
Abstract
Introduction:
We aimed to evaluate the efficacy of bipolar cauterization for tract site bleeding during standard percutaneous nephrolithotomy (PCNL).
Methods and Materials:
We defined tract site bleeding as when the visual field across the parenchymal tract starts to bleed while the sheath of a balloon dilator is being withdrawn just before the operation is completed. Among 181 patients, 90 patients showed no significant bleeding, and 91 patients required further procedures to resolve tract site bleeding. In cases of unresolved tract site bleeding, either nephrostomy placement (n = 60) or cauterization (n = 31) was performed. The outcomes of three groups (no procedure group, nephrostomy group and cauterization group) were compared.
Results:
The median decrease in hemoglobin at 2-hour intervals postoperatively was −1.75, −1.0, and −0.2 in the nephrostomy, cauterization, and no procedure groups, respectively (P < .001). There were 25 patients (41.7%) who received transfusions in the nephrostomy group, whereas only 1 patient (3.2%) received a transfusion in the cauterization group (P < .001).
Conclusion:
The bipolar cauterization of bleeding points at the end of PCNL could efficiently decrease tract site bleeding and reduce the need for transfusion.
Clinical Research Information Service (https://cris.nih.go.kr/cris; No. KCT0008303).
Introduction
With respect to percutaneous nephrolithotomy (PCNL), bleeding is one of the most bothersome problems. The transfusion rate has been reported to be 7%–20%, and the prevalence of life-threatening bleeding that requires angioembolization has been estimated to reach 1%. 1 For a long time, PCNL-related bleeding complications have tormented surgeons. Twenty years ago, Jou et al. found that electrocauterization of the puncture site could reduce the need for transfusion. 2 At that time, however, reports of electrocauterization during PCNL did not receive attention. One of the reasons might be owing to not using normal saline as irrigation fluid. Most authors used monopolar electrodes, and therefore, hyponatremia could develop after electrocauterization. In addition, switching the irrigation fluid might be troublesome. At present, endoscopic bipolar cauterization is popular and typically performed in transurethral surgery. It is already known that endoscopic bipolar cauterization avoids the occurrence of transurethral resection syndrome. 3 Therefore, we need to shed new light the use of bipolar cauterization during PCNL.
Although miniaturized PCNL has become an excellent alternative procedure to standard PCNL because of its equal stone-free rate, less significant decrease in hemoglobin, and lower transfusion rate, 4 standard PCNL is still beneficial in that has a short operation time and allows easy stone retrieval, especially in patients with a large stone burden. Therefore, endourologists should not discard standard PCNL in patients with staghorn stone. In this study, we present our experience with bipolar cauterization during PCNL, with focus on PCNL-related bleeding.
Methods and Materials
Ethical approval and public data depository
The Institutional Review Board of St. Vincent's Hospital approved the study protocol (Approval No.: CV22RISI0209, approval date: September 29, 2022). This study was also registered in the Clinical Research Information Service (https://cris.nih.go.kr/cris, no: KCT0008303). This study was performed in accordance with the Declaration of Helsinki. This article does not reference any animal studies performed by any of the authors. Informed consent was obtained from all individual participants in the study.
Study population and design
This was a single-center retrospective study in which any patient who underwent PCNL from August 2018 to July 2022 were candidates. Inclusion criteria were as follows: (1) patients who underwent standard PCNL in the prone position and (2) patients older than 20 years. Exclusion criteria were: (1) patients with other life-threatening complications, such as hemothorax; (2) patients who underwent simultaneous surgery, such as transurethral resection of the prostate; (3) patients who were unable to discontinue anticoagulants; (4) patients who underwent miniaturized PCNL; and (5) patients who underwent multitract PCNL.
We defined significant tract site bleeding as the presence of obvious bleeding in the visual field across the parenchymal tract when the sheath of the balloon dilator was being withdrawn. According to these criteria, we sorted out 91 cases of recognized puncture site bleeding by carefully watching the puncture tract where either nephrostomy catheter insertion (n = 60) or bipolar cauterization (n = 31) was performed. Finally, we compared three groups, including the no/negligible bleeding group (i.e., the no procedure group), nephrostomy group, and cauterization group (Fig. 1).
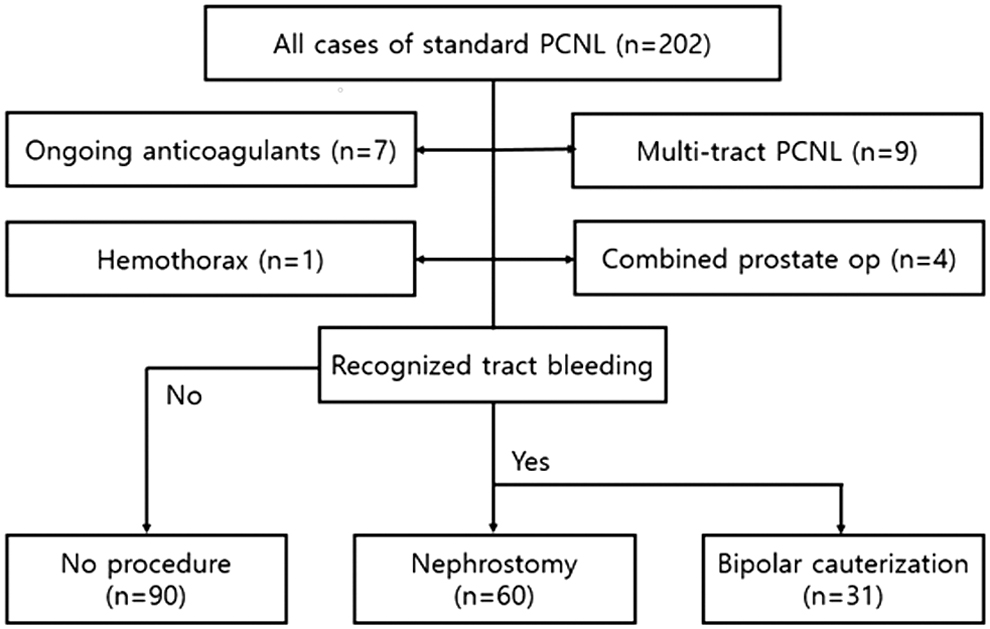
Study design. Either nephrostomy catheter insertion or electrocauterization was performed when obvious bleeding was identified or when the visual field across the parenchymal tract was disturbed while withdrawing the sheath of a balloon dilator. Finally, three groups were compared.
The patients' charts were reviewed carefully to obtain the following information: age, sex, body mass index, underlying diseases such as diabetes mellitus and hypertension, preoperative and postoperative (2 hours after operation) hemoglobin, preoperative platelet count, preoperative prothrombin time international normalized ratio, total operation time, puncture site (lower calix, mid-calix, or upper calix), use of nephrostomy, use of bipolar cauterization instead of nephrostomy, transfusion after operation, and angioembolization after the operation. Finally, all preoperative CT scans were reviewed to obtain the following information: stone laterality, maximal stone length, Hounsfield unit, and Guy's stone score.
Surgical technique
All PCNL procedures (n = 202) were performed by three expert endourologists who had previously performed over 100 PCNL procedures. We always performed standard PCNL in the prone position, and in most cases, the PCNL tract was created by an urologist. We created a PCNL tract using a 30 Fr and an X-Force nephrostomy balloon dilator (Bard, Covington, GA, USA). We positioned the sheath of the balloon dilator in place and then inserted a 24 Fr Universal Nephroscope (Richard. Wolf, Knittlingen, Germany) to continue with the procedures. Stone fragmentation and dust suction were performed using an ultrasound lithotripor (Richard. Wolf). Two or three prong forceps were used to retrieve the fragments. As mentioned previously, at the end of the procedure, the sheath of the balloon dilator was removed carefully to observe whether there was significant bleeding throughout the puncture site.
In patients with noticeable puncture site bleeding, an 18 Fr nephrostomy tube was placed through the sheath of the balloon dilator before the sheath was removed, or a bipolar resectoscope (TURis 2.0, 30°) with its sheath (26 Fr) was inserted into the sheath of the balloon dilator to control the bleeding lesion of the PCNL tract while the sheath of the balloon dilator was slowly removed. A loop-type, button-type, or roller-type electrode tip was used during bipolar cauterization. During bipolar cauterization, surgeons apply minimal pressure to the bleeding focus for a few seconds (Supplementary Video S1). Normal saline (3000 cc) was used as irrigation fluid for PCNL and for cauterization via natural drainage (∼1 m from the operation table) using a disposable Y-shaped TUR irrigation set.
Data analysis
SPSS (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0.; IBM Corp., Armonk, NY, USA) was used for the statistical analysis. The comparison of continuous variables was performed using one-way analysis of variance or the Kruskal–Wallis test based on the result of the Levene test for equality of variances. The comparison of categorical variables was performed using the chi-squared test or Fisher's exact test. The Bonferroni correction method was used to perform post hoc analysis. A value of P < .05 was considered significant.
Results
The characteristics of all the patients who underwent standard PCNL are summarized in Table 1.
The Characteristics of All the Patients Who Received Single Tract Standard Percutaneous Nephrolithotomy (n = 181)
Data are given as IQR or frequency (%).
ΔHb is the value that subtracts preoperative hemoglobin from 2-hour postoperative hemoglobin.
BMI, body mass index; Hb, hemoglobin; INR, international normalized ratio; IQR, interquartile range; PCN, percutaneous nephrostomy; PLT, platelet; PT, prothrombin time.
The mean age was 57.4 years, and 58.6% patients were men. Over half of the single-tract standard PCNL procedures (54.7%) were performed via a lower caliceal approach. A total of 24.3% of patients underwent percutaneous nephrostomy (PCN) in advance by a radiologist. The overall transfusion rate was 14.4%, and 2.2% of all enrolled patients underwent angioembolization. An 18-Fr nephrostomy catheter was placed in 60 patients (33.1%), whereas electrocauterization instead of nephrostomy tube placement was performed in 31 patients (17.1%). In fact, there were 4 more patients in whom electrocauterization was performed. However, multitracts were created in those patients (Fig. 1), and we excluded them from this study. For comprehensive comparison, we compared all available preoperative parameters and postoperative outcomes among the three groups: the no significant bleeding group and the bleeding groups, including the nephrostomy group and cauterization group (Table 2).
Comparison of Outcomes According to Management of Bleeding at the End of Percutaneous Nephrolithotomy
Data are given as IQR or frequency (%). One-way ANOVA was applied for continuous variables and chi-squared test was used for categorical data.
Kruskal–Wallis test was applied instead of one-way ANOVA owing to failed Levene test for equality of variances.
ΔHb is the value that subtracts preoperative hemoglobin from 2-hour postoperative hemoglobin.
Fisher's exact test was applied instead of chi-squared test.
Bonferroni-adjusted p-value between Group 2 and Group 3.
ANOVA, analysis of variance; BMI, body mass index; Hb, hemoglobin; INR, international normalized ratio; IQR, interquartile range; PCN, percutaneous nephrostomy; PLT, platelet; PT, prothrombin time.
One transfusion (3.2%) was performed in the cauterization group, whereas 41.7% of patients in the nephrostomy group received a transfusion (P < .001). Similarly, the drop in hemoglobin at 2 hours postoperatively was significantly less in the cauterization group than in the nephrostomy group (P < .001). Because only 4 patients underwent angioembolization, the statistical value of this procedure was not significant in the nephrostomy group or the cauterization group, although angioembolization was more frequently performed in the nephrostomy group than in the entire cohort (P = .016).
Consequently, the total number and severity of complications were highest in the nephrostomy group, and the length of postoperative hospital stay was the longest in the nephrostomy group, where the longest stay was 8 days (total length of hospital stay was 10 days). Lower caliceal puncture was more frequently performed in the no procedure group (no significant bleeding group), whereas upper caliceal puncture was more frequently performed in the cauterization group. However, puncture location did not significantly differ between the nephrostomy group and the cauterization group. All the other parameters did not differ between the two groups.
Discussion
Puncture site bleeding is an important PCNL-related complication. To avoid puncture site bleeding, surgeons should carefully review the preoperative computed tomography scan to achieve puncture correctness. 5 Nevertheless, no one will disapprove of a bleeding control method for standard PCNL if it is reliable. Based on this study, we believe that bipolar cauterization is an excellent alternative to control puncture site bleeding during standard PCNL. For this method, the most important thing is to examine the parenchyma of the tract while very carefully withdrawing the sheath of the balloon dilator at the end of the procedure. In this study, cases in which the visual field across the tract remained relatively clear, under gravity-dependent normal saline irrigation did not require a transfusion after the procedure.
The subjective assessments of the tract site bleeding could be a limitation of these kinds of studies, including this study. To the best of our knowledge, there has been no method that can quantitatively assess tract site bleeding during PCNL. To evaluate a bleeding control method more objectively, a prospective study in which groups (e.g., patients who were subjected to a method versus those who were not) are divided regardless of bleeding severity is needed. However, such manner would let patients in for a procedure regardless of bleeding severity, or vice versa. In addition, comparing two groups regardless of bleeding severity leads to the effect of a treatment (or a procedure) on bleeding control diluted. The low rate of transfusion reported in previous studies explains this phenomenon. 2 A prospective study evaluating a hemostatic agent that was conducted by Istanbulluoğlu et al. showed the effect of a hemostatic agent on tract site bleeding 6 despite failing to provide any criterion for tract site bleeding before the authors finished their operations. In this sense, our method to decide a procedure for tract site bleeding may be reasonable with respect to ethical issues in the real world.
Torque is another reason for PCNL-related bleeding. The appropriate choice of puncture site and use of flexible nephroscopy are important to minimize the torque, especially in patients with multicaliceal stones.5,7 Guy's stone score is usually applied to classify the anatomical complexity of renal stones. 8 According to Said et al., stone complexity may contribute to PCNL-related bleeding. 9 In this study, stone complexity was deemed to be higher in both bleeding groups, although the statistical result was not significant. However, by looking at all the cohorts (Table 2), it was found that the choice for puncture site was different in both bleeding groups (more cases of upper pole puncture) (P = .010), which is consistent with a report showing that bleeding risk is higher in upper pole puncture than in lower pole puncture. 10 However, between the nephrostomy group and cauterization group, stone complexity and puncture location were not significantly different between each other, which indicates that there was no significant difference in the level of difficulty.
Cauterization, as a technique to prevent puncture site bleeding, is simpler for small arterial bleeding than for venous bleeding. According to our experiences, we recommend using button-type or roller-type electrode tips with sufficient time and minimal contact pressure (Supplementary Video S1). When the bleeding was controlled and the visual field was no longer disturbed, the need for postoperative transfusion was extremely decreased. Moreover, once the bipolar resectoscope was ready, cauterization could be performed without increasing the total operating time.
As mentioned previously, there were some limitations: (1) the retrospective nature of this study and (2) subjective sorting of the groups owing to the lack of standard criteria for site bleeding. However, the findings in the this study not only supports those in previous clinical studies 2 but also helps us to rediscover the usefulness of cauterization while avoiding the development of hyponatremia.
Conclusion
The electrocauterization of bleeding points at the end of PCNL could safely and efficiently decrease tract site bleeding and reduce the need for transfusion. To date, further prospective studies are needed.
Footnotes
Authors' Contributions
Design of the work by D.S.L., H.Y.K.; Data acquisition by J.M.Y., D.S.L., Analysis and interpretation of data for the work: D.S.L., H.Y.K.; Drafting the work by J.M.Y., D.S.L.; Revising the work by D.S.L., Final approval of the version and agreement to be accountable for all aspects of the work by D.S.L., J.M.Y., H.Y.K.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.