
Abstract

Some information presented in this article has been presented as posters in meetings:
Forse, CL, Worley S, Barry JN, Mahajan L, Seifarth FG, Plesec T. Evaluating and defining follicular hyperplasia in the appendixes of children with chronic right lower quadrant abdominal pain. USCAP 108th Annual Meeting, National Harbor, MD, USA; March 16–21, 2019. Available from: https://www.nature.com/articles/s41374-019-0213-1 Forse, CL, Worley S, Barry J, Mahajan L, Seifarth FG, Plesec T. Evaluating and defining follicular hyperplasia in the appendices of children with chronic right lower quadrant abdominal pain. 10th Annual Educational Conference, Cleveland Clinic Foundation, Cleveland, OH, USA; May 16, 2019. Barry J, Forse CL, Plesec T, Worley S, Seifarth FG, Mahajan L. Evaluating and defining follicular hyperplasia in the appendixes of children with chronic right lower quadrant abdominal pain: Clinicopathologic implications. NASPGHAN, Annual Conference, Denver, CO, USA; October 24–27, 2018.
Abstract
Introduction
A
The generally accepted definition of chronic abdominal pain in research requires at least three pain episodes over a minimum of 3 months, interfering with social, athletic, or academic life. In clinical practice, daily pain for longer than 1 or 2 months in duration can be considered chronic.1–3
Of all patients suffering from abdominal pain, it is estimated that chronic abdominal pain accounts for 2%–4% of pediatric outpatient visits. 4 “Chronic or recurrent appendicitis” is a controversial diagnosis believed to cause recurrent right lower quadrant (RLQ) abdominal pain and is attributed to infectious or inflammatory appendiceal pathology without a clearly defined histopathological correlate.5,6 Some clinicians suggest a psychosomatic etiology or appendiceal pathology without associated infection such as appendiceal obstruction as contributing factor for chronic RLQ abdominal pain (CAP).
The value of laparoscopic exploration in patients with unclear abdominal pain has been well reported.7–11 Numerous studies postulate a 70%–100% success rate in ameliorating or resolving RLQ abdominal pain with laparoscopic appendectomy.12–14
We report a series of patients who underwent elective laparoscopic appendectomy for focal CAP of unknown origin. Clinical symptoms, presurgical workup, pathology results, and follow-up are presented. Histopathological findings of the removed appendixes of this patient cohort were compared with age-matched controls to identify defining histological characteristics with focus on evaluating appendiceal lymphoid hyperplasia.
Materials and Methods
Patients
After gaining approval by our institutional review board (IRB No. 11-483), we performed a single-center retrospective analysis of prospectively collected data. Medical records were reviewed for 40 pediatric patients who underwent elective laparoscopic appendectomy for daily complaints of focal RLQ abdominal pain lasting longer than 1 month at first presentation or a history of at least weekly focal RLQ abdominal pain for more than 3 months, interfering with daily activities such as school attendance and participation in social or athletic activities. Patients were seen in a 7-year period between February 2008 and October 2015 at a tertiary care institution. All patients were examined and operated on by two pediatric surgeons. Ten patients were excluded due to loss of follow-up or lack of adequate pathology records, resulting in a study cohort of 30 patients. We identified 16 age-matched controls who in the same period underwent concomitant appendectomy during bowel resections for diagnoses other than chronic abdominal pain or underlying inflammatory disorders.
Patients in the CAP group had a history of idiopathic RLQ abdominal pain ranging from 1 to 72 months of duration. All subjects underwent a gastrointestinal (GI) workup with negative results before surgical evaluation and treatment. GI assessment included a combination of the following: imaging (computed tomography [CT], magnetic resonance imaging [MRI], hepatobiliary iminodiacetic acid [HIDA], kidney, ureter and bladder [KUB], upper GI, and ultrasound), capsule endoscopy, upper and lower endoscopies, and laboratory workup. On physical examination, they presented without exception with focal tenderness to palpation at McBurney's point.
Patients were routinely seen in the pediatric surgery office 3–4 weeks after surgery. Subsequent follow-up by phone or in-person was completed 1–178 months after the appendectomy. During follow-up phone calls, patients were asked to rate their pain on a five-point Likert scale with the following ratings: 1 = much worse, 2 = somewhat worse, 3 = no change, 4 = somewhat resolved, and 5 = completely resolved.
Histopathology
The resected appendixes were histologically evaluated by a staff GI pathologist. The appendixes of the 30 children who had chronic RLQ pain were compared with those of 16 randomly selected and age-matched patients without chronic pain, appendicitis, or infectious or inflammatory disorder. The GI pathology department reviewed appendiceal specimens for any significant pathological findings and differences. Furthermore, the degree of lymphoid hyperplasia was determined by measuring the number of germinal centers (GCs) per 5 mm and the greatest diameter of five consecutive GCs using an ocular ruler. Appendixes were only included if they had a complete longitudinal section of the appendiceal tip.
Surgical technique
Transumbilical laparoscopic assisted extracorporeal appendectomy (TULAA) was performed to remove the appendix of all patients in the CAP cohort. TULAA is well established in children. This technique combines the convenience of an open operation with the benefits of a minimally invasive approach. Unlike conventional three-port laparoscopic appendectomy, TULAA requires only one umbilical laparoscopic port to introduce a 10 mm laparoscope with an inbuilt offset 5 mm working channel. The appendix is exteriorized through the umbilicus and extracorporeally amputated. TULAA has been shown to be a quick, cost-effective, and reproducible method with virtually scar-less results.15–17
Statistical analyses
Data were described using medians and ranges or means and standard deviations for continuous variables and counts and percentages for categorical variables. Study groups were compared on demographic and clinical characteristics using Wilcoxon rank sum or t-tests for continuous and ordinal characteristics and chi-square or Fisher's exact tests for categorical characteristics. Study groups were compared on GC using the two-sample t-test, and on GC adjusting for age using two-methods: (1) paired t-test on subjects matched by year of age and (2) ANCOVA regression model for GC by group, age, and group–age interaction.
All analyses were performed on a complete-case basis. All tests were two-tailed and performed at a significance level of 0.05. SAS 9.4 software (SAS Institute, Cary, NC, USA) was used for all analyses. The performance of counting the number of GCs/5 mm for identifying lymphoid hyperplasia was evaluated by calculating the sensitivity (Sn), specificity (Sp), positive predictive value (PPV), and negative predictive value (NPV).
Results
Thirty patients (18 females, 12 males), 4.4–17.5 years (median 14.5 years), with duration of symptoms ranging 1–72 months (median 8.5 months), were reviewed. One patient was excluded due to loss to follow-up, and 9 patients were excluded due to lack of adequate pathology records. Table 1 lists symptoms reported during the preoperative encounter with pediatric surgery. All patients underwent previous GI workup, averaging 0.77 colonoscopies and 0.9 upper endoscopies per patient. Ten patients had a HIDA scan (mean 0.33 scans per patient). Patients had 0–4 CT scans (mean 1.1). Other studies included MRI (mean 0.13), KUB (mean 0.9), abdominal ultrasound (mean 1.6), capsule endoscopies (mean 0.07), and upper GI series (mean 0.23).
Symptoms of Included Patients with Chronic Right Lower Quadrant Abdominal Pain
RLQ, right lower quadrant.
There were no intraoperative complications for any patients included in the study. Three of the 30 patients developed a postoperative surgical site infection (SSI, 10%), defined by clinical findings of incisional infection within 30 days after surgery. While 1 patient with an SSI needed an incision and drainage procedure in the operating room, the remaining patients with an SSI were treated with oral antibiotics to full resolution.
All patients reported a significant improvement of abdominal symptoms postoperatively. At the follow-up time of 1–178 months (median 38.5) after surgery, patients had an average Likert score of 4.7. Only 1 patient reported worsening of his abdominal pain on questioning 39 months later. This patient's appendix showed no pathological alterations, and he was subsequently diagnosed with irritable bowel syndrome.
Table 2 compares study groups on demographic and clinical characteristics. Groups differed significantly not only on GC but also on age and related variables height and weight.
Demographic and Clinical Characteristics
P-values: aKruskal–Wallis test.
Pearson's chi-square test.
Data not available for all subjects. Missing values: weight (kg) = 1, height (cm) = 1, BMI = 6, BMI-for-age percentile = 6.
ANOVA.
ANOVA, analysis of variance; BMI, body mass index; GC, germinal centers; SD, standard deviation.
Of the 30 appendixes, 8 (27%) were found to be unremarkable on pathology. The remaining 22 (73%) showed one or two of the following pathological findings: acute inflammation, congestion, fecalith, fibrous obliteration, focal reactive inflammation, luminal inflammatory cells, reactive lymphoid hyperplasia, and submucosal scarring. Qualitatively, there were no differences observed in inflammation or fibrosis between the two cohorts. There was no evidence of interval appendicitis such as mesenteric fibrosis, serosal adhesions, or subserosal collections of foreign body giant cells.
Children with chronic pain had significantly more GCs per 5 mm than age-matched controls (mean difference: 3.3, P < .001 [95% confidence interval (CI)]). There was no significant difference in the average size of individual GCs. Using a cutoff of ≥9 GCs/5 mm as an assessment for follicular hyperplasia had a Sn of 80%, Sp of 73.3%, PPV of 85.7%, and NPV of 64.7% (Fig. 1). The chronic pain group had significantly higher GC values than the control group. The difference in means (95% CI) was 3.3 (1.6–5.0) (P < .001). Table 3 shows the mean difference in GC between study groups, with 95% CI, and Figure 2 shows corresponding histograms and box plots.
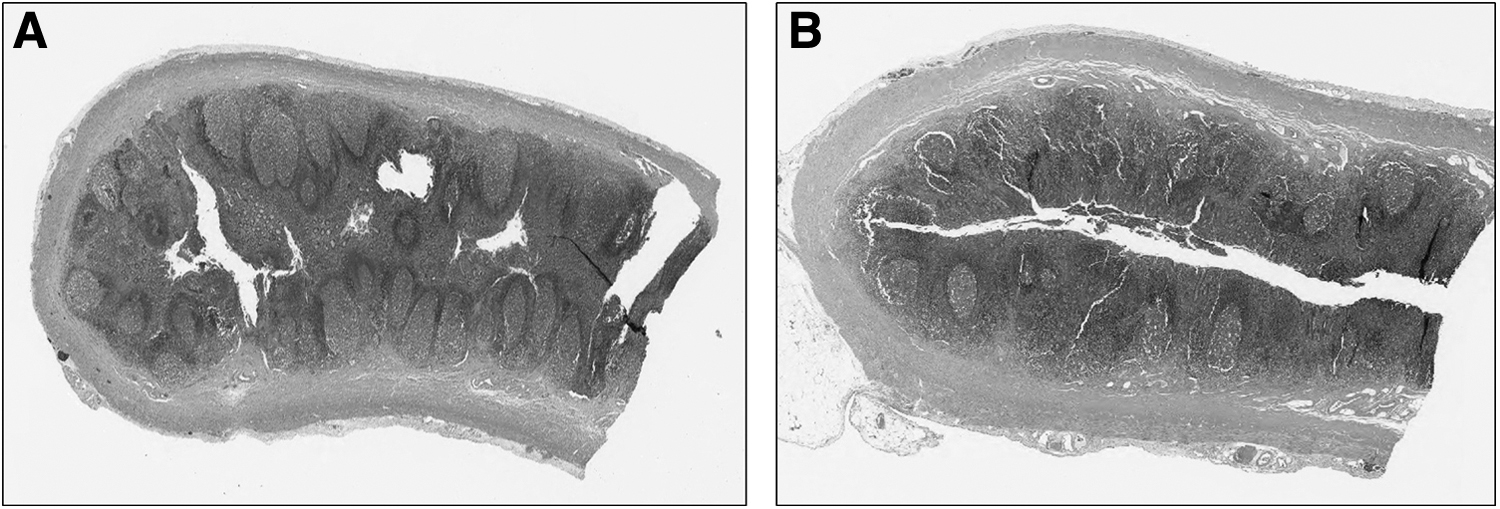
Cross-section of an appendix from a child with
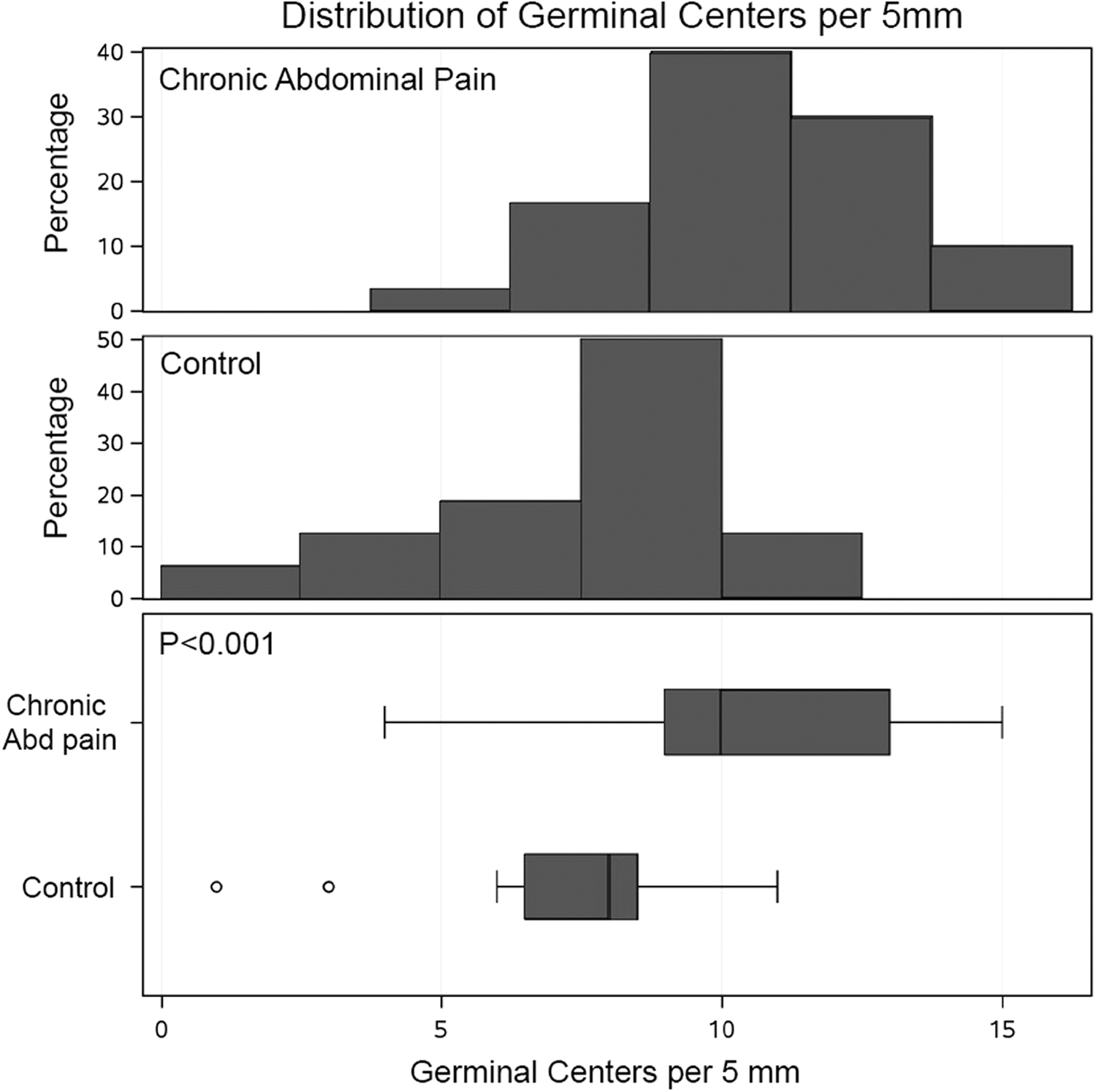
Germinal center distribution histograms (top and middle) and box plot (bottom) demonstrate that there are significantly more germinal centers per 5 mm in the appendixes of children with chronic abdominal pain compared with children without chronic abdominal pain (P < .001).
Two-Sample t-Test for Difference in Germinal Centers Between Groups (N = 46)
CI, confidence interval.
To show that the group difference in GC was not due to the difference in age between the two study groups, patients were matched on age within a 1-year margin. A paired t-test on GC in the 10 pairs of patients who were able to be matched under these criteria was performed. The mean difference was very similar to that found in the two-group analysis: 3.0 (95% CI 0.4–5.6, P = .030).
All patients with ages in the range of overlap between the two groups (ages 4–15 years, N = 29) were analyzed using an Analysis of Covariance (ANCOVA) regression model for GC with predictors age, group, and age–group interaction. The interaction was not statistically significant and removed from the final model, and the results were similar to the two previous analyses: mean group difference 3.1 (9%% CI 1.1–5.1, P = .004).
Discussion
Chronic abdominal pain in children is defined as long-lasting (>3 months), intermittent, or constant abdominal pain of functional or organic origin.1,2 Frequently, no identifiable pathological condition such as an anatomic, metabolic, infectious, inflammatory, or neoplastic disorder can be identified in patients with diffuse chronic abdominal pain. Many patients with focal recurrent RLQ abdominal pain were also grouped under this diagnosis, coined in 1958 by Apley and Naish, who postulated chronic abdominal pain to be a functional problem without an organic correlate. 3
Chronic or recurrent RLQ pain has been attributed to appendiceal luminal compromise, leading to bouts of spontaneously resolving acute appendicitis, or true chronic appendicitis. 11 Since Wangensteen and Dennis' publication in 1939, it has been widely accepted that luminal obstruction of the appendix can lead to acute appendicitis and colicky pain. 3 A high index of suspicion is necessary, however, to identify patients presenting with focal and recurrent RLQ symptoms. Elective appendectomy has been successful in treating children with chronic RLQ pain. 14
In light of the vaguely defined etiologies for CAP, the preoperative workup is exceptionally challenging. Patients with recurrent RLQ pain can present completely pain free at the time of the physical examination. Stevenson 14 reported a 77% rate of positive RLQ physical examination and Chichom Mefire et al. reported an 87% rate. 18 While intraluminal pressure within the appendix may play a role for pain development, it cannot be measured. Imaging of the appendiceal lumen has not been amenable to very detailed imaging. Recent advances in ultrasonography, notably in successfully detecting lymphoid hyperplasia of the appendix, may benefit this patient population in the future. 19
Etiologies for chronic RLQ pain unrelated to the appendix must be kept in mind. A caeco-peritoneal band was postulated by Wong et al. as a potential cause for chronic right iliac fossa pain. 20 In their prospective study, a caeco-peritoneal band was found in 13% and laparoscopically divided resulting in complete long-term resolution of symptoms. 20
The appendiceal histopathology of patients suffering from chronic or recurrent RLQ abdominal pain can show a variety of findings. In 1999, Stevenson reported histological abnormalities of excised appendixes from patients with chronic RLQ pain. 14 They included fibrosis, fecaloma, focal inflammation, and lymphoid hyperplasia as the predominant findings in 30%, 26%, 12%, and 12%, respectively. Chichom Mefire et al. reported a rate of appendiceal fibrosis with subsequent obstruction in 70%–80% of patients with CAP.14,18 In our patient cohort, the rate of fibrosis was not different from that in the control group with only 2 patients showing fibrous serosal or submucosal alterations. We speculate fibrotic changes to be a late finding of chronic inflammation while follicular hyperplasia represents a possible finding of an earlier stage.
The theory of benign appendiceal lymphoid hyperplasia with partial luminal obstruction as a potential cause of appendicitis was first developed in the early 20th century and has been debated ever since. 19 To date, no study has quantified the frequently encountered lymphoid hyperplasia and compared it to an asymptomatic, age-matched control group. The primary pathological finding in our study cohort, reactive lymphoid hyperplasia as defined by ≥9 GCs/5 mm, was associated with resolution of chronic abdominal pain post-appendectomy. Histological investigations on apparently normal appendices of patients who underwent appendectomy for presumed acute appendicitis led to the concept of neurogenic appendicopathy. Mucous, axial, or submucosal neuromas were found in these patients, suggesting a possible cause of RLQ pain.18,19 In our patient series, no specimen satisfied the histopathological criteria for neurogenic appendicopathy by hematoxylin and eosin staining.
In the current study, we did not find evidence of pain recurrence after appendectomy. Even in the subgroup of patients with normal pathology of the appendix (8 of the 30 patients), long-term resolution of pain was excellent, with an average Likert score of 4.8 during follow-up at 12–63 months postoperatively.
Laparoscopy has evolved into a valuable diagnostic and therapeutic tool for abdominal pathologies. Laparoscopic appendectomy is a quick and safe procedure with low morbidity and a short postoperative hospitalization. In carefully selected patients suffering from chronic and focal RLQ pain without evidence of alarm symptoms such as weight loss, bleeding, persistent fevers, diarrhea, or significant vomiting, elective appendectomy is likely to yield long-term resolution of symptoms. We advocate for early consideration of laparoscopic appendectomy for patients with unremarkable workup suffering from chronic RLQ abdominal pain of unclear etiology.
In conclusion, we found that lymphoid hyperplasia in the appendix is a frequent finding in excised appendixes. Lymphoid/follicular hyperplasia of the appendix defined by ≥9 GCs/5 mm was significantly more common in pediatric patients with CAP. Our data suggest that the histopathological finding of lymphoid/follicular hyperplasia of the excised appendix is a predictor for resolution of chronic abdominal pain post-appendectomy.
Pediatric gastroenterologists and gastroenterological pathologists should be aware that this unique clinicopathologic correlation exists when reviewing the post-surgical appendiceal pathology of children with chronic abdominal pain.
This study is limited by its retrospective nature; the lack of a validated abdominal pain protocol and a limited number of random age-matched controls of patients who underwent removal of their appendix in the same time frame for diagnoses other than chronic abdominal pain and without underlying inflammatory or infectious disorder.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.