
Abstract
Introduction:
Gas embolism can occur during minimally invasive surgical procedures. Its incidence and implications in infants and children are not clear. The objective of this study is to identify gas embolism with transthoracic echocardiography and its consequences in pediatric laparoscopic appendectomy.
Materials and Methods:
This is a descriptive observational study including children undergoing laparoscopic appendectomy. We performed transthoracic echocardiography during surgery and collected data on intraoperative hemodynamic and respiratory parameters.
Results:
To date, we have included 10 patients in whom intraoperative transthoracic echocardiography revealed a 50% incidence of gas embolism. All episodes of embolism were grade I or II, and the patients remained asymptomatic. The hemodynamic and respiratory parameters varied slightly during the pneumoperitoneum.
Conclusions:
Episodes of gas embolism in pediatric laparoscopic appendectomy appeared in up to 50% of patients. Although they were subclinical, we should be aware of the risk of serious events and take measures to maximize safety in pediatric minimally invasive surgery.
Introduction
Pediatric minimally invasive surgery (MIS) has been used increasingly in the past decade. Currently, the most frequent surgical procedures in the pediatric population are performed by this approach. 1 The viability and safety of pediatric MIS have been demonstrated even in newborns and young children. 2 However, studies have also reported its disadvantages. 3 We must be especially careful in pediatric MIS considering the physiological characteristics of pediatric patients and the cardiovascular and respiratory changes that occur in them during thoracoscopy or laparoscopy. Their physiology differs considerably from that of adult patients, and we must take specific measures to avoid any complication related to the minimally invasive approach.4,5
Insufflation with carbon dioxide (CO2), even in minimal amounts, is essential to have sufficient operative space in almost all thoracoscopic and laparoscopic procedures. This gas was chosen among others for its safety profile: it is not flammable, it has high solubility, and it is rapidly metabolized. 6 The entire surgical team, surgeons, and anesthesiologists need a deep understanding and knowledge of its dynamics to adjust anesthetic and surgical techniques to minimize the risks derived from its use.
Gas embolism occurs during laparoscopic and hysteroscopic procedures, with publications dating from the 1980s. 7 Most CO2 emboli are subclinical and they are detected only by imaging studies. Small amounts of CO2 bubbles in the venous bloodstream are rapidly cleared and go unnoticed. 8 However, severe events have been reported in certain cases of massive embolism. 9 In the specific case of pediatric surgery, case reports have described suspected or confirmed gas embolism, in both neonates and older patients, causing serious life-threatening events.10–16
Gas embolism has been studied in different animal models,17,18 and abundant literature is available on many MIS procedures in adult patients.19,20 However, in terms of pediatric MIS, no specific studies are available, only reports of the isolated cases mentioned.10–16 Our hypothesis is that gas embolism happens in a number of patients during pediatric MIS and that we could detected it using echocardiography.
The objective of this trial is to evaluate the incidence, extent, and consequences of gas embolism during laparoscopic appendectomy in children by monitoring with transthoracic echocardiographic imaging and cardiorespiratory parameters.
Materials and Methods
Type of study and population included
We designed an observational descriptive study in which we included children undergoing laparoscopic appendectomy in our institution between 2021 and 2022.
We included all patients undergoing laparoscopic appendectomy from 1 to 15 years of age, regardless of the type of appendix or clinical course.
Patients whose families did not agree to participate or who were operated on without the availability of pediatric cardiologists at the time of surgery were excluded.
All patients and relatives received information about the course and purpose of the study, and all signed the informed consent form.
Surgical procedure
The patients underwent balanced general anesthesia with orotracheal intubation and volume-controlled ventilation. For maintenance, we used sevoflurane (minimum alveolar concentration 1) and remifentanil 0.06 micrograms/kilogram per minute (mcr/kg per min).
We performed a standard three-port technique for laparoscopic appendectomy. We established a CO2 flow of 2–3 liters per minute (lpm) and adjusted it during surgery if aspiration was needed. We set the maximum pressure of CO2 at 10–12 mercury millimeters (mmHg). We used the open technique for first-trocar placement and purged the CO2 tube for 15 seconds before connecting it. For dissection, we used advanced monopolar or bipolar coagulation depending on each specific case. We ligated the stump with preformed ties and extracted the appendix through a surgical retrieval bag. Antibiotics were used as a standard protocol according to the type of appendix.
Intraoperative monitoring
A standard multifunction monitor is used during pediatric general anesthesia. We collected information on heart rate (HR), blood pressure (BP), pulse oxygen saturation (SpO2), end-expiratory CO2 pressure (P-ETCO2), and temperature (T). All measurements were recorded at five different moments during surgery:
Baseline, at the beginning of anesthesia. At the beginning of insufflation. Five minutes after pneumoperitoneum establishment. During dissection and ligation of the mesoappendix. At the end of the pneumoperitoneum.
Transthoracic echocardiography was performed during the same five times. We used an ultrasound machine device with S/W Vivid T8 (GE) function and an S3 probe in the four-chamber apical view. The pressure of the pulmonary artery (Ppa) was calculated by the peak pressure obtained from the measurement performed in the atrial face of the tricuspid valve by adding the value of the central venous pressure. The presence of gas embolism was noted and scored as previously described by Schmandra et al. (Table 1). 21
Grades of Embolism According to Schmandra Et Al.
Two experienced pediatric cardiologists with special interest in cardiac imaging (S.F.-V., E.S.-H.) conducted all studies.
Statistical analysis
For the statistical analysis, IBM SPSS Statistics version 23.0 (IBM Corporation, Armonk, NY) was used.
For general descriptive statistics, quantitative data are expressed as the median and quartile values of 25% and 75% in variables without a normal distribution. Categorical data are expressed as frequencies with percentages (%).
The study was reviewed and approved by the research ethics committee of our institution on September 30, 2020 under registration number 11/2020.
Results
To date, 10 children have been included in our study. Six patients were boys (60%) and 4 were girls (40%). Their ages ranged from 4 to 13 years, with a median of 9 (7.5–10.75). Half of the appendixes were phlegmonous, 20% gangrenous and 30% perforated (Table 2).
General Demographic Data and Type of Appendix
The pneumoperitoneum lasted between 19 and 45 minutes, with a median of 31.5 minutes (25.75–38.75). The CO2 flow ranged between 2 and 4 lpm, with a median of 3.5 lpm (3–3.5). The maximum pressure ranged between 10 and 12 mmHg, with a median of 11 mmHg (10–12).
Slight hemodynamic and respiratory changes occurred in all patients after pneumoperitoneum without evidence of gas embolism in any patient at this time. The changes included slight elevation of P-ETCO2 in 70% of patients, HR in another 7 patients (70%), and systolic BP in 2 (20%) without temperature or SpO2 variation.
During dissection of the appendix and mesoappendix (moment number 4), we detected 5 cases of grades 1 and 2 embolism. This represents an incidence of 50% with a 95% confidence interval (CI) of 12.3% to 87.7%.
SpO2 remained unchanged, and systolic BP, diastolic BP, HR, and P-ETCO2 varying slightly. In patients with embolism, Ppa and P-ETCO2 slightly increased above the values of patients in whom no embolism was detected (Figs. 1–4).
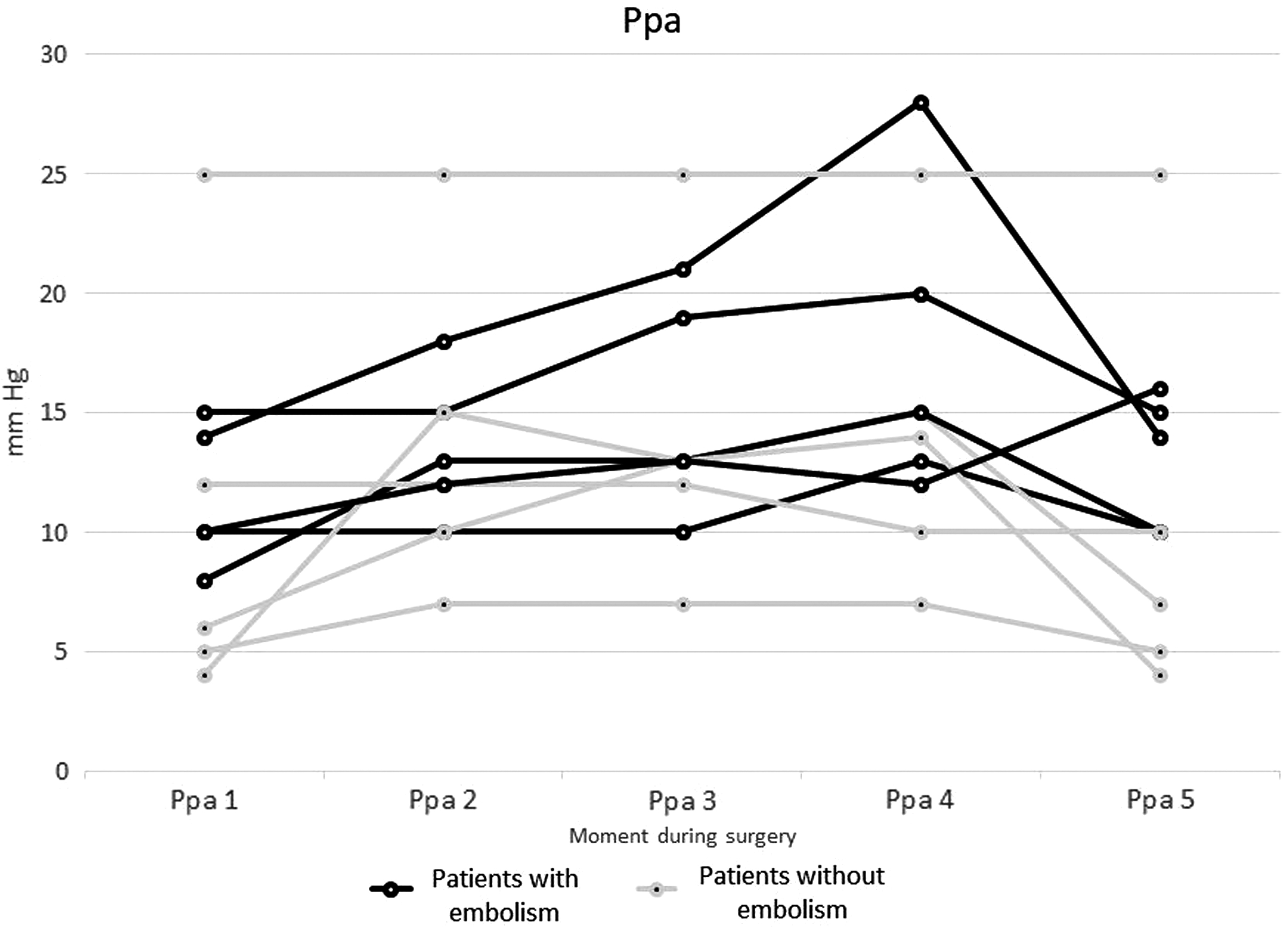
Ppa in the five different moments of surgery. Embolism occurred in moment number 4. (moment 1: baseline; moment 2: insufflation; moment 3: pneumoperitoneum established; moment 4: dissection; moment 5: deflating). Ppa, pressure of the pulmonary artery.

Median Ppa of patients with and without embolism. (moment 1: baseline; moment 2: insufflation; moment 3: pneumoperitoneum established; moment 4: dissection; moment 5: deflating). Ppa, pressure of the pulmonary artery.

P-ETCO2 in the five different moments of surgery. Embolism occurred in point 4. (moment 1: baseline; moment 2: insufflation; moment 3: pneumoperitoneum established; moment 4: dissection; moment 5: deflating). P-ETCO2, end-expiratory CO2 pressure.

Median P-ETCO2 of patients with and without embolism. (moment 1: baseline; moment 2: insufflation; moment 3: pneumoperitoneum established; moment 4: dissection; moment 5: deflating). P-ETCO2, end-expiratory CO2 pressure.
Owing to the small number of patients in our study, we could not perform a reliable statistical analysis to determine the significance of these slight variations.
All patients remained stable during the procedures, no other intra- or postoperative changes or events were observed, and all had an uneventful recovery.
Discussion
We detected gas embolism in 50% (95% CI 12.3–87.7) of the pediatric patients undergoing laparoscopic appendectomy in our series. Our figures follow the same trend as those reported by previous studies in the adult population. Derouin et al. found an incidence of ∼70% in laparoscopic cholecystectomy, 22 and Kim et al. found an incidence of up to 100% during total laparoscopic hysterectomy. 23
CO2 is absorbed by the peritoneum during laparoscopy. The gas diffuses into the capillaries, and as a result, we can detect an increase in P-ETCO2. Optimal ventilatory and surgical management can reduce this absorption and minimize its consequences, especially in neonates and infants.4,5
However, gas embolism is a completely different entity. Gas bubbles enter the bloodstream when there is an open vessel in which the blood pressure is lower than that of the pneumoperitoneum or pneumothorax. Such an opening can be due to injury of a main vessel or direct puncture with a Veress needle but can also occur during the dissection of a profusely vascularized area or by microinjuries when manipulating tissues.17,24
Therefore, we have two different scenarios for gas embolism during MIS: massive embolism and mild subclinical embolism.
Massive embolism is defined as grade 3 or 4, when bubbles fill most of the right chambers of the heart according to the Schmandra classification. Hemodynamic and respiratory compromise is more likely in this type of embolism. Both SpO2 and BP can fall along with P-ETCO2 if the patient goes on acute heart failure. The life-threatening events described in some case reports seem to be related to this type of embolism.9,16 Incidental damage to a blood vessel, such as a persistent umbilical vein, could be the inherent cause.11,12,15 Although it is extremely rare, we must be aware of this possibility, especially in the case of neonatal MIS, where fetal circulation may persist.
Umbilical access does not seem to be a risk factor by itself, but special care must be taken when inserting ports in these patients, avoiding damage to the periumbilical vessels.25,26
Mild subclinical embolism corresponds to grades 1 and 2. It can only be detected by strict monitoring. As the amount of bubbles that enter the bloodstream is minimal, CO2 is rapidly metabolized, and a gas embolism is rarely identified. All the changes that we could detect during mild embolism, such as a rise in P-ETCO2 and Ppa, would be similar to those that occur with pneumoperitoneum7,8 but at a different time during surgery. Instead of happening at insufflation, they will happen when a blood vessel is opened (at insufflation or during dissection).
Transesophageal echocardiography is the best method to detect gas embolism, 27 but as it is an invasive procedure, we opted to monitor our patients with transthoracic echocardiography. Although it is not as sensitive as transesophageal echocardiography, it is specific and noninvasive; therefore, it is more suitable for monitoring children. 28
In our study, we had 6 cases in which the Ppa increased after pneumoperitoneum, but it clearly increased even more after detecting a gas embolism in only 1 case. We also found episodes of P-ETCO2 elevation that occurred during insufflation and were not related to episodes of embolism, although the median P-ETCO2 during dissection in patients with embolism was slightly higher than that in patients without it. PO2 remained stable during surgery in all cases. Future research with a larger cohort of patients could help us to determine the best way to identify mild embolism by means of standard monitoring.
In all of our cases, embolism did not occur during insufflation but during dissection. All cases in whom embolism was detected had particularly inflamed and subserous appendixes or attached omentum that surrounded them, which necessitated careful blunt dissection. Despite the small caliber of the peritoneal vessels opened during these maneuvers, gas embolism occurred. Consequently, we can think that whenever a vessel is opened during laparoscopy, a mild embolism can occur, even in routine pediatric surgery such as appendectomy. Currently, the question is whether this event should be a concern.
There are two main problems with respect to pediatric MIS that increase our patients' vulnerability to a possible serious complication related to an episode of embolism.
First, air embolism, unlike CO2 embolism, is more likely in pediatric patients than in adults. Air bubbles do not decrease in size as quickly as CO2 bubbles. They easily accumulate and can have serious consequences. Animal models show that small amounts of air bubbles can accumulate in the pulmonary vascular system and cause pulmonary hypertension and right heart failure. The lethal dose of air embolism is five times lower than that of CO2 embolism. 18
Ambient air can enter the peritoneal cavity when placing the first trocar during an open technique, especially in neonates. The peritoneal space is small in these patients; with <100 cc of air, we can achieve good laparoscopic vision. The air that enters when we pull the umbilicus to introduce the first trocar already represents a significant percentage of the total amount of intra-abdominal gas once we start CO2 infusion. In addition, unless we purge the insufflator tubes with CO2, all the air that fills the system will also enter the peritoneal cavity. The study by Taylor and Sato measured the proportion of ambient air (nitrogen and oxygen) within a space of 500 cc, similar to the abdominal cavity of a baby, and could reach 40% of the total amount if the system was not purged with CO2 before connecting it to the trocar. 29
In our center, we have a strict protocol according to which we purge the insufflation system with CO2 for 15 seconds at 4 lpm, and we think that all surgeons should follow this protocol to perform a safe laparoscopic surgery. Avoiding air within the peritoneal cavity must be a top priority, especially in neonatal MIS, to prevent any potential complication.
Second, paradoxical embolism should also be a cause of concern in infants and children. It occurs when the right and left circulations are connected, as in atrial or ventricular septal defects. The gas bubbles enter the venous system and they can access the arterial circulation through these anomalous communications. As we have explained previously, gas embolism produces an elevation of the Ppa that favors the shunt from right to left. Once in the systemic circulation, they can end up in any capillary network, including the central nervous system, with potentially devastating consequences.10,12
The transitional circulation present in newborns supposes a greater risk of paradoxical embolism. The patent ductus arteriosus or the foramen ovale are present at birth, and their closure time varies between 1 and 2 weeks. In addition, a 26% incidence of patent ductus arteriosus has been reported in autopsy studies in adults. 30 Therefore, we think that we should perform an echocardiography before a more complex pediatric MIS surgery that involves large vessels or highly irrigated areas such as the liver.
The most important limitation of our study is the small number of patients included. This project is ongoing, and we are including different surgeries to obtain more data. However, in view of the incidence of gas embolism that we have found, we considered presenting our preliminary results to be worthwhile.
Conclusion
Gas embolism occurred in at least 50% of our series of pediatric laparoscopic appendectomies, although it was subclinical. It might not be a concern in routine pediatric MIS procedures but all surgeons should be aware of it and take measures to avoid its potential consequences to maximize safety in minimally invasive pediatric surgery.
Footnotes
Authors' Contributions
S.F. contributed to conceptualization, methodology, investigation, resources, data curation, writing—original draft, and project administration. C.G.-M. was involved in conceptualization, investigation, resources, and data curation. J.M.-M. carried out investigation, resources, writing—review and editing. S.F.-V. was in charge of investigation, resources, and data curation. E.S.-H. took charge of investigation, resources, and data curation. A.J.-M. carried out formal analysis, writing—review and editing, and supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.