
Abstract
Background:
Minimally invasive and endoscopic surgical techniques have surpassed the conventional open thyroidectomy for the treatment of thyroid nodules. Trans-axillary, Unilateral Axillo-Breast Approach (UABA), Bilateral Axillo-Breast Approach, and Trans-Oral Endoscopic Thyroidectomy Vestibular Approach (TOETVA) are the most common endoscopic procedures performed currently. This article highlights our experiences with UABA and TOETVA over a period of 6 years.
Materials and Methods:
Between January 2015 and December 2020, we retrospectively analyzed our experience in Endoscopic thyroidectomy with 119 patients using UABA (n = 72) and TOETVA (n = 47) in our tertiary care teaching hospital. Both approaches used the standard three-port technique. Real time angiography was performed intraoperatively using Indocyanine Green dye to delineate the vessels in all patients.
Results:
The mean operative time for UABA and TOETVA was 90 and 110 minutes, respectively. Estimated blood loss was 18 mL in the former and 20 mL in the latter. Temporary Recurrent Laryngeal Nerve palsy and Hypoparathyroidism were minimal with TOETVA (5 patients versus 4 patients and 7 patients versus 2 patients). Shorter duration of hospital stay was observed with UABA (3 days versus 5 days). Cosmetic satisfaction was better with TOETVA.
Conclusion:
Based on our 6-year experience, we propose “JJ Hospital Criteria,” which we currently follow to decide which surgical approach will yield best results. UABA and TOETVA are safe, feasible, and give exceptional cosmetic satisfaction. Both approaches should be seen as complementary rather than competitive.
Introduction
Ever since Emil Theodor Kocher performed thyroidectomy in 1906, it has become the standard treatment for thyroid disorders. Endoscopic technique for the parathyroids and thyroid, pioneered by Gagner 1 and Hüscher et al., 2 was the next major breakthrough in neck surgery. Recently various endoscopic and robotic techniques have drawn attention as they use the concepts of Minimally Invasive Surgery and Natural Orifice Transluminal Endoscopic Surgery (NOTES). Among these, endoscopic thyroidectomies are preferred as they are less expensive, utilize simple laparoscopic instruments, and give supreme results without altering the treatment efficacy. 3
Since the last two decades, Trans-axillary (TA), Bilateral Axillo-Breast Approach (BABA), Unilateral Axillo-Breast Approach (UABA), and Trans-Oral Endoscopic Thyroidectomy Vestibular Approach (TOETVA) approaches have been the most frequently performed procedures for benign nodules. Axillo-Breast approach pushes the external scars away from the neck, and TOETVA is based on the principles of NOTES. 4 Both require a high learning curve and skillful instrument handling. Nonetheless, they deliver paramount cosmetic satisfaction, minimal postoperative complications, less postoperative pain, shorter hospital stay, and quicker recovery. We present our 6-year experience in the management of thyroid nodules using UABA and TOETVA approaches.
Materials and Methods
We performed a retrospective study after obtaining approval from the Institutional Review Board on endoscopic thyroidectomy at our Grant Government Medical College and Sir JJ Group of Hospitals, a tertiary care teaching hospital in Mumbai, with 119 patients total between January 2015 and December 2020. Seventy-two patients were operated with UABA, and 47 patients underwent TOETVA. All patients had preoperative diagnosis of benign thyroid diseases with euthyroid state, based on clinical and Ultrasound (US) examination, confirmed by Thyroid Function Tests and Fine Needle Aspiration Cytology. The surgical approach was based on Surgeons' choice.
Patient selection criteria
Inclusion criteria:
Benign thyroid disease in Euthyroid state Thyroid nodules of size 6 cm or less Patient consenting for the study
Exclusion criteria:
Thyroid nodules of size more than 6 cm
Retrosternal goiter
Pregnancy
Previous neck surgery/Irradiation
Compromised Oral Hygiene/Infection
Unable to tolerate general anesthesia
Not consenting for the study
Preoperative preparation
Patients planned for Trans-oral vestibular approach had undergone routine oral cavity examination to exclude any source of infection, and they were advised chlorhexidine gluconate gargles thrice a day for 3 days to reduce risk of infection, preoperatively. All participants underwent flexible fiber-optic laryngoscopy before surgery to look for any pre-existing vocal cord dysfunction.
Operative methods
Unilateral Axillo-Breast Approach
General anesthesia is performed by endotracheal intubation. Patients are placed in supine position with slight neck extension by placing a bolster between the shoulder blades and ipsilateral arm abducted (Fig. 1). The surgeon and the assistant stand on the ipsilateral side. A 10/12 mm port is placed at the intersection of the mammary borderline and anterior axillary line. A blunt dissector is used to create tunnel from the axillae toward clavicle and sternoclavicular head for working ports and camera port. Two 5 mm ports are placed over the upper edge of ipsilateral areola and the anterior axillary line. A pressure of 6–8 mm Hg is achieved with continuous Carbon dioxide (CO2) insufflation.
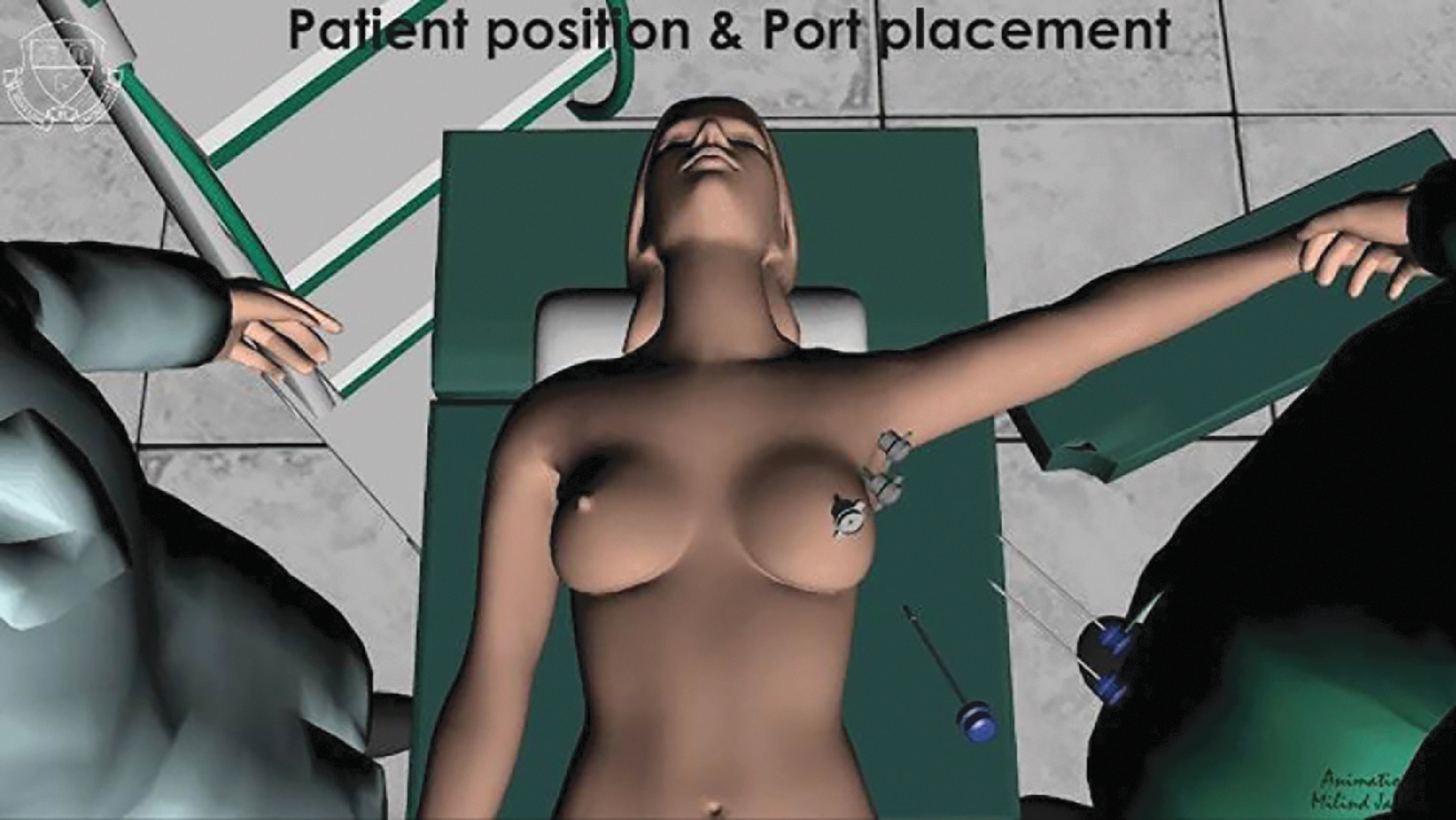
Patient position and ports placement in UABA. UABA, unilateral axillo-breast approach.
Flap dissection is commenced with ultrasonic shears and monopolar diathermy until midline, clavicle, and sternoclavicular joint. Strap muscles are opened and dissection proceeded over the nodule. Real time angiography with Indocyanine Green (ICG) dye fluoroscopy (Fig. 2) facilitated to distinguish inferior pedicle which is dissected and divided. After dividing the isthmus in midline, middle thyroid vein and superior pedicle are identified and divided. Parathyroids along with recurrent laryngeal nerve (RLN) are preserved (Fig. 3). The resected specimen is extracted in an endo-bag (Fig. 4).
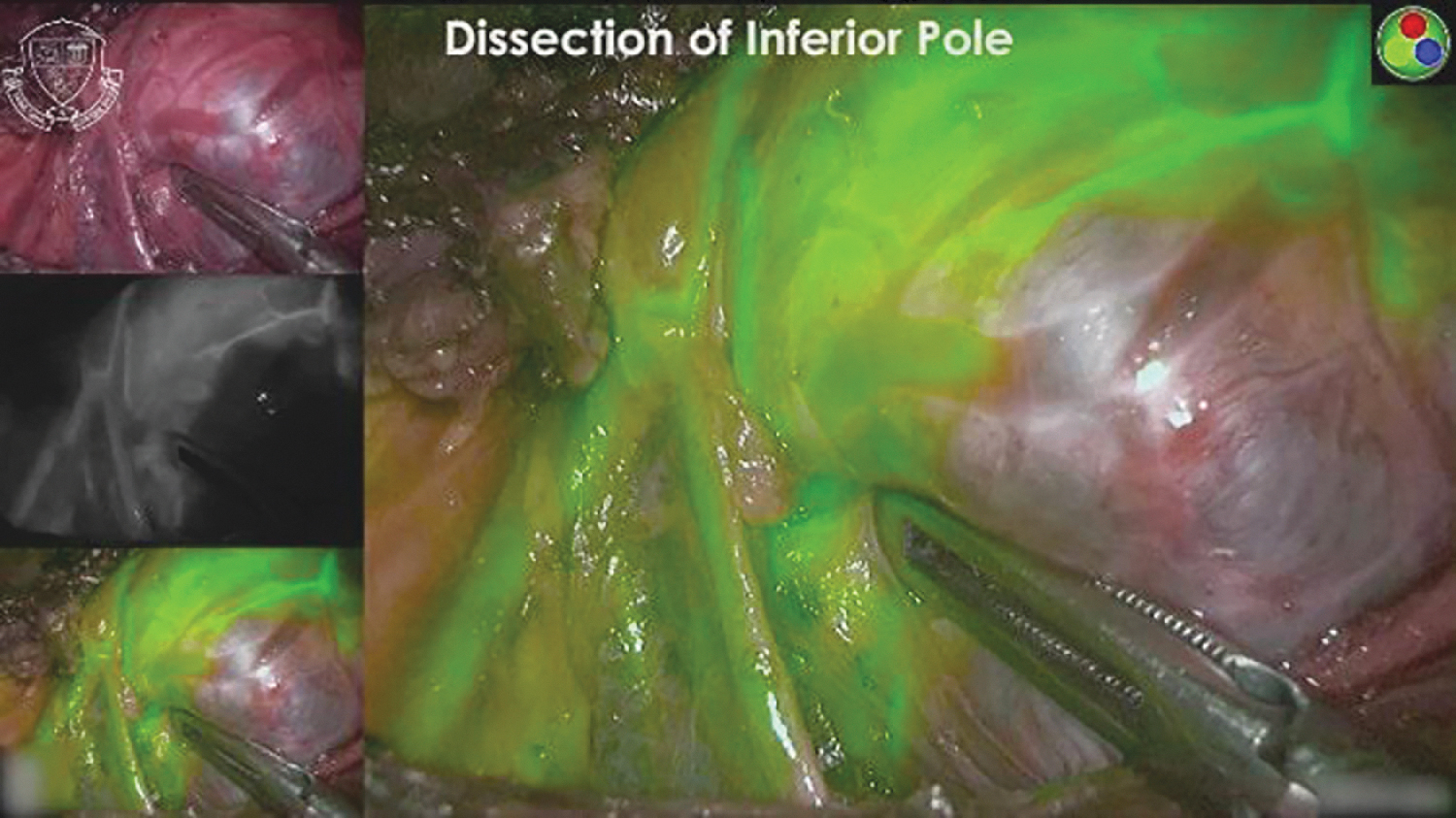
Real time Angiography using ICG dye. ICG, Indocyanine Green.
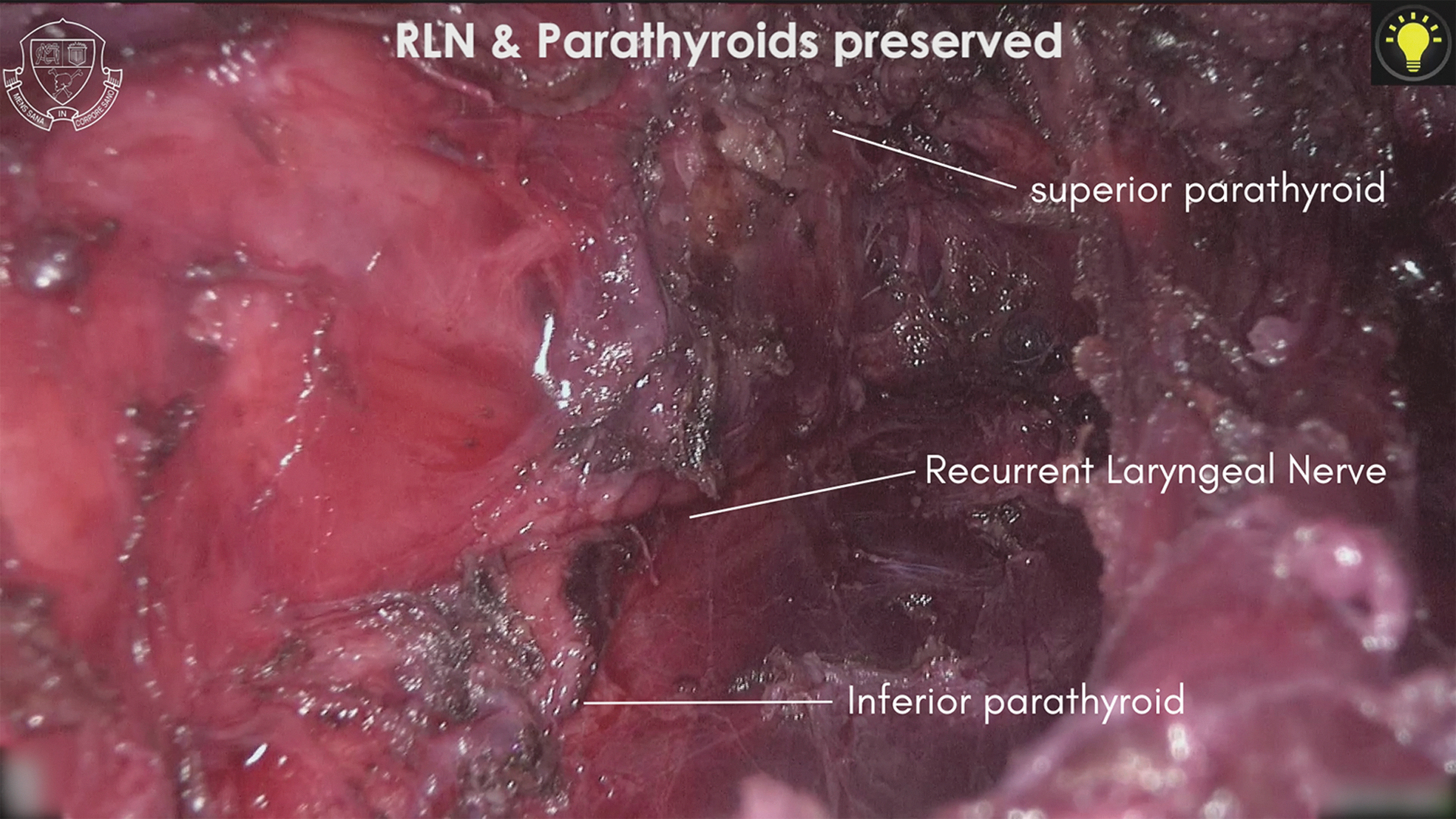
Shows preserved RLN along with parathyroids. RLN, recurrent laryngeal nerve.

Illustrates retrieval of specimen using endo-bag.
Transoral endoscopic vestibular approach
Patients are administered general anesthesia using endo-nasal intubation and placed in supine position with slight neck extension and both arms by the side. The surgeon and the assistant stand at the head end of patient. Oral cavity vestibule is disinfected with diluted povidone iodine solution. A 10 mm horizontal incision is made in the midline and two 5 mm vertical incisions, 1.5–2 cm lateral and above to it (Fig. 5). Hydro-dissection is done using 50 mL of 1:200,000 adrenaline saline solution. Blunt dissection is done till sternum and three ports are inserted through the incisions (Fig. 6). CO2 insufflation is started with pressure of 6–8 mmHg and flow rate of 3 L/minute. Dissection is proceeded in the midline using monopolar hook and ultrasonic shears. Strap muscles are divided and hitched with sutures for better visualization. Isthmus, Superior pedicle, middle thyroid vein, and inferior thyroid pedicle are divided in that order with the help of real time angiography using ICG. RLN and parathyroids are protected. Specimen is retrieved using an endo-bag. Strap muscles are approximated using barbed polydioxanone. Vestibular incisions are closed using poliglecaprone 3’0 sutures. The same steps are repeated on the contralateral side in cases of total thyroidectomy.
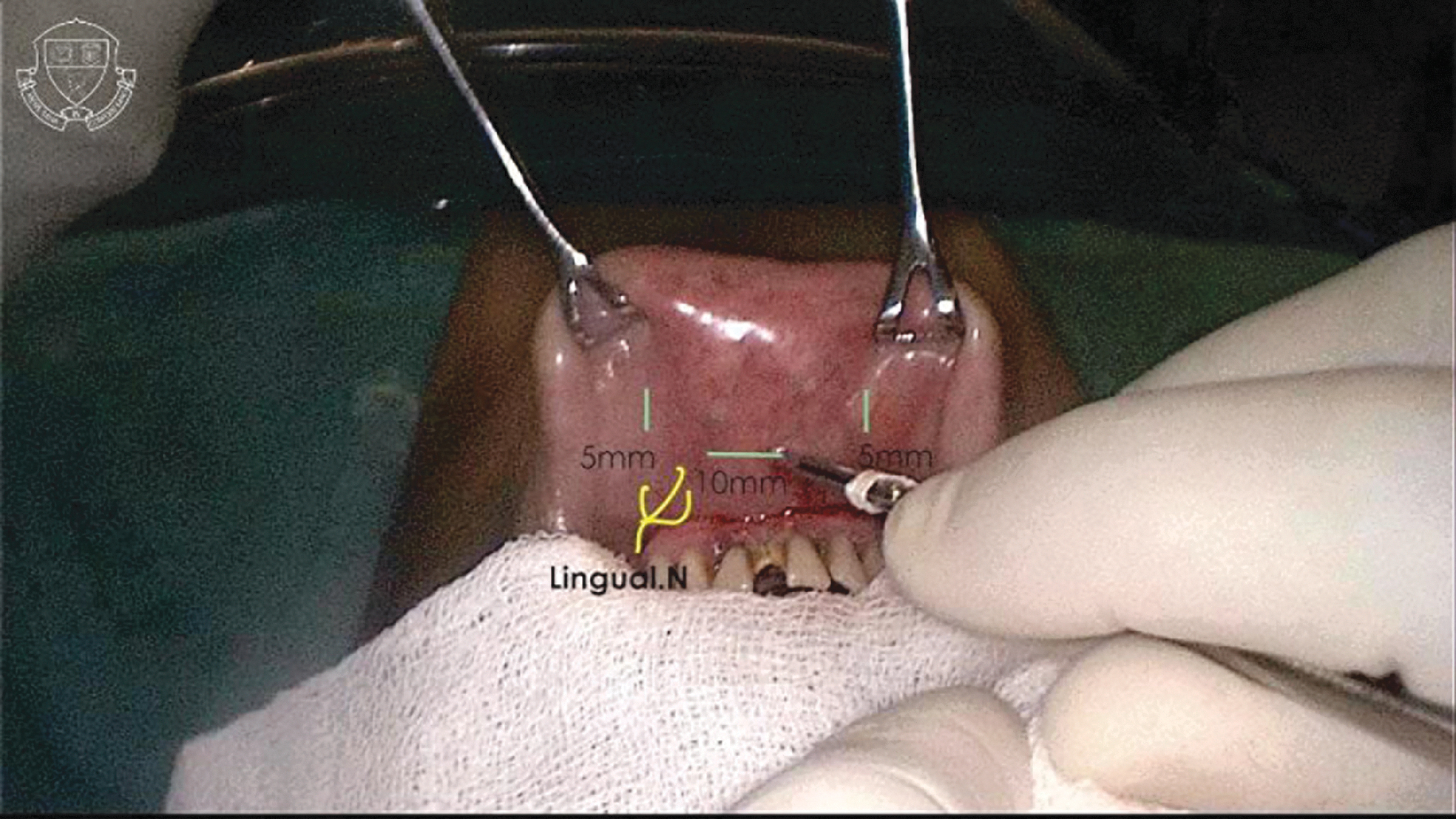
Surface marking of port-site incisions in TOETVA. TOETVA, trans-oral endoscopic thyroidectomy vestibular approach.

Creation of surgical tunnel in TOETVA using blunt dissection. TOETVA, trans-oral endoscopic thyroidectomy vestibular approach.
We used a questionnaire to assess the subjective cosmetic satisfaction (after 3 months) and Vancouver scar scale (after 10–12 months) to assess the scar (Table 1). Cosmetic satisfaction score was calculated by adding the score of the questions about the neck scar and contour of the neck using a verbal response scale ranging from 1 to 5 (corresponding to decreasing satisfaction). 5
Cosmetic Satisfaction Score Questionnaire
TOETVA, trans-oral endoscopic thyroidectomy vestibular approach; UABA, unilateral axillo-breast approach.
Statistical analysis
The means were compared using t-test or Mann–Whitney U test when appropriate. The proportions were compared by Fisher's exact test or Chi-square test when appropriate. All tests were two-tailed, and when P ≤ .05, differences were deemed statistically significant. Data were analyzed using IBM-SPSS statistics application, version 25.
Results
A total of 119 patients (Male: 17, Female:102) were enrolled in the study, with 72 receiving UABA and 47 receiving TOETVA. Among them, females were the predominant participants in both groups (UABA—83.3%, TOETVA—89.4%). Mean age was 34.2 years in UABA and 35.8 years in TOETVA. Mean Body Mass Index was 22 and 20 in UABA and TOETVA, respectively. Average size of thyroid nodule in each group was 4.7 and 2.5 cm, respectively. In TOETVA group, 8 patients (25.5%) underwent Lobectomy and 39 patients (74.5%) underwent Total thyroidectomy, whereas all 72 patients in UABA group underwent Lobectomy (Table 2).
Patients' Characteristics
BMI, body mass index; SD, standard deviation; TOETVA, trans-oral endoscopic thyroidectomy vestibular approach; UABA, unilateral axillo-breast approach.
The duration of surgery was longer in TOETVA compared to UABA (110 ± 20 minutes versus 90 ± 15 minutes). Mean estimated blood loss was minimal with both the approaches (UABA = 18 mL; TOETVA = 20 mL). Mean duration of postoperative hospital stay was 3 days for UABA and 5 days for TOETVA. In contrast to the western countries, the longer follow-up duration is owing to the fact that we are a Pan-India referral center in addition to being a government tertiary care teaching institute. Patients were not discharged in the immediate postoperative period because they were referred from different parts of the country, and frequent follow-up in the postoperative period is inconvenient. Therefore, patients are discharged only when deemed fit and there is less likelihood of immediate complications. Cosmetic satisfaction score was low with TOETVA, that is, 3.12 and 3.47 with UABA after 3 months of discharge.
Complications were divided into minor and major complications. Temporary RLN palsy, temporary hypoparathyroidism, seroma formation, skin infection, difficulty in swallowing, difficulty in chewing, paresthesia in the chest wall, and paresthesia of lower lip due to mental nerve injury are included in minor complications. Major complications include conversion to open permanent RLN palsy, permanent hypoparathyroidism, hematoma formation, skin burns, and other complications which require extended hospital stay.
All patients were assessed with clinical voice assessment and Direct Laryngoscopy on postoperative day 1 and subsequently at 2 weeks. Temporary RLN palsy (Neuropraxia) was recorded in 4 and 5 cases with TOETVA and UABA, respectively. All these patients were managed by speech-language pathologist with multiple sessions of voice therapy. Nonetheless, all patients recovered within 4 weeks, which was confirmed by Direct Laryngoscopy examination. Temporary hypoparathyroidism was defined as recovery within 6 months of surgery. 6 Temporary hypoparathyroidism was seen with 7 patients who had undergone UABA, and only 2 patients among those who underwent TOETVA suffered from it. They also recovered within 6–8 weeks (Table 3).
Surgical Outcomes
RLN, recurrent laryngeal nerve; SD, standard deviation; TOETVA, trans-oral endoscopic thyroidectomy vestibular approach; UABA, unilateral axillo-breast approach.
Three patients (UABA—2; TOETVA—1) had postoperative diagnosis of Papillary Thyroid Carcinoma (PTC) and 1 patient (UABA—1; TOETVA—0) had Follicular Thyroid Carcinoma. Completion thyroidectomy with central lymph node dissection was done using TOETVA in patients who underwent UABA and using UABA in patients who underwent TOETVA. Completion thyroidectomy was done between 2 and 3 weeks after the primary surgery. After 1 year of follow-up, both these approaches yielded analogous outcomes and improved patient satisfaction (Figs. 7 and 8).

Postoperative scar picture of UABA. UABA, unilateral axillo-breast approach.

Postoperative scar picture of TOETVA. TOETVA, trans-oral endoscopic thyroidectomy vestibular approach.
Discussion
Five percent of the entire world population has palpable thyroid nodules, and the incidental detection increases up to 70% with the advent of better US imaging techniques. Although most of them are benign nodules, the importance lies in ruling out malignancy. Besides US, Cytology and Radionuclide imaging techniques facilitate the diagnosis of exact pathology. 7 Most of the benign thyroid nodules are asymptomatic and have a mild course. It is more common in young females. Largely, cosmesis is the most important factor for which such patients seek medical care.
Paolo Miccoli first described the famous Minimal Invasive Video-Assisted Thyroidectomy in 1999 to achieve less postoperative pain and better cosmetic results than the standard open thyroidectomy. 8 In 2000, an alternative technique to avoid an operative scar in the neck was developed by M Ohgami. He utilized subcutaneous space in the breast and the subplatysmal space in the neck for dissection by placing small 15 mm incision between the nipples. The Breast Approach (BA) was feasible with low pressure subcutaneous CO2 insufflation and exploited ultrasonic energy to remove the thyroid lobe endoscopically. 9 Afterward, Y. Ikeda accomplished endoscopic thyroidectomy using three ports through TA approach in the year 2001. 10 Kenzo Shimazu combined both the approaches and introduced Axillo-Bilateral-Breast approach. 11 Later, Jun-Ho Choe modified it and proposed BABA by adding another port in the contralateral axilla as well. This improved the visualization and helped to perform total thyroidectomy successfully. 12
Owing to the extensive dissection involved with these endoscopic procedures, they are not considered minimally invasive procedures. Even though they provide better cosmetic results, the extensive dissection and the external scars still bothered patients and surgeons as well. NOTES offers solution for all the queries, avoids extensive dissection, and leaves no external scar. Since Wilhelm (2011) performed a combined endoscopic trans-oral and minimally invasive thyroidectomy (eMIT), the paradigm shifted toward trans-oral endoscopic approach. He placed three ports in the sublingual and bilateral vestibular region. 13
In 2014, Cunchuan Wang introduced Endoscopic Thyroidectomy using the oral vestibular approach (ETOVA) where he placed three ports in the gingivobuccal sulcus. 14 Shulutko et el. studied that each individual face shape has its own distinct mandibular shape which may influence the surgical tunnel formation. Euryprosopic faces have short wide basal arches and are feasible for Trans-oral vestibular approach (Fig. 6). A Leptoprosopic face has a long and narrow mandible arch, and a Mesoprosopic face has the intermediate features of the above two (Fig. 9). 15

Model to access thyroid gland in TOETVA. a, width of the operating plane; h, height of the mandible; s, accessibility zone; TOETVA, trans-oral endoscopic thyroidectomy vestibular approach.
Yang et al. conducted first randomized study between ETOVA and Endoscopic Thyroidectomy using the areolar approach (ETAA) with 82 patients. Similarly, our study results exhibited better esthetic results with ETOVA. 16 Angkoon Anuwong adopted TOETVA in 2015 which showed promising results with excellent cosmetic outcome. 17 Since then, there has been flourishing evidence that TOETVA is both safe and successful.18–21 Jitpratoom compared open thyroidectomy with TOETVA in 97 patients diagnosed with Graves' disease which proved that TOETVA is equally effective and a viable alternative approach. 22 TOETVA is an authentic cutaneous scar-free surgical option. The median approach gives bird's eye view to access both lobes of thyroid, as well as central neck compartment. Both endoscopic and robotic procedures have been pronounced in TOETVA. Mental nerve injury, CO2 leak, collision of instruments, and conversion of clean wound (class I) into clean-contaminated wound (class II) are few limitations. 23 Some TOETVA patients experienced subcutaneous emphysema and a long-term worrisome dragging sensation along the surgical route. 24
Guo et al. reported a comparative retrospective analysis between 40 cases of TOETVA with 40 cases of Areola-Breast approach. Apart from cosmetic satisfaction (TOETVA—100%), there were no significant differences observed between two groups. 25 Similarly, comparable cosmetic satisfaction scores were observed with the TOETVA group in our study, as well as less postoperative pain and a shorter hospital stay with the UABA group. Sun conducted a retrospective study to compare TOETVA, Endoscopic thyroidectomy using areolar approach, and conventional open thyroidectomy (COT) for the treatment of PTC with central lymph node dissection which yielded similar results. 24
Kim et al. compared 47 cases using Trans-oral approach (TORT) with 43 cases using Bilateral Axillo-Breast approaches in robotic thyroidectomy. Akin to our results, they concluded that TORT had lesser postoperative pain and a greater cosmetic satisfaction than BABA. No significant differences were observed in postoperative surgical results. 26 Likewise, Chae et al. compared 14 cases of TORT with 56 cases of BABART for PTC. TORT had longer operative time and less visual analogue scale pain score than BABART. 27 These findings were consistent with our study.
It was believed that in case of malignancy for completion thyroidectomy, repeat surgery should be deferred for at least 6 weeks to reduce the postoperative complications and an enhanced tissue healing. 31 But Razavi et al. published a successful completion thyroidectomy using TOETVA as early as 9 days after the initial procedure and outmoded the former concept. 32 Similarly, we were able to perform the completion thyroidectomy within 3 weeks by utilizing the other approach.
We performed endoscopic thyroidectomies using UABA and TOETVA in a total of 119 patients. The 6-year experience imparted us to combine the utilization of both methods according to patient profile. Ultrasonic energy device should be preferred to minimize the skin burn; the usage of spiral ribbed trocars should be encouraged to minimize the leak. Superior pole dissection was simpler with TOETVA, and inferior pole dissection was easier with UABA. For total thyroidectomy, TOETVA was appropriate due to its median approach. If the patient has short and wide mandible, surgical tunnel creation was facile with TOETVA approach. For completion thyroidectomy if the patient had undergone any of the approaches, there is no need to wait another 6 weeks, and the alternative approach should be adopted. This will not only reduce the postoperative complications but also prevent the unnecessary delay in the management.
Several criteria have been proposed for patient selection in endoscopic thyroidectomy. As technology evolves every day, there exist no single gold standard criteria for selecting patients for different types of endoscopic thyroidectomy. There is heterogeneity in inclusion and exclusion criteria used in numerous studies (Table 4). The novel criteria which we use in our JJ Hospital are distinctive in that they help surgeons to decide between TOETVA and UABA. Furthermore, the jaw type and previous type of surgery are taken into account in addition to thyroid size, location, and laterality making our “JJ Hospital criteria” unique. We recommend the new “JJ Hospital Criteria” to choose patients wisely between UABA and TOETVA based on our 6-year experience with endoscopic thyroid and parathyroid surgery (Table 5). 33
Literature Review
ETAA, Endoscopic Thyroidectomy using the areolar approach; RLN, recurrent laryngeal nerve; TOETVA, trans-oral endoscopic thyroidectomy vestibular approach; UABA, unilateral axillo-breast approach.
JJ Hospital Criteria
TOETVA, trans-oral endoscopic thyroidectomy vestibular approach.
Conclusion
Based on our experience, both UABA and TOETVA are safe and feasible in the management of thyroid nodules. Accordingly, the new “JJ Hospital Criteria” can be used preferably in different clinical situations. Each approach has its own set of benefits and drawbacks. Hence, the strategy chosen should be personalized, and the patient preferences should be factored into the treatment plan.
Footnotes
Acknowledgment
The authors acknowledge Prof. Bharat Shah and his entire anesthesia team of Grant Government Medical College and Sir JJ Group of Hospitals for their diligence.
Authors' Contributions
A.B.—conceptualization (lead) and review, A.W.—conceptualization (supporting), A.T.—review and editing (equal), G.B.—writing original draft (lead), formal analysis (lead), review and editing (equal), Methodology (lead), S.B.—original draft (supporting), S.J.—review and editing (equal), S.G.—formal analysis (supporting) and review, C.P.—formal analysis (supporting) and editing.
Ethical Standards
An institutional ethics committee approval was obtained for this retrospective analysis of data. All procedures being performed as a part of the study were a part of routine care. This research work is compliant with STROBE guidelines for observational studies.
Informed Consent for Participation and Publication
Before surgical intervention, all participating patients have consented to undergo the procedural interventions described, as well as the collection of their data and its subsequent analysis and publication.
Data Availability
The data are being maintained in a local database, and details are available at request from the corresponding author with masked identifying details.
Disclosure Statement
A.B., A.W., A.T., G.B., S.B., S.J., S.G., and C.P. have no conflict of interest or financial ties to disclose. A.T. has presented our early experience in endoscopy thyroidectomy at the SAGES 2019 annual meeting in Baltimore, USA.
Funding Information
No funding was received for this article.