
Abstract
Background:
The lack of tension at the anastomosis site and the blood flow of the gastric conduit are important to prevent anastomotic leakage in the anastomosis of the esophagogastric conduit. This study reports a gastric conduit stump closure method using Endo GIA™ Radial Reload in end-to-side anastomosis of the esophagogastric conduit, especially focusing on blood flow.
Methods:
A 4-cm conduit was created to ensure an intramural vascular network. The gastric conduit was elevated to the neck through the posterior mediastinal route, and end-to-side anastomosis of the esophagus and gastric conduit was performed using a circular stapler. Closure of the gastric stump with an Endo GIA Radial Reload was performed 2 cm proximal to the anastomosis on the end side of the esophagogastric conduit. The lesser curvature of the stump of the gastric conduit is the most frequent site of anastomotic leakage as it has the least blood flow, and the pressure is highest when the pressure inside the gastric conduit increases. Therefore, the gastric conduit stump was closed using the Endo GIA Radial Reload to resect the intersection of the gastric stump and lesser curvature from which the gastric conduit was created. The gastric conduit stump is gently curved; therefore, the pressure applied to the gastric conduit stump could be dispersed when the intragastric pressure increases.
Results:
No anastomotic leakage was observed among the 21 patients who underwent this method.
Conclusion:
This method is a novel anastomosis method to prevent anastomotic leakage in an end-to-side anastomosis of the esophagogastric conduit.
Introduction
Gastrointestinal anastomosis is the most important procedure in gastrointestinal surgery, in which anastomotic leakage is a serious complication. Data on esophageal cancer surgery registered in the National Clinical Database in Japan revealed that complications were observed in 41.9% of patients, and the incidence of anastomotic leakage was 13.3%, which was the second highest postoperative complication after pneumonia. 1 Postoperative complications lengthen the hospital stay, increase medical costs, reduce activities of daily living, and worsen prognosis.2–4 The ability of surgeons alone to reduce the occurrence of postoperative complications is limited, and preoperative cooperation from a multidisciplinary medical team as well as proficiency in surgical techniques is crucial. 5 This study aimed to present a novel rational anastomosis method using an Endo GIA™ Radial Reload (Medtronic, Minneapolis, MN) to prevent anastomotic leakage in end-to-side anastomosis of the esophagogastric conduit.
Methods
Participants
The technique presented in this study was performed on 21 patients (20 men and one woman; age, 59–82 [median, 75] years) who underwent esophagectomy for esophageal cancer. All patients had a preoperative histological diagnosis of esophageal squamous cell carcinoma. Two patients had upper thoracic esophageal cancer, 16 patients had middle thoracic esophageal cancer, and three had lower esophageal cancer (Table 1). All patients underwent McKeown esophagectomy.
Patient Demographics
TNM, Tumor-Node-Metastasis.
The incidence rate of the supraclavicular lymph node metastasis was ∼20% higher in patients with carcinoma deeper than the muscularis propria; here, supraclavicular lymphadenectomy was useful for accurate pathological diagnosis and improved prognosis in metastatic cases.6–8 Therefore, the McKeown procedure for lower thoracic esophageal cancer is frequently performed as the primary clinical practice in our institution. End-to-side esophagogastrostomy with a gastric conduit, which was elevated through the posterior mediastinal route, was performed at the neck level using a Curve Detachable Head (CDH) circular stapler (Ethicon Inc., Somerville, NJ).
Creation of gastric conduit
Harvesting the gastric conduit and achieving esophagogastric anastomosis without anastomotic leakage require particular attention to the anastomosis technique. 9 The gastric conduit is mainly supplied extramurally by the right gastroepiploic artery and vein. However, since extramural anastomosis between the left and right gastroepiploic artery and vein was not observed in all cases, a 4-cm gastric conduit was created to ensure an intramural vascular network (Fig. 1). 10
The anterior wall of the stomach was pigmented to create a 4-cm gastric conduit.
Gentle extraction of the gastric conduit was performed without grasping the greater curvature of the gastric conduit under laparoscopy. Since the greater omentum may cause congestion after elevation, it was removed 3–4 cm from the right and left gastroepiploic artery and vein. 11 The left gastroepiploic artery and vein were dissected at the root, whereas the short gastric artery and vein were dissected near the spleen. Next, the stomach was pulled up to the cranial side, and the left gastric artery and vein, left inferior diaphragmatic artery cardiac branch, and posterior gastric artery were dissected at their roots.
Since the length of the gastric conduit is defined by the length of the greater curvature, a long gastric conduit can be created by creating a gastric conduit along the curvature of the greater curvature. The Endo GIA Radial Reload can be used as the first stapler to create a 4-cm gastric conduit from the site where two or three branches of the right gastric artery and vein bifurcate into the stomach (Fig. 2).

The Endo GIA™ Radial Reload was the first stapler to create a gastric conduit.
Due to the large curvature in the greater curvature of the antrum, gastric resection by the Endo GIA Radial Reload should be adjusted according to the individual case rather than using the entire 60-mm suture length. A gastric conduit was created using a linear stapler for the second and subsequent stapler because the greater curvature of the stomach on the oral side of the antrum is relatively straight (Fig. 3). After the gastric conduit was created, the entire length of the staple line was sutured with 4-0 polydioxanone (PDS) sutures (Ethicon Inc.) and buried (Fig. 4).

A gastric conduit was created using a linear stapler for the second and subsequent staples.

Completion of gastric conduit creation.
Gastric conduit elevation
An echo probe cover was left in the thoracic cavity at the end of chest manipulation to lift the gastric conduit through the posterior mediastinal route, and the gastric conduit was passed through the echo probe cover and lifted to the neck. Secondary injury to intrathoracic organs and gastric conduit injury can be avoided as contact with other organs can be prevented.12,13
End-to-end anastomosis of the esophagus and gastric conduit
The cervical esophagus was cut relatively short, the anvil head was inserted from the esophageal stump, and a purse-string suture was placed in the esophagus to straighten the esophagogastric anastomosis and position the anastomosis in the neck. The stump of the gastric conduit was then incised, and the main body of the circular stapler was inserted. Stapling was performed by penetrating the trocar of the stapler body and combining it with the anvil head to avoid applying excessive tension (Fig. 5).

The circular stapler was fired, and an end-to-side esophagogastrostomy was achieved.
Closure of gastric stump with Endo GIA Radial Reload
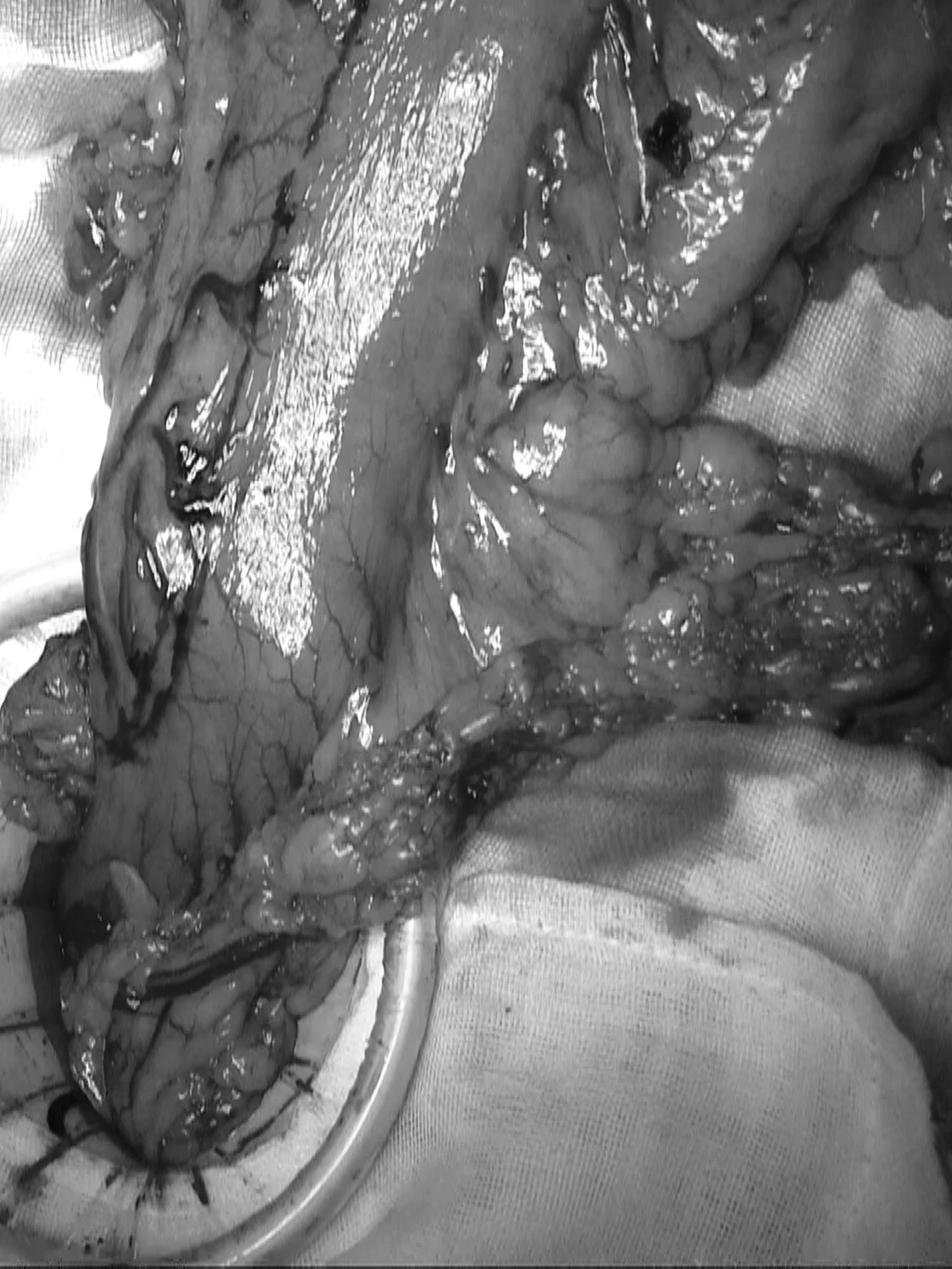
The gastric stump was closed 2 cm proximal to the esophagogastric anastomosis site. The lesser curvature of the stump of the gastric conduit was considered the most frequent site of anastomotic leakage due to decreased blood flow. Furthermore, using a linear stapler to close the gastric conduit stump of the circular stapler insertion causes it to cross the linear stapler of the lesser curvature at the time of gastric conduit creation, which may further reduce the blood flow. The Endo GIA Radial Reload is more suitable than the linear stapler closure of the gastric stump and avoids these problems. Closing the gastric stump with the Endo GIA Radial Reload resects the most hypoperfused area at the intersection of the gastric stump and lesser curvature from which the gastric conduit was created (Fig. 6).

Gastric conduit stump closure using the Endo GIA Radial Reload.
In addition, since a gentle curve is formed in the stump of the gastric conduit, the pressure applied to the stump of the gastric conduit can be dispersed as much as possible when the pressure inside the gastric conduit rises. The staple line of the Endo GIA Radial Reload was reinforced with 4-0 PDS sutures, and end-to-side anastomosis of the esophagogastric conduit was completed (Fig. 7). The Endo GIA Radial Reload may be difficult to handle; however, insertion of the Endo GIA Radial Reload main body from the patient's left dorsal side enables this procedure to be performed safely in all cases.
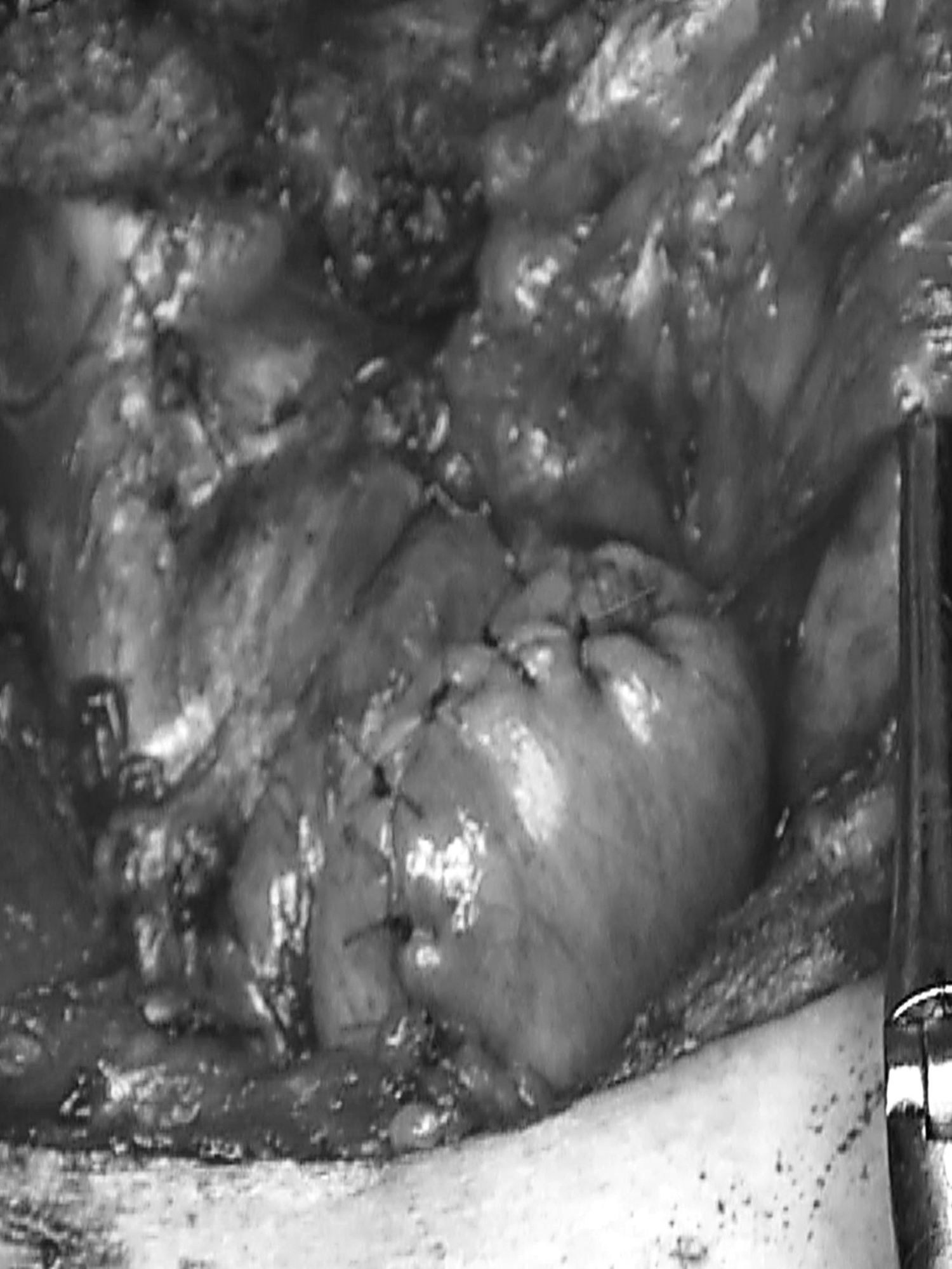
Completion of end-to-side anastomosis of the esophagogastric conduit.
Results
Two patients had an end-to-side anastomosis of the esophagus and gastric conduit using an automatic 21 mm circular stapler (CDH; Ethicon Inc.), and 19 patients with 25 mm CDH at the level of the neck. Gastric conduit creation and stump closure using purple Endo GIA radial reload cartridge were accomplished in all patients without technical difficulties. Furthermore, none of the patients experienced anastomotic leakage (Table 2).
Surgical Results
CD, Clavien–Dindo classification; CDH, Curve Detachable Head.
Discussion
Maintenance of blood flow in the gastric conduit and lack of tension at the anastomosis site were essential conditions to prevent anastomotic leakage in esophageal cancer surgery. 14 However, it is often difficult to achieve both; therefore, many facilities are making various efforts to overcome this. It is possible to create a relatively long gastric conduit with a narrow gastric conduit, but communication between the left and right gastroepiploic arteries and veins has been reported, varying from 23.5% up to 100%.15–19 Blood flow to the gastric conduit varies from case to case. Therefore, since there are few individual differences in the intramural vascular network, a slightly wider gastric conduit is more advantageous than a narrow gastric conduit from the viewpoint of the intramural vascular network.
Furthermore, some facilities preserve the greater omentum as much as possible, but when the gastric conduit is elevated through the posterior mediastinal route, there is little effect on the surrounding organs.12,13 When the gastric conduit is elevated through the retrosternal route, the omental volume causes congestion due to compression. The artery has high blood pressure and shows little change in blood flow before and after elevation, whereas the vein has low blood pressure and is easily affected by compression. However, the space in the thorax is limited, and the hemodynamics in the greater omentum are affected by intrathoracic pressure, even in the case of posterior mediastinal reconstruction. 10 If gastric blood flow is hypoperfusion, revascularization of the neck and gastric vessels is required; therefore, the left gastroepiploic artery and vein are ligated and cut at the root.
The length of the gastric conduit depends on the length of the greater curvature, and a long gastric conduit can be created by resecting the lesser curvature in a gentle curve parallel to the greater curvature. Therefore, we used a curved automatic suture device for the first cut on the lesser curvature. There are two types of anastomosis curved instruments, the CONTOUR™ Curved Cutter (Ethicon Inc.) and Endo GIA Radial Reload.
A major difference between these is that the Curved Cutter provides a suture length of 51 mm, whereas the Radial Reload provides an anastomosis length of 60 mm.20–23 Since the length of the greater curvature of the antrum differs depending on the case, Endo GIA Radial Reload, which has a longer anastomosis length, can adjust the dissection length and create a gastric conduit with a longer curvature. Therefore, in our department, we use the Endo GIA Radial Reload for the first resection on the anal side when creating a gastric conduit. For the second and subsequent shots, a linear stapler was used to create a slightly wider (4 cm) gastric conduit with a preserved intramural vascular network.
There are various anastomotic methods of the esophagus and gastric conduit, such as the Collard method, triangular anastomosis, end-to-side anastomosis using an automatic suture device, and hand-sewn anastomosis. There have been several reports that anastomosis using a circular stapler causes stenosis and is equivalent to hand-sewn anastomosis in terms of anastomotic leakage. Anastomotic leakage due to the use of a circular stapler is reported to be common at the stump of the gastric conduit, caused by the blood hypoperfusion of the gastric conduit. 24 The intersection of the resection line where the lesser curvature gastric conduit was created and the stump of the gastric conduit were the sites where the blood flow was most decreased due to tissue loss from the circular stapler.
Furthermore, the gastric stump is considered to be a site where anastomotic leakage occurs because it has the most pressure when the gastric conduit pressure rises due to an increase in intrathoracic pressure caused by cough reflex during the acute postoperative period. 25 It is essential to decompress intragastric pressure by inserting a nasogastric conduit and devising a method to close the stump of the gastric conduit. Closure of the gastric stump using Radial Reload can resect the lesser curvature where the blood flow is hypoperfusion, and the intersection of the stapler at the gastric stump can be resected with a gentle curve.
Therefore, it is possible to disperse the concentration of pressure due to the gentle curve at the intersection of the stapler, which prevents anastomotic leakage of the stump. Furthermore, the stump of the gastric conduit was reinforced by covering it with excess greater omentum. The residual cervical esophagus is shortened as much as possible to straighten the anastomosis so that it is located in the neck. Opening the neck wound improves drainage and prevents aggravation, even if anastomotic leakage occurs.
This study has some limitations. First, the study included only a few cases. If the incidence rate of anastomotic leakage in accumulating patients was confirmed to be low, it may be possible to remove the nasogastric tube early after surgery. Second, the efficacy and versatility of this method through retrosternal reconstruction were not examined, which is necessary as this study only evaluated gastric conduit reconstruction through the posterior mediastinal route. Third, this procedure is performed only with McKeown surgery. This procedure would be possible for Ivor-Lewis surgery using thoracotomy.
However, in thoracoscopic surgery, Radial Reload makes it difficult to insert it into the thoracic cavity due to its curved nature, and it may be impossible to perform this procedure. Fourth, the blood flow of the gastric conduit was evaluated by indocyanine green angiography, but not after the completion of reconstruction. In the future, we would like to evaluate the blood flow after reconstruction. Finally, we only used a circular stapler of size ϕ25 mm and did not investigate whether other sizes of the circular stapler are effective.
The general and local conditions of the surgical field differ depending on the individual case, even when using the same reconstruction method. Although the safety of surgery has been improved through meticulous perioperative management by coordinating with multiple professionals, the incidence of postoperative complications is ∼40%, which is unsatisfactory. 1 The occurrence of postoperative complications leads to the deterioration of long-term prognosis and quality of life; therefore, complications must be reduced. We aim to continue evaluating both the short- and long-term outcomes of this method.
Footnotes
Authors' Contributions
N.H. was the lead author and surgeon for all the patients. T.M., H.H., T.Y., R.H., K.T., H.Z., T.T., and K.I. were co-surgeons on the cases. T.M. and H.H. contributed in terms of patients and information on the patients. Y.T. reviewed the article and the surgical technique. All authors read and approved the final article.
Availability of Data and Materials
The datasets used and analyzed during this study are available from the corresponding author upon reasonable request.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study received no external source of funding.