
Abstract
Background:
Whole-course intraperitoneal robot-assisted choledochal cyst resection in children under 1 year of age is controversial due to its technical challenges. Current Pfannenstiel incision is widely used in adults for its cosmetic effects but is rarely used in children.
Materials and Methods:
We conducted a prospective, single-center study to assess the feasibility, safety, and cosmesis of whole-course intraperitoneal robot-assisted choledochal cyst resection with Pfannenstiel incision in children under 1 year of age.
Results:
Ten patients were treated with our surgical protocol, and there was no conversion to laparotomy. The average total operation time was 223 minutes. The average duration of anesthesia was 260.2 minutes. The average docking time between the robot arm and Trocar was 17.5 minutes. The average intraoperative blood loss was 16 mL. No postoperative complications occurred in the 10 patients. The mean time to start drinking water after surgery was 2.4 days. The mean postoperative drainage tube removal time was 2.6 days. The average length of stay was 8.5 days. The scar assessment scale total scores of the 2 observers were (6.8 ± 1.23) and (7.4 ± 1.84), respectively. For every patient, there are only four abdominal surgery scars of which 75% of scars were hidden by underpants and 25% of scars were not covered.
Conclusion:
It is feasible and safe to perform whole-courses intraperitoneal robot-assisted choledochal cyst resection with Pfannenstiel incision in children under 1 year old. It also has a hidden incision effect and is worthy of promotion.
Introduction
Choledochal cyst is a group of congenital cystic malformations causing dilation of the biliary tract. The primary clinical manifestations are abdominal pain, gangrene, vomiting, fever, and abdominal mass. Choledochal cyst has a higher rate of prevalence in East Asia, with 1 in 13,000 children reported to be affected. 1 Clinically, this disease is generally divided into five types according to Todani classification, the most common is type I cystic fusiform dilatation of the extrahepatic common bile duct (80%–90%), and type I can be further divided into types IA, IB, and IC.2,3 The disease cannot be cured by itself or through drug treatment, and surgical resection is required. Minimally invasive surgery for choledochal cysts is currently the mainstream method, including laparoscopic-assisted and robot-assisted surgery.
The surgical procedures mainly included choledochal cyst combined with cholecystectomy, intestinal anastomosis, and biliary intestinal anastomosis. 4 Laparoscopic hepatic duct jejunum anastomosis is the most technically demanding and time-consuming part of the operation. 5 In addition, to reduce the difficulty of operation, most laparoscopic-assisted surgeries have to enlarge the surgical incision and drag the intestines outside the abdominal cavity for enteroenteric anastomosis, which not only involves complicated surgical procedures but also increases the risk of postoperative intestinal adhesion. 6 These factors make intraperitoneal suture reconstructive surgery technically demanding and may not be feasible in pediatrics. 7 Robotic surgery has significantly improved operability and accuracy in adult abdominal surgery due to its unique three-dimensional (3D) imaging and flexible design of its simulated manipulator.
For children with choledochal cysts, robotic surgery is expected to try to perform a full intraperitoneal operation, thereby solving the drawbacks of laparoscopic-assisted surgery. However, the limited space in a baby's body can severely hinder the movement of robotic instruments. There is no consensus on which babies should receive robotic intervention. 8 As far as we know, there are few reports on robot-assisted choledochal cyst resection for children under 1 year old. Early case reports have shown the ergonomic advantages of robot-assisted surgery in children around 1 year of age with choledochal cysts, but the Roux ring is shaped outside the body, meaning no intraperitoneal jejunojejunostomy is performed. 9 A retrospective study of robot-assisted intra-abdominal choledochal cyst resection has shown that it is feasible in patients under 1 year of age, but the Roux ring is still extraperitoneally shaped and its port strategy may leave visible abdominal scars. 10 We think the port strategy still could be improved.
Choledochal cyst occurs in female children. With the increase of age, these female patients will become more and more disgusted with the scars left in the abdomen, and even feel inferior. To avoid this psychological harm, for female children, scarless abdominal surgery is worth promoting. After all, they have a long way to go. At present, Pfannenstiel incision is widely used in adults because of its cosmetic effect, but it is still less in children. The name Pfannenstiel is not derived from the shape or position of the incision. It comes from the name of German gynecologist Hermann Johannes Pfannenstiel (1862–1909), who invented this technique. 11 Later, the incision was promoted by Dr. Monroe Kerr, so it is sometimes called the Kerr incision or the Pfannenstiel–Kerr incision. 12 Pfannenstiel incision is an abdominal surgical incision that allows access to the abdomen. It is the most commonly used method for performing caesarean section today. 13 A surgeon cuts a roughly horizontal (slightly curved) line above the pubic symphysis. This incision is usually called a “bikini line incision.”
For aesthetic reasons, the Pfannenstiel incision has become popular over the years. Young women with benign gynecological and pelvic problems are very fond of using this surgical incision. If placed properly, it is usually hidden by pubic hair regeneration. The incision does not distort the navel, the healing speed is faster than the traditional vertical incision, and there is no obvious scar healing. In short, the purpose of this technique is to provide cosmetic incision for pelvic surgery. Later, with the development of minimally invasive abdominal techniques, such as laparoscopy and robot-assisted techniques, these techniques requiring abdominal ports are perfectly combined with the Pfannenstiel incision, which further enhances the aesthetic effect. Existing case reports indicate Pfannenstiel incision is used in robot-assisted urological surgery in children, but it is rarely reported in choledochal cyst resection, especially in children under 1 year of age. 14
To explore whether intra-abdominal robot-assisted choledochal cyst resection can be performed in children under 1 year old while maintaining almost scar-free results, we designed a prospective single-center study in the Affiliated Hospital of Guizhou Medical University. Patients with choledochal cyst under 1 year old were selected as the research objects. Using our surgical plan, that is, robotic working port and camera port are placed on Pfannenstiel incision, to conduct whole-course intraperitoneal robot-assisted choledochal cyst resection, including choledochal cyst excision, jejunojejunostomy, and hepaticojejunostomy. To evaluate the feasibility, safety and cosmetic effects of whole-course intraperitoneal robot-assisted choledochal cyst resection with Pfannenstiel incision in children under 1 year old, the value of this study is to propose the surgical plan and verify its effectiveness, which will help the surgical plan to promote the benefit of more patients with choledochal cysts under 1 year old.
Materials and Methods
Study design
The study was a prospective single-center study in which patients met inclusion and exclusion criteria. The study was conducted at the Affiliated Hospital of Guizhou Medical University in China, one of the country's top Grade-A hospitals. We attempt whole-course intraperitoneal robot-assisted resections of choledochal cyst for children using the da Vinci Robotic Surgical System (Intuitive Surgical, Sunnyvale, CA, USA). All the operations were performed by a senior surgeon. Patients were enrolled between October 2019 and August 2022. The Institutional Review Board approved prospective patient data collection and follow-up.
Inclusion and exclusion criteria
Inclusion criteria: (1) age ≤1 year; (2) preoperative diagnosis was choledochal cyst; (3) can tolerate general anesthesia; (4) preoperative evaluation can tolerate carbon dioxide pneumoperitoneum during robotic surgery; (5) the patient's coagulation function was normal. Exclusion criteria: (1) acute cholangitis; (2) with intrahepatic bile duct dilatation, the corresponding liver needs to be removed to achieve a radical effect; (3) malignant transformation of choledochal cyst; (4) serious organ dysfunction; (5) the family members of the children did not accept the operation.
Baseline data
Demographic data, including gender, age, and body mass index, were collected before surgery. Understand the patient's clinical symptoms, including abdominal pain, distension, palpable mass, jaundice, and laboratory indicators including white blood cells, neutrophil, alanine transferase, aspartic aminotransferase, total bilirubin, direct bilirubin, indirect bilirubin, hemoglobin, and red blood cell.
Hidden incision approach
The patient first received general anesthesia through endotracheal intubation, followed by the placement of a gastric tube for gastrointestinal decompression and a urinary catheter for bladder emptying. The patient's head is elevated 15°, with the body slightly tilted to the left by 15°. Next, disinfect the patient's abdominal area with Povidone iodine disinfectant three times, and sterile sheets were placed. After that, the artificial pneumoperitoneum was established using a pneumoperitoneum needle at the junction of the Pfannenstiel line (1 cm above the symphysis pubis) and the midline transumbilical line to maintain intra-abdominal pressure between 6 and 8 mmHg.
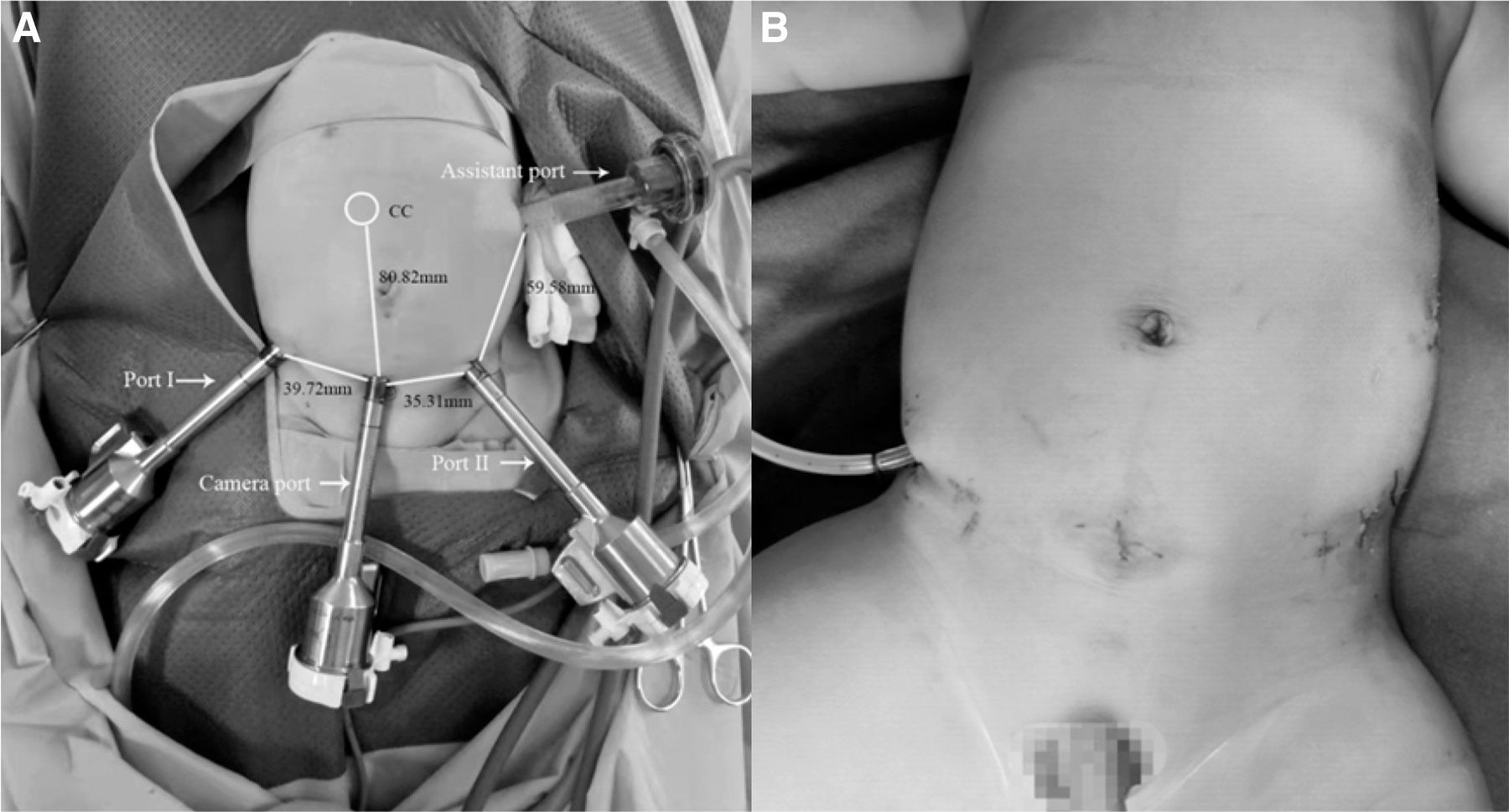
Following that, the four-hole layout strategy was implemented. Briefly, after removing the pneumoperitoneum needle, an 8 mm trocar was inserted at the pneumoperitoneum site to establish the Camera port required for robot-assisted laparoscopic surgery. A 3D endoscopy camera was then introduced for visualization. Under the observation of the camera, another 8 mm trocar was inserted ∼1–2 cm away from the junction between the Pfannenstiel line and the right anterior superior iliac spine to establish Port I. Similarly, another 8 mm trocar was inserted ∼1–2 cm away from the junction between the Pfannenstiel line and the left anterior superior iliac spine to establish Port II. An Assistant Port was created by inserting a 12 mm trocar 1 cm below the left midaxillary line and costal margin (Fig. 1A). Finally, the robotic bedside robotic arm system was guided into the operating area, and each arm was docked with the corresponding trocar.
Port placement and distance in robotic-assisted surgery for choledochal cysts
Operation procedures
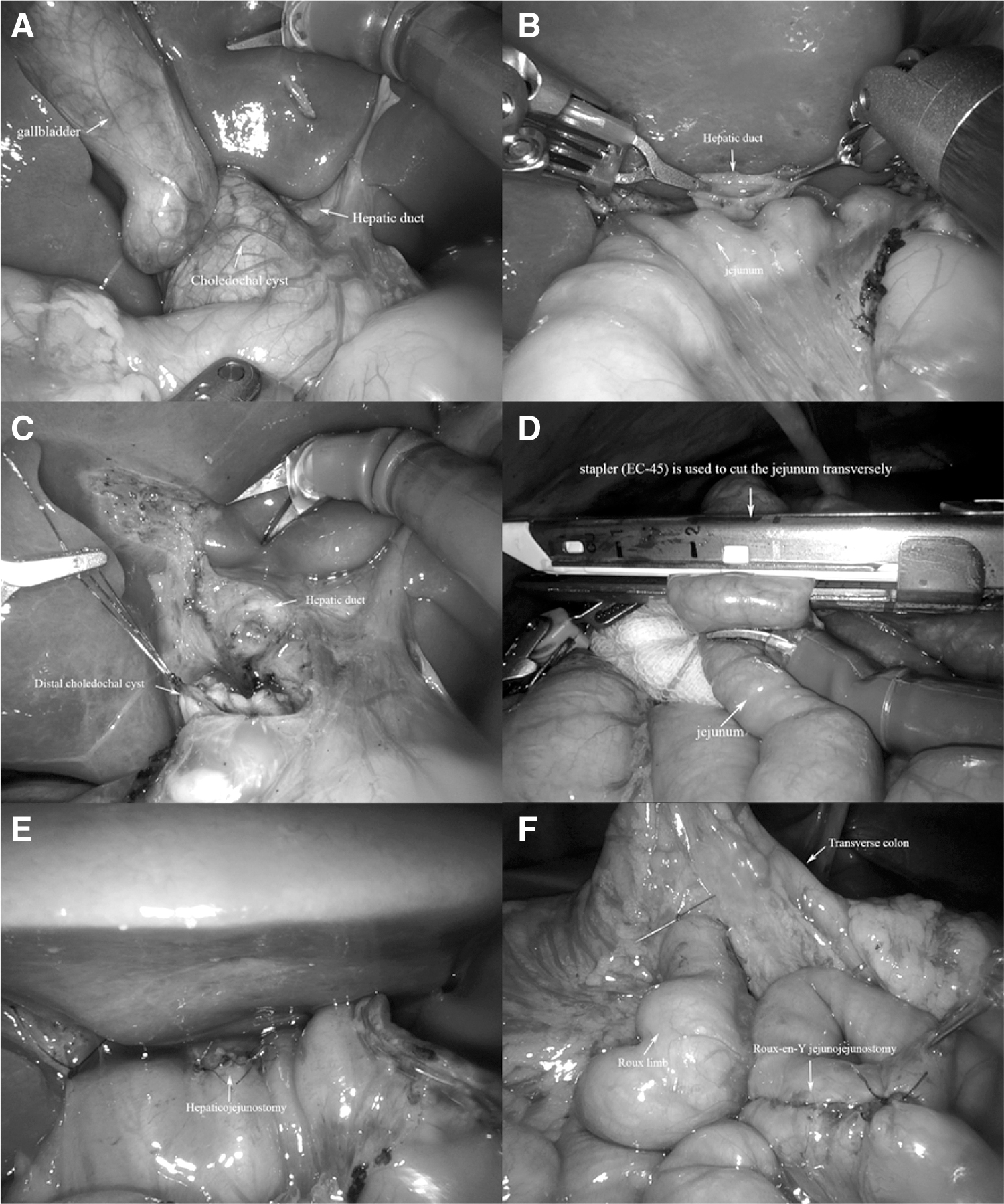
Next, the entire intraperitoneal operation was performed to complete the robot-assisted choledochal cyst resection and Roux-en-Y hepaticojejunostomy. After connecting the robotic arm, the surgeon looked for the choledochal cyst and identified its anatomical relationship with the gallbladder and the hepatic duct (Fig. 2A). Before starting the surgery, if the choledochal cyst was large, a cyst aspiration and decompression procedure should be performed first. Then, the connection between the proximal choledochal cyst and the normal hepatic duct was cut to prepare the hepatic duct for subsequent hepaticojejunostomy (Fig. 2B).
Looking for the location of the choledochal cyst
The connection between the distal choledochal cyst and the normal bile duct was cut, and the cut end of the bile duct was closed using a continuous suture with 4–0 absorbable suture (Fig. 2C). The excised choledochal cyst along with the gallbladder was removed from the Assistant Port. The linear cutting stapler (EC-45) was used at a distance of 15–20 cm from the Treitz ligament to cut the jejunum while simultaneously closing the broken end of the proximal and distal jejunum (Fig. 2D). The distal ileum was brought up to the porta hepatis by passing it through the avascular region of the right mesentery of the transverse colon. The distal jejunum was incised longitudinally by 0.5–1 cm at a distance of 1–2 cm from the closed end. Continuous end-to-side anastomosis between the hepatic duct and the jejunum was performed using a 5–0 absorbable suture (Fig. 2E). The continuous side-to-side anastomosis was performed with the proximal jejunum using a 5–0 absorbable suture at a distance of 35–40 cm from the closed end of the distal jejunum. The diameter of the anastomosis was ∼1–2 cm. The mesenteric defect was then repaired promptly using intermittent sutures with a 5–0 absorbable suture (Fig. 2F).
The anastomotic area was rinsed with normal saline to ensure there was no intestinal torsion, bleeding, or bile leakage during the operation. A drainage tube inserted from Port I to place around the hepatic hilum. The pneumoperitoneum was released, the trocars were removed, and the incisions were subcutaneously sutured. Finally, medical biological glue was used to align and adhere to the skin (Fig. 1B).
Efficacy evaluation
The efficacy of the surgical program in this study was evaluated from three dimensions: feasibility, safety, and cosmesis. Feasibility indexes include the applicability to different types of choledochal cysts, the diameter of the choledochal cyst, whether the entire procedure was completed intraperitoneally, whether conversion to laparotomy was required, the length of the operation, the duration of anesthesia, and the duration of docking between the manipulator and the trocar. Safety indexes include intraoperative blood loss, intraoperative blood transfusion or not, whether there were postoperative complications, the time to start drinking water after surgery, postoperative drainage tube removal time, length of hospital stay, and follow-up results after discharge. Cosmesis indexes include Observer Scar Assessment Scale (OSAS) and pictures comparison of scars before and after surgery. 15
Statistical analysis
Data were collected using Microsoft Office Excel 2007. Classification variables are represented by count (N) and percentage (%). Shapiro–Wilk test was performed using SPSS 26.0 software to determine the type of data distribution. Value variables conforming to normal distribution were represented by Mean (standard deviation), and value variables conforming to skew distribution were represented by Median (interquartile range).
Results
Ten patients under 1 year of age diagnosed with choledochal cyst were treated with our surgical protocol. Baseline data for 10 children are shown in Table 1. Three of the cases were male, and 7 were female. The age was 115 (88.25–271.25) days, and the body mass index was 16.8 ± 1.25 kg/m2. Sixty percent of these patients developed abdominal pain, 40% bloated, 20% palpable abdominal mass, and only 10% jaundice. The average total number of white blood cells in peripheral blood is 9.56 ± 1.25 × 109/L. The mean neutrophil percentage was 25.02 ± 9.88%. The average alanine transaminase was 53.63 ± 31.99 U/L. The average aspartate transaminase was 56.86 (37.02–107.07) U/L. Average total bilirubin is 17.9 (7.65–47.48) μmol/L. Average direct bilirubin is 11.70 (2.80–35.10) μmol/L. Average indirect bilirubin is 5.83 (2.82–16.71) μmol/L. The average hemoglobin was 11.89 ± 0.96 g/dL. The average total number of red blood cells was 4.40 ± 0.38 × 109/L.
Baseline Data
ALT, alanine transferase; AST, aspartic aminotransferase; BMI, body mass index; DBIL, direct bilirubin; F, female; Hb, hemoglobin; IBIL, indirect bilirubin; M, male; N, neutrophil; RBC, red blood cell; TBIL, total bilirubin; WBC, white blood cell.
The evaluation results of feasibility indicators are shown in Table 2. This surgical protocol was applied to Todani I patients, including 7 Todani IA patients, 2 Todani IB patients, and 1 Todani IC patients. The average diameter of choledochal cysts was 5.51 ± 2.83 cm. All the 10 patients underwent abdominal surgery without conversion to laparoscopy or laparotomy. The average total operation time was 223.00 ± 11.60 minutes. The average duration of anesthesia was 260.20 ± 10.51 minutes. The average docking time between the robot arm and trocar was 17.50 ± 1.72 minutes.
Feasibility Indicators
The evaluation results of security indicators are shown in Table 3. The intraoperative blood loss was 10 (5–12.5) mL. None of the 10 patients received blood transfusion. No postoperative complications occurred in the 10 patients. The mean time to start drinking water after surgery was 2 (2–3) days. The postoperative drainage tube removal time was 2 (2–3.25) days. The length of stay was 8.5 ± 2.7 days. All the 10 patients recovered and were discharged from hospital. The mean follow-up time after discharge was 2 years, and all patients recovered well.
Security Indicators
Since children under 1 year of age could not clearly express their evaluation of the cosmetic effect of their own surgical scars, OSAS was used to evaluate surgical scars at 6 months after surgery. OSAS score consists of five items (vascularization, pigmentation, thickness, relief, and pliability), each of which has a score ranging from 1 to 10, with a total score of 50. The smaller the score, the higher the scar satisfaction. OSAS scores were evaluated by 2 senior physicians including the surgeon. The OSAS total scores of the 2 observers were (6.8 ± 1.23) and (7.4 ± 1.84), respectively. The OSAS scores showed good scar satisfaction (Table 4).
Observer Scar Assessment Scale Scores Distribution of Two Observers
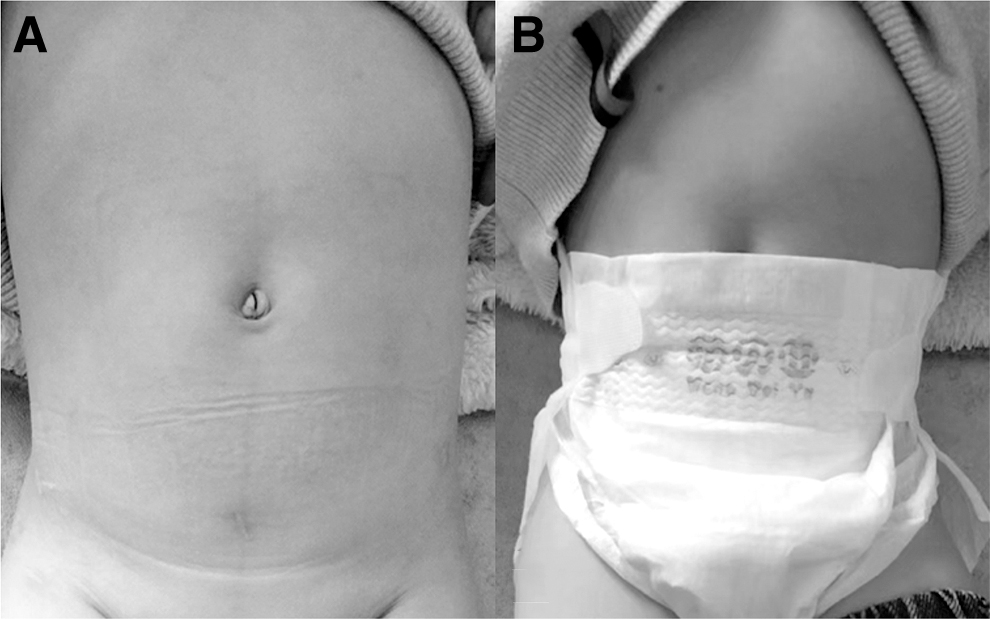
Finally, we followed up the patients and took a comparative set of images of scars before and after surgery. There were only four abdominal surgery scars per patient, 75% (n = 10) of scars were concealed by panties and 25% (n = 10) of surgical scars at Assistant Port position were not covered. The results show that most surgical scars can be covered by underwear, which plays a cosmetic effect of hiding the incision (Figs. 3 and 4).
Pictures comparison of postoperative scars

Pictures comparison of postoperative scars
Discussion
A previous study suggested that total robot-assisted choledochal cyst resection should be performed in patients aged 4 years and above; for patients under 4 years, a Roux-en-Y jejunojejunal anastomosis is recommended to be performed extracorporeally. 16 Our study challenges the previous view that total peritoneal robot-assisted choledochal cyst resection is not feasible in children under 1 year of age. At the same time, drawing on the previous ideas, Pfannenstiel incision was applied to the whole-course intraperitoneal robot-assisted choledochal cyst resection in children under 1 year old. Our results show that Pfannenstiel incision can be used for robot-assisted choledochal cyst resection in children under 1 year of age, which not only has cosmetic effects but also does not affect the whole abdominal operation.
Our surgical protocol emphasizes intraperitoneal Roux-en-Y anastomosis. Although many centers have reported experience in laparoscopic choledochal cyst excision, most reports have used extraperitoneal Roux-en-Y, due to the difficulty of intraperitoneal Roux-en-Y anastomosis. The use of the Da Vinci robotic surgical system provides 3D visualization of the operating field and the advantages of a wrist-type end-effector with reduced tremor, motion scaling, and additional freedom compared to standard laparoscopic instruments. Thus, intraperitoneal Roux-en-Y anastomosis was possible. Existing case reports suggest that Roux-en-Y anastomosis can be created entirely by a robot intraperitoneal or extraperitoneal through a small incision. Although robotic assistance is common in many surgeries, there is very limited information about robot-assisted choledochal cyst excision. We summarized the existing literature on robot-assisted choledochal cyst excision in pediatrics, as shown in Table 5.7,9,10,16–28
The Summary of Children Cases of Robotic-Assisted Choledochal Cyst Excision
The advantage of our surgical protocol is that we used a whole-course intraperitoneal procedure, including in intraperitoneal Roux-en-Y anastomosis. In addition, the number of abdominal scars in our cases was only four. 3D visualization, clear instrumentation, and fine motion filtering are major advantages of robot-assisted surgery, enabling more general surgeons to perform certain complex procedures. Our study shows that whole-course intraperitoneal robot-assisted choledochal cyst resection is feasible in children under 1 year of age. This is thanks to advances in technology.
Before the study, we reviewed relevant literature on robot-assisted choledochal cyst excision. Considering the technical difficulty of whole-course intraperitoneal incision and suture reconstruction, initially we believed that our operation time would be longer than that reported in the literature. At the end of the study, we counted the overall operation time and reviewed 16 robot-assisted choledochal cyst excision studies, including 13 studies of extracorporeal Roux-en-Y anastomosis and 3 studies of intracorporeal Roux-en-Y anastomosis. To our surprise, our approach did not seem to prolong the operative time based on what is reported in the literature. Due to previous conceptual limitations, many surgeons have been reluctant to attempt the entire surgical process of intraperitoneal incision and suture reconstruction with the assistance of robots in children under the age of 1 with choledochal cysts.
In addition, one of the advantages of our surgical protocol is the emphasis on placing the robotic working port and camera port on the Pfannenstiel incision. Pfannenstiel incisions are commonly used in adults due to their cosmetic properties, but they are often overlooked in children. 29 The reason for this is that adults can appreciate the importance of scar cosmesis, whereas children, especially those under 1 year old, cannot express such concerns.
We conducted a comprehensive analysis of the port strategies reported in the current literature for robot-assisted choledochal cyst excision in children and provided corresponding schematic diagrams (Fig. 5). The results revealed a wide variety of port strategies in different countries, suggesting a lack of a unified standard. In comparison to the port strategy reported in the current literature, our approach offers several advantages. First, the incision positions can be covered by underpants, enhancing the cosmetic effect. Second, we only require four incisions that are connected in an arc, which has a good aesthetic effect. Additionally, we utilized the OSAS to assess scar satisfaction and demonstrated positive results in terms of scar satisfaction.

Summary of port strategies for robot-assisted choledochal cyst resection in different studies
However, it is important to note that this study has certain limitations. First, it was an exploratory study with a relatively small sample size. Additionally, it was not a randomized or multicenter study. Furthermore, due to the use of Pfannenstiel incision, we were unable to conduct a comparative study with robot-assisted extraperitoneal Jejunojejunostomy, which requires an additional umbilical incision. Therefore, a surgical control group was not included in this study.
Conclusion
In summary, we report the case series of complete intraperitoneal robot-assisted choledochal cyst resection in children under 1 year of age with Pfannenstiel incision. The results show that Pfannenstiel incision in children under 1 year of age is feasible, safe, and has aesthetic effects. This surgical protocol is worth promoting because it can provide additional options for robot-assisted choledochal cyst excision.
Footnotes
Authors' Contributions
Y.Z., X.Y., and H.G.: conception and design. J.D., H.J., and X.S.: collection and assembly of data. G.C., K.H., and W.Z.: data analysis and interpretation. Y.Z., J.L., and H.G: article writing. All authors contributed to the article and approved the submitted version.
Data Availability
All data used during the study are available from the corresponding author by reasonable request.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Science and Technology Program of Guizhou Province (Grant Nos. ZK-2022-418 and ZK-2023-368), the Guizhou Science and Technology Support Program (Grant No. 2019–2793), the Guizhou Health and Health Commission Science and Technology Fund Project (Grant No. gzwkj2022–133), and the National Natural Science Foundation of Guizhou Medical University Funding (Grant No. 20NSP036).