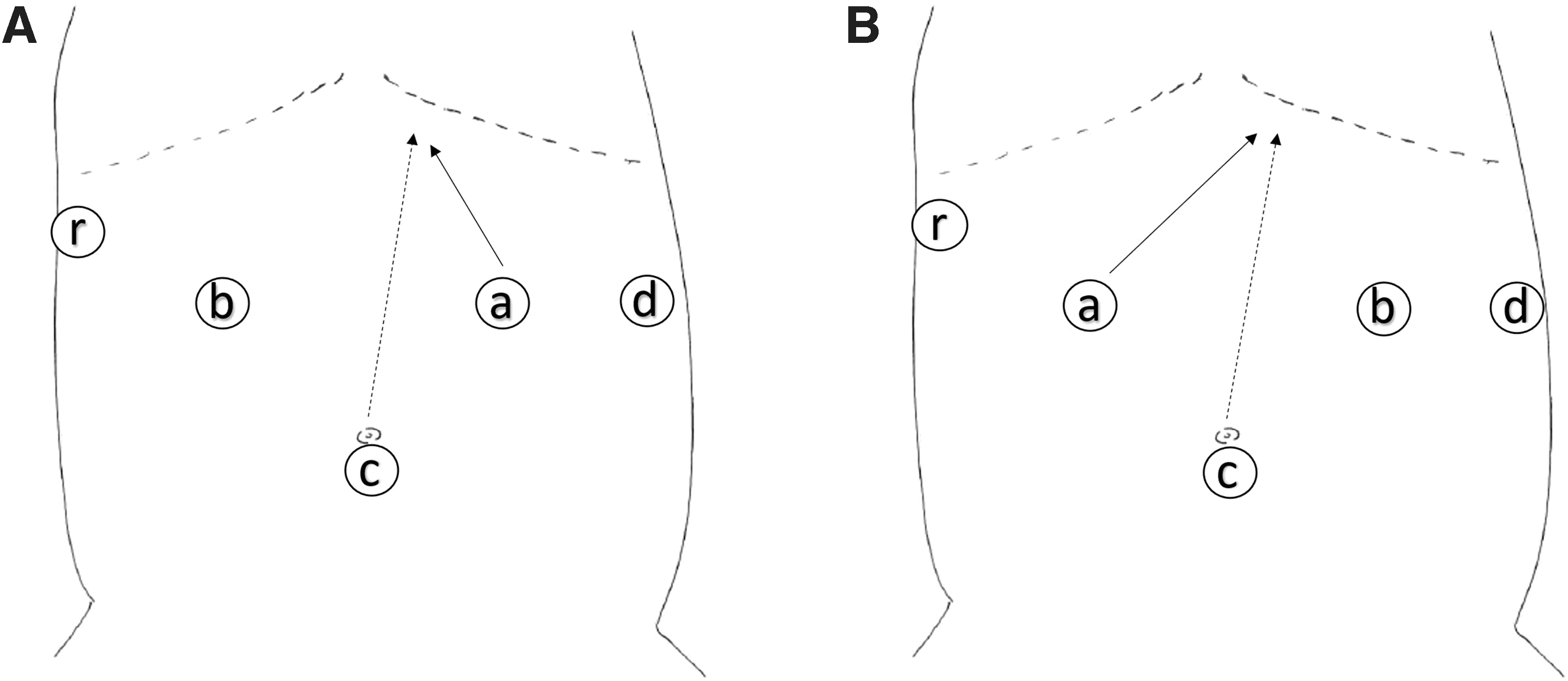
Dissection: RH via the left midclavicular port is used for dissection. The assistant typically retracts the spleen laterally and the surgeon retracts the stomach toward the patient's right hip. The retroesophageal window is created and the fundus brought through the window with the surgeon's LH. The fundoplasty stitches are done with the RH and go in a left to right direction. Occasionally the fundus may slip posteriorly while the RH surgeon is placing the first stitch (Fig. 2A).
Positioning and port placement for
Modifications for the LH surgeon
Positioning/port placement: Same as RH approach.
Dissection: The division of the short gastrics is done by the surgeon's LH. The surgeon's RH is used to retract the spleen laterally and the first assistant retracts the stomach toward the right hip. The retroesophageal window is created and the fundus brought through the window with the surgeon's LH. The fundoplasty stitches are done with the LH and go in a patient's right to left direction. In this scenario, the fundus is less likely to slip during this maneuver (Fig. 2B).
Pearls and tips:
A degree of ambidexterity is advantageous here if the trainee is comfortable dividing the vessels also with their RH while the assistant retracts the spleen.
The retroesophageal dissection is much more intuitive for the LH trainee. The angle allows an approach that minimizes dissection into the mediastinum.
Due to the LH approach with the fundoplication stitches, care must be taken not to injure the liver with the back of the needle.
Laparoscopic duodenoduodenostomy
Description of technique for the RH surgeon
Positioning: Frog leg or lithotomy in an older child. Patient at the foot of the bed with surgeon and assistant on surgeon's right side.
Port/instrument placement: Camera port in the umbilicus, with working ports along the left and right midclavicular lines to facilitate retraction and dissection by the primary surgeon. A flexible tip retractor can be inserted via a lateral RUQ stab incision just below the liver edge and used to elevate the left lobe of the liver if needed. Alternatively, in neonates, a falciform stitch to suspend the liver can also aid visualization.
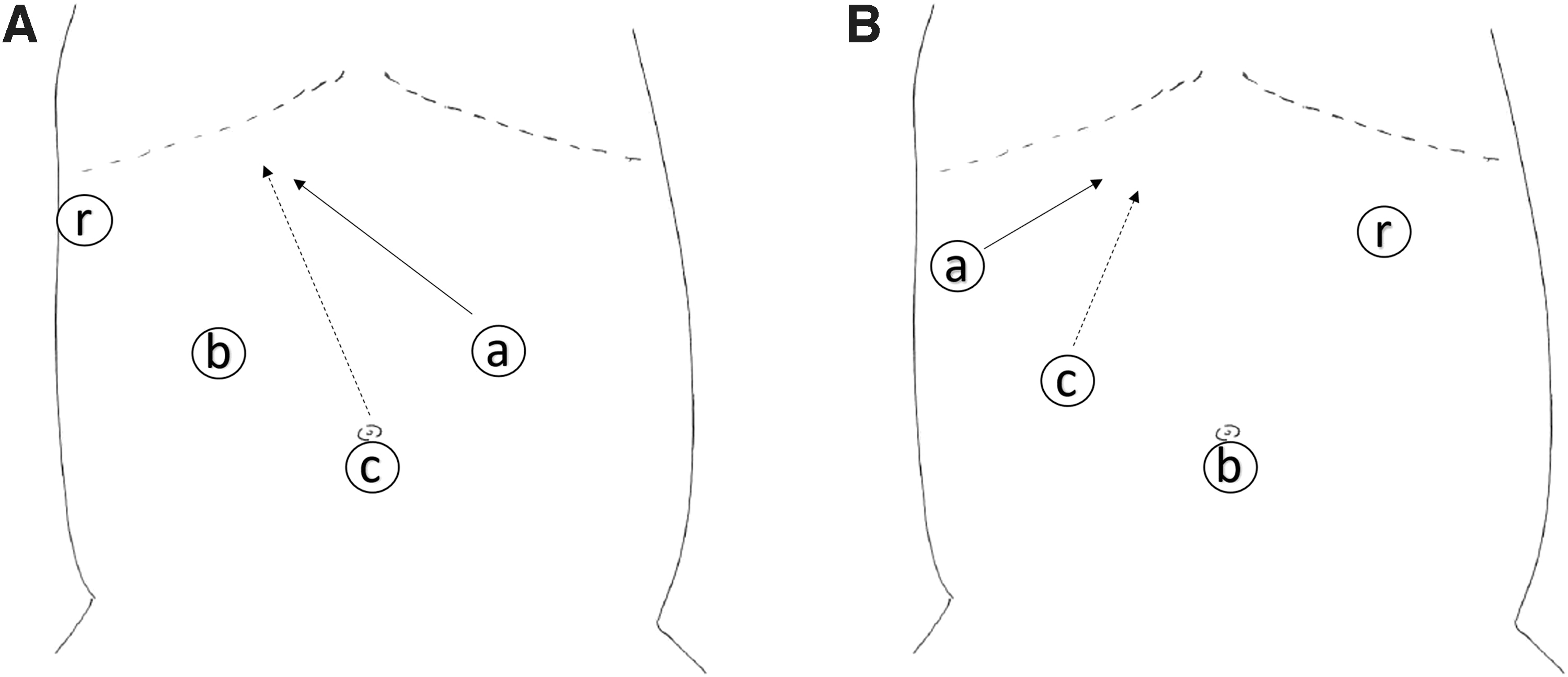
Dissection: RH via the LUQ or epigastric port, which may require crossing the hands. The anastomosis is made via intracorporeal suturing, stapling, or exteriorizing the duodenum through an extension of the umbilical incision (Fig. 3A).

Positioning and port placement for
Modifications for the LH surgeon
Positioning: place the patient in the right lowermost area at the foot of the bed in frog-leg position.
Port placement: place ports in the right side of the patient, to look toward patient's left shoulder. Place the self-retracting suture to line up the anastomosis in the LUQ (Fig. 3B).
Pearls and tips:
This approach allows for unencumbered use of the LH for dissection and suturing. Depending on the size of the patient and location of the atresia, the self-retaining suture to line up the two ends of the duodenum may need to be adjusted.
Regardless of surgeon preference on the method of duodenoduodenostomy, the adjusted port placement allows for more ergonomic dissection and mobilization of the duodenum.
Laparoscopic choledochal cyst excision and hepaticoduodenostomy or hepaticojejunostomy
Description of technique for the RH surgeon
Positioning: Frog leg or lithotomy in an older child. Patient at the foot of the bed with surgeon and assistant on surgeon's right side.
Port/instrument placement: Camera port in the umbilicus, with working ports in the left and right midclavicular lines. A flexible tip retractor can be inserted via a lateral RUQ stab incision just below the liver edge and used to elevate the left lobe of the liver if needed. Alternatively, in neonates, a falciform stitch to suspend the liver can also aid visualization (Fig. 4A).
Positioning and port placement for
Modifications for the LH surgeon
Positioning: Standard supine for the older child; to the right lowermost area at the foot of the bed if infant.
Port/instrument placement: A 4 mm umbilical port is inserted. Two 3–4 mm working ports for the surgeon are inserted in the RUQ, with the RH port located in the midclavicular line superior and lateral to the umbilicus and the LH port in the lateral RUQ just inferior to the liver edge. Utilization of the 4 mm port allows for the 4 mm camera to be moved to the right midclavicular port depending on the ease of visualization and operative space. Suturing and cautery are carried out using the left hand, with retraction performed by the right. A lateral LUQ 3 mm is placed for retraction by the assistant (Fig. 4B).
Pearls and tips:
Placing the patient on a bump with the right side up can help place ports laterally.
Dissection from the patient's right allows for good visualization of the portal vein.
Suturing the hepaticoduodenostomy or hepaticojejunostomy using the left hand comes at a more ergonomic angle from the RUQ port.
Thoracoscopic lobectomy
Description of technique for the RH surgeon
Positioning: Lateral decubitus position, with camera port in the midaxillary position. Operative ports are then placed under direct vision in the anterior axillary line (Fig. 5A).

Positioning and port placement for
Modifications for the LH surgeon
Positioning: Same as RH approach.
Port placement: This varies depending on the lobectomy to be performed. The general concept is to expose the fissure to allow for the left hand to be in prime positioning for dissecting out the vessels. For a left lower or right upper lobectomy, the approach can still be via the working ports in the anterior axillary line to allow the right hand to retract the lower lobe inferiorly, and delicate dissection carried out using the left hand instruments. Adjustments can be made for the left upper or right lower lobes, including approaching the dissection from a slightly posterior positioning. For the left upper lobe, placing the working ports inferior and looking toward the apex can allow for a more favorable ergonomic position. Likewise, for the right inferior lobe, a more superior positioning of the trocars allowed for easier use of the dominant left hand instruments (Fig. 5B).
Pearls and tips:
Creativity with triangulation yielded the most success in making adjustments for this operation. Placement of a fourth 3 mm port when needed or moving the port a rib space in a neonate allowed for easier dissection depending on the patient's anatomy and size.
Thoracoscopic tracheoesophageal fistula and esophageal atresia repair
Description of technique for the RH surgeon
Positioning: Semiprone position, with a roll placed under the left axilla. The camera port is placed below the inferior tip and slightly anterior to the scapula. The working ports are placed for the left hand posterior to the camera and the right hand anterior and superior to the camera (Fig. 6A).

Positioning and port placement for
Modifications for the LH surgeon
Positioning: Same as RH approach.
Port placement: The camera port is placed slightly more anterior to the scapula, and one rib space superior to the RH approach, if needed. This allows the left hand working port to be placed slightly inferior to the camera and at the midaxillary line. In this position, dissecting out the structures and suturing the anastomosis are slightly less cumbersome (Fig. 6B).
Pearls and tips:
Suturing the esophageal anastomosis in a neonate thoracoscopically can be a challenge. To optimize the approach, where suturing will now take place from inferior to superior, requires the left hand to be placed less inferiorly and more anteriorly. This positioning of the trocars can make it difficult to have an optimal angle for dissecting out the fistula or the upper pouch. If this is the case, do not hesitate to place a fourth trocar, or move the left hand trocar to an adjacent rib space, which can often be performed in a neonate without making a new skin incision.
Discussion
LH surgeons face unique challenges in training and practice compared with their RH colleagues. Although 10%–12% of the general population is LH, we nevertheless exist in a world with lateral bias.2,12 Many devices and instruments are designed for RH use, and this extends into the operating room.12,13 As many as 24% of LH surgeons perceive a significant disadvantage based on handedness. 1 There also exists a degree of discrimination toward LH trainees as being perceived as inferior or a burden,1,4,10,11,17 sometimes forcing the LH surgeon to become RH or ambidextrous. 11 However, when studies are designed to account for handedness, this difference does not persist. 7 Studies that have assessed attempts at training the nondominant hand have found that the quality of performance is not the same.10,18,19
Importantly, whereas LH surgeons were historically considered technically inferior,4,8 skills-based evaluations have shown this not to be the case.1,6,7 The training environment, attending surgeon hand dominance, mentorship, and hand-specific teaching, each plays a significant role in addressing any disparities. 4 In a study of first-year medical students performing routine tasks such as suturing, laparoscopy, venous cannulation, and urinary catheterization found no differences in performance between LH and RH students. They conclude that surgical skills are not due to innate dexterity but the academic environment in which the students are trained and evaluated. 6
There is increasing recognition of these biases, and attention is being paid to the importance of LH-specific training and mentoring. Despite the data, there is still work to be done. Among the training programs surveyed in the NYC area, only 3% of LH surgeons receive laterality-related mentoring. Only 10% of LH attending surgeons provided mentorship to LH residents, and 13% have LH instruments. 8 A Turkish surgical society survey of 194 respondents found that none was offered mentoring regarding laterality, only 11% used LH instruments, and 47% believed endoscopic surgery should be modified for the LH endoscopic surgeon. 16 To this effect, primers on how to operate with an LH trainee have been published in cardiac surgery 12 and for specific operations within general surgery. 9
Challenges in teaching LH trainees appear to be more significant for RH teachers than their LH counterparts, and this is likely due to being unaware of the adaptations required of the LH surgeon. Reported issues include preoperative planning, intraoperative skills, to techniques for closing. RH teachers had more difficulty (46% versus 16%, P = .003) and less comfort (28% versus 4%, P = .002) teaching LH residents, and 15% thought LH trainees were technically less skilled than their RH counterparts. 4 They found that there were challenges translating technique to LH trainees, and physical limitations of an environment optimized for RH mechanics.
LH trainers were more likely to describe an LH trainee as having greater technical ability (18.9%), but overall they reported that 42.7% of LH surgeons had difficulty with utilizing tools and 62.7% alter handedness to accommodate for these difficulties. 1 27.8% of respondents reported decreased difficulty and 39.9% reported fewer required adjustments if the teacher was also LH.
Laparoscopy was thought to minimize or eliminate many of the difficulties encountered in open surgery, including right-hand-specific instruments, switching sides of the bed to improve ergonomics, and need for procedure modification. However, 6 of the 18 LH surgeons in the Turkish Society of Surgery survey responded that they had difficulty with endoscopic scissors, grasper, dissector, and/or endoclip. 16 Therefore, the need for LH-specific modifications and instruments extends to minimally invasive surgery where the use of the surgeon's dominant hand is preferred for efficiency, accuracy, and precision. No surgical manual with emphasis or mention of the LH approach with regard to laparoscopy exists at this time. 2
Robot-assisted laparoscopy may be beneficial in mitigating differences attributable to handedness. Multiple studies have shown the benefit of robot-assisted laparoscopy on fine motor skills of the nondominant hand.20–22 Measuring Fundamentals of Laparoscopic Surgery curriculum tasks completed by surgical novices (medical graduates with no robotic/laparoscopic experience), surgeons in training (postgraduate year 3–4 residents and fellows with intermediate robot and laparoscopy experience), and advanced surgeons (extensive experience) showed that the between-hand performance time difference was negligible when utilizing the robot system (374.4 seconds versus 399.7 seconds, P = .48). 20 The advantage in performance was especially significant in the novice and intermediate-experience groups. Unfortunately, at this time a platform small enough for neonates and children does not yet exist. 21
Preparation and communication can overcome many of the issues in the operating room to avoid complexity, variability, and reduce the potential for error. Preoperative planning with the operating room team, specifically the scrub nurse/technologist, to ensure proper instrument availability such as LH instruments and loading of needles in the proper orientation can lessen missteps or delays. 11 The attending surgeon should be notified or reminded of the trainee's handedness before the start of the operation if any modifications to positioning of the patient or surgeon side, or adjustments to intraoperative steps are required. 12 Preparation, mentorship, and modifications allowing for the surgeon to operate at their maximal potential despite handedness of the trainee and the trainer can only lead to a more supportive learning environment and success to the LH surgeon, which should lead to improved operative time, efficiency, and patient safety. Further studies are needed to extrapolate from simulation studies.
There is debate on whether LH or RH surgeons are more ambidextrous, but the advantages of ambidexterity are well documented. Among the neurosurgeons surveyed, Beehler et al. found that LH surgeons are more likely to be ambidextrous in the operating room than their RH counterparts (36.5% versus 13.3%, P < .001). 1 However, training LH surgeons to become ambidextrous does not appear to be the solution. In a study of RH surgeons who were tested on fine motor skills using their LH in a model repair of congenital diaphragmatic hernia, quality/precision was almost, but not quite the same. They note movements were too fast but not economical, implying rough and risky manipulation. They conclude that nondominant hand training, while necessary, is not the same as using the dominant hand. 18
Burdett et al. also note that whereas LH surgeons adapt well in the operating room, there exists a limit to compromise, and thus, a tailored approach to teaching the LH trainee is needed to ensure the precision required in cardiac surgery. 12
Pediatric surgery requires the manual dexterity and precision required in other areas of surgery while encompassing a wide range of cases with open and minimally invasive approaches. Although some operations can favor the LH surgeon, such as a patient with situs inversus, these cases are not common.23–26 We have found that with creativity and ingenuity, the LH surgeon can have innate advantages in certain aspects of pediatric minimally invasive procedures. Due to the small patient size, it becomes essential to orient the trocars in such a way that the surgeon is able to maximize mechanical advantage.
Due to the increased complexity of operating on small neonates and infants, we felt that describing the key concepts of teaching an LH pediatric surgeon would be of value. We do not include all common procedures such as laparoscopic cholecystectomy, which has already been described elegantly by Herrero-Segura et al. 9 As described above, we began our trainee–trainer relationship using a common, low-complexity case (laparoscopic appendectomy) to gain familiarity with instruments and triangulation, as well as to familiarize the RH trainer with the visual aspects of an LH surgeon. As the teaching environment matured, we stepped up to more complex cases.
Many of the adjustments can be basic. In the case of pyloromyotomy, the instruments are flipped and this works well to accommodate use of the dominant hand for the fine motor required to split the muscle.
In other cases, we adjusted the triangulation of the case to favor an LH approach, which allowed us to see that creativity and flexibility were most important to teaching success. Where the trainee stands during these cases can depend on the size of the patient, where the patient is positioned on the bed, the orientation of the room, and the comfort of the surgeon. An example of this is during a laparoscopic Nissen, where some surgeons prefer a frog-leg position and standing at the end of the bed versus standing more to the right side of the patient. Therefore, we did not indicate this on the figures. Overall, many of these concepts can be extrapolated to larger children and adults.
As the trainer–trainee relationship grows, there will be cases that naturally favor an LH or RH surgeon; at times, use of the dominant hand may not be practical. One example that we encountered is the low pelvic dissection involved in a laparoscopic-assisted pull through for Hirschsprung's disease or anorectal malformation with a vesicular fistula, which is typically approached from the right side of the abdomen, especially if there is a colostomy present in the LLQ. Conversely, the retroesophageal dissection during a Nissen fundoplication is well suited for an LH approach. It is our hope that this article will inspire other surgeons to publish their tips and tricks in the future.
As more LH trainees are encouraged to utilize their dominant hand, it is important to address the needs of an LH surgeon performing minimally invasive surgery in infants and children. Realizing that use of the surgeon's dominant hand helps to ensure economy of motion and accuracy in small spaces, we have adapted 7 common or technically challenging pediatric surgery-specific cases. In concordance with previously published reports, we found that laparoscopy was not the great equalizer when it came to overcoming obstacles with handedness. We recognize that this report is by no means comprehensive and hope to inspire other LH surgeons to share modifications to their technique.
Conclusions
Disparities in handedness extend into minimally invasive surgery.
Training LH pediatric surgeons with an emphasis on utilizing their dominant hand is both possible and essential, since the small patient size requires high levels of precision and economy of movement.
Preparation and communication between the LH surgeon and the operating room team can reduce potential error.
Simple adjustment of approach angles can improve ergonomics and facilitate optimal dissection and suturing.
Footnotes
Acknowledgments
The authors wish to thank the patience and enthusiasm of the entire operating room team at Children's Health Dallas for the extra time and understanding required to make this project successful.
Authors' Contributions
J.A.Z. conceived the concept and performed the modified surgeries, drafted the article, and prepared the figures. M.L.R. and S.R.P. supervised the operations, heavily edited the article, and gave final approval of the draft and figures.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.