
Abstract
Aims:
This study aimed to review our surgical experience of laparoscopic adrenalectomy (LA) for adrenal masses in the pediatric age group.
Materials and Methods:
The electronic medical records of all patients younger than 18 years of age who underwent LA between 2016 and 2023 were retrospectively reviewed. Children with adrenal tumors localized to the site of origin without evidence of encasement of major vasculature or involvement of adjacent organs were considered for LA. Patients with diagnosis of malignant adrenal tumor on preoperative work-up underwent open adrenalectomy. Data were collected regarding demography, clinical presentation, hormonal workup, imaging, duration of surgery, transfusion requirement, conversion rate, postoperative recovery, duration of intravenous (i.v.) analgesia and hospital stay, pathology, complications, and status at follow-up.
Results:
Between 2016 and 2023, LA adrenalectomy was performed in 11 patients (6 boys and 5 girls) with a mean age of 46.3 (8–120) months. A functional tumor was detected in 6 (54.5%) children, manifesting clinically with Cushing's syndrome (3), virilization (1), feminization (1), or Conn's syndrome (1). Seven (63.6%) tumors originated from the right adrenal, and 4 (36.4%) from the left adrenal gland. The mean tumor weight and size was 49.1 (10–80) g and 5.6 (3–8) cm, respectively. Histopathology included adrenal adenoma (5), ganglioneuroma (3), ganglioneuroblastoma (1), myelolipoma (1), and intermediate adrenocortical tumor (1). The mean surgery duration was 186.6 (120–265) minutes. Intraoperative blood transfusion was required in 2 (18.2%) patients and none required conversion. Full feeds were resumed at 42.7 (24–60) hours, i.v. analgesia requirement was for 54.5 (36–72) hours and mean hospital stay was 5.1 (3–8) days. All patients were symptom-free with no recurrence at mean follow-up period of 50.6 (3–83) months.
Conclusions:
In children with well-circumscribed, localized, and noninvasive adrenal tumors, LA is feasible, effective, and safe with all advantages of minimally invasive surgery.
Introduction
Adrenalectomy in children is mainly indicated for resection of adrenal tumors, arising either from adrenal cortex or medulla. Although the adrenal cortex is the site of origin of adenoma, carcinoma, or hyperplasia, neuroblastoma, ganglioneuroma, or phaeochromocytoma may arise from the adrenal medulla. 1 Pediatric adrenocortical tumors (ACTs) are extremely rare, accounting for only 0.2% of all tumors and 10%–25% of all adrenal tumors in children. 2 The most common (60%–75%) adrenal lesions in children are neuroblastic tumors (neuroblastomas, ganglioneuroblastomas, and ganglioneuromas). About 2%–10% of adrenal lesions are pheochromocytomas. Sarcomas, metastasis, calcifications, cysts, and hematomas are very rare lesions of the adrenal gland and represent only ∼2.5%–6% of all cases.3,4 Adrenal tumors can be further classified based on their secretory status as hormonally active (“functional”) or hormonally silent (“nonfunctional”).
Gagner et al. were the first to report laparoscopic adrenalectomy (LA) in 1992. Since then, minimally invasive approach has rapidly become the gold standard for adrenalectomy in adult patients. 5 However, the application of LA in children is still a matter of debate. The relative infrequency of pediatric adrenal tumors, wide spectrum of pathologies, higher frequency of malignancy, disproportionately large tumor size in relation to the small body habitus, technical challenges in small infants, availability of appropriate size instruments, and a long learning curve have all been postulated to be the underlying factors.1,2 Compared with the extensive literature available on LA in adult patients, the published evidence for LA in children is limited to few retrospective case series, 6 couple of case–control studies,7,8 and no randomized controlled trial.
The aim of this study was to review the surgical experience of LA in children with varied clinical presentations and diverse adrenal pathologies.
Materials and Methods
This study was performed in accordance with the ethical standards of the institutional and/or the national research committee and with the Declaration of Helsinki as revised in 2013 or comparable ethical standards. This was a retrospective review of the electronic medical records of all children who underwent LA between January 2016 and April 2023 at our institute and were operated by the primary authors (A.M. and S.M.).
Inclusion criteria
LA was considered in all patients younger than 18 years of age with localized adrenal tumors without signs of vascular encasement or adjacent organ involvement on preoperative imaging. 9
Exclusion criteria
Patients with adrenal tumors with signs of vascular encasement or adjacent organ involvement on preoperative imaging or a confirmed preoperative diagnosis of malignancy (e.g., neuroblastoma, adrenocortical carcinoma) were excluded and managed with an open adrenalectomy, as and when indicated.
Study variables
Data regarding demography (e.g., age, sex, height, weight), clinical presentation, diagnostic workup (hormonal profile, imaging features) were collected. Intraoperative variables included were duration of surgery, requirement of blood transfusion, conversion rate, and need for drains. Postoperative end points were time to full feeds, requirement of intravenous (i.v.) analgesia, hospital stay, medical and surgical complications, histopathology, and size of lesion at pathologic examination. Follow-up focused on clinical and hormonal status, any evidence of recurrence and overall survival. Electronic medical records were reviewed and patient data were compiled.
Preoperative workup
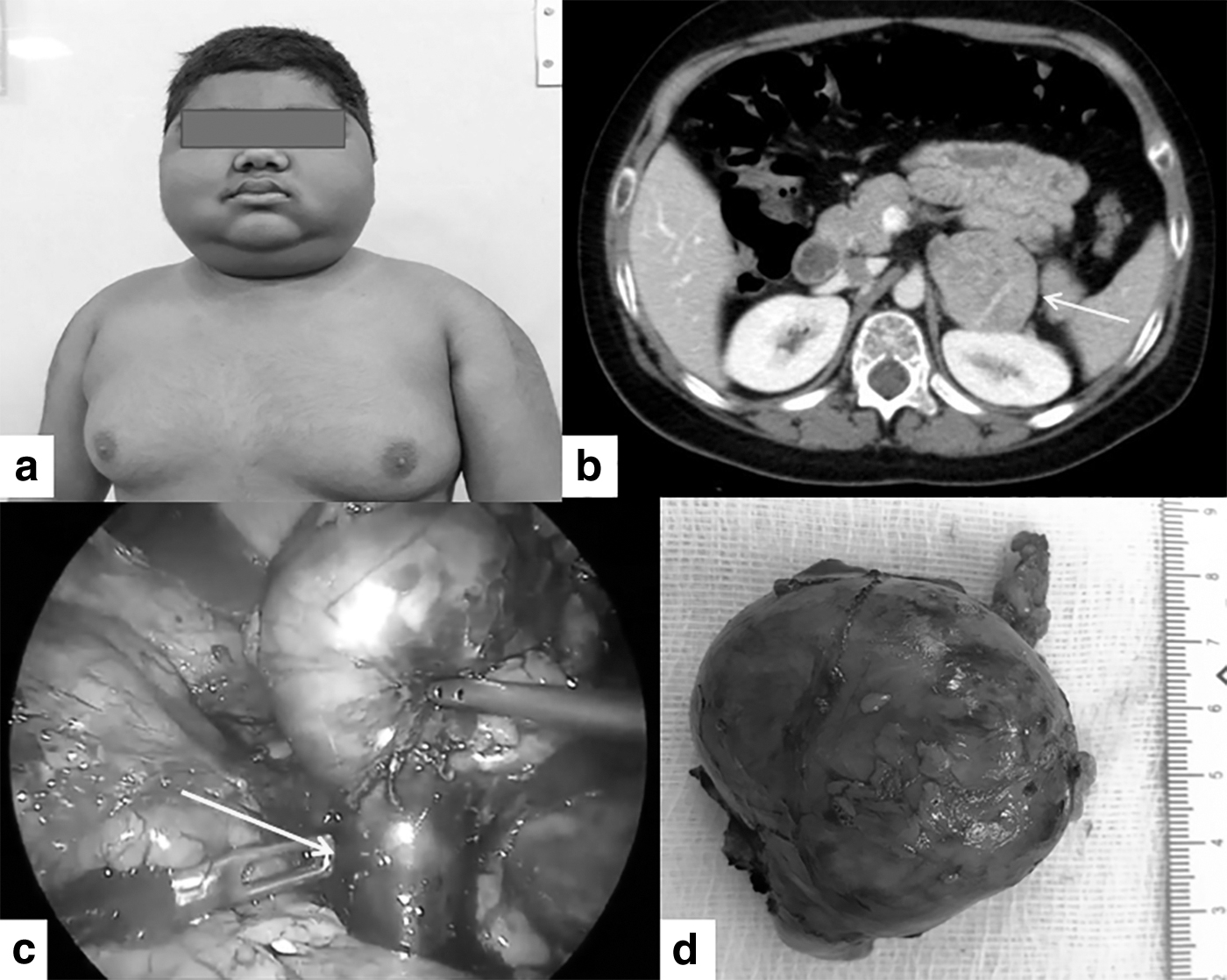
A thorough clinical evaluation was followed by a comprehensive preoperative workup in all cases. This included a detailed biochemical and hormonal assay, and various imaging studies. Ultrasonography and a triple-phase computed tomography were carried out in all patients to characterize the primary lesion, evaluate any invasion of major vessels or adjacent viscera, and to rule out any metastases. In addition, patients with suspected adrenal medullary lesions underwent 123 I—Meta iodo benzyl guanidine scintigraphy, when necessary.
Surgical technique
Patients were generally admitted 24 hours before surgery and bowel preparation was not routinely used (Video 1: Video demonstration of laparoscopic right adrenalectomy for right adrenal adenoma in a 42-month-old girl who presented with precocious puberty, https://1drv.ms/v/s!ApvYHcdANSnkwATKbLii2mmWopAb?e=kSBMM2; Video 2: Video demonstration of laparoscopic left adrenalectomy for left adrenal adenoma in an 11-month-old boy with Cushing's syndrome, https://1drv.ms/v/s!ApvYHcdANSnkwCBbwQbQo_lI65eZ?e=VEyfKH). Adequate blood pressure control was ensured in all patients who were receiving medication for hypertension. Perioperative stress steroid dose was given at induction of anesthesia, as indicated by the pediatric endocrinology team.
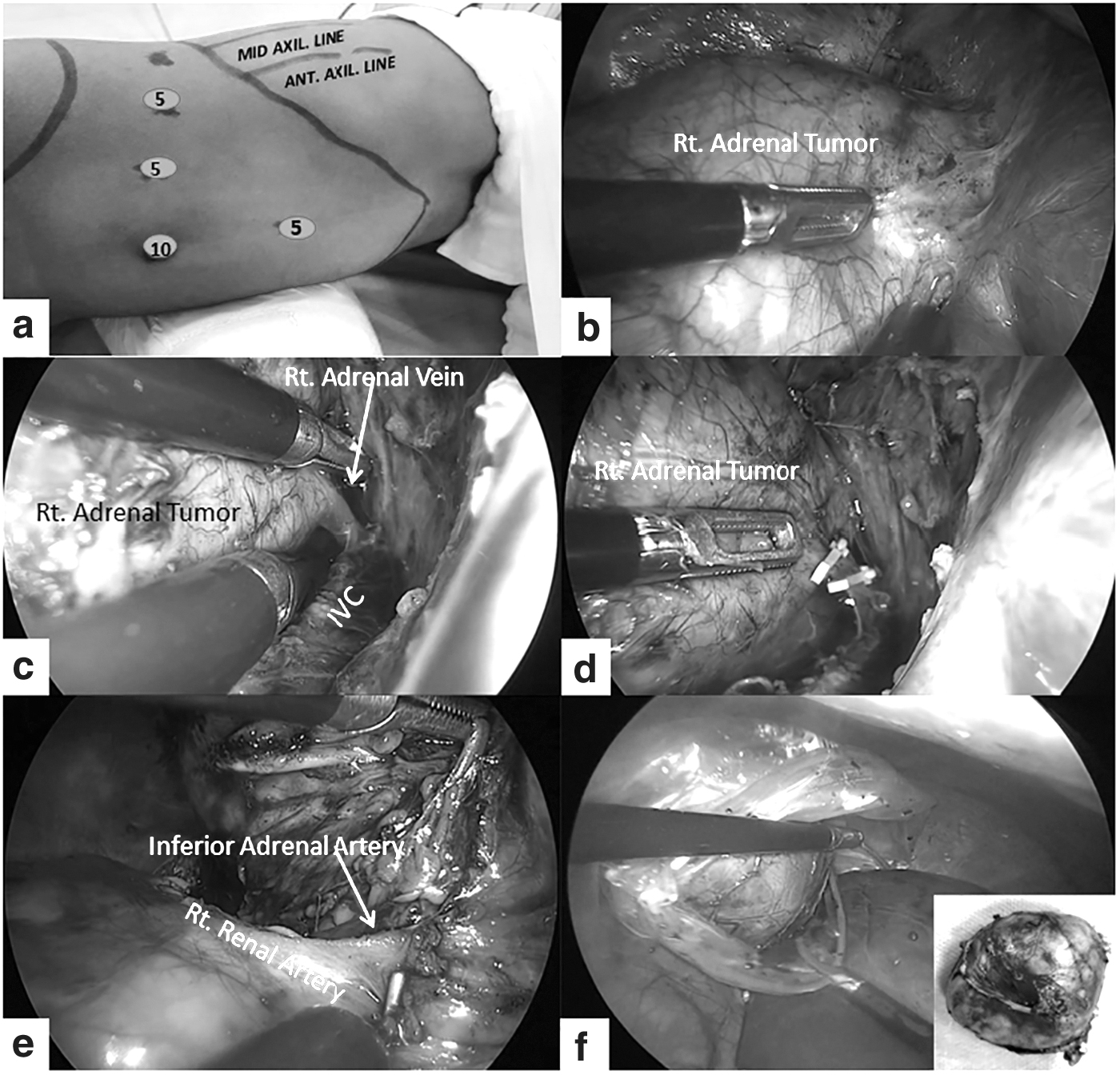
All patients underwent LA by the lateral transperitoneal approach using four ports as described previously.10,11 Following induction of anesthesia, the patient was intubated in the supine position and an orogastric tube and a urinary catheter were inserted. Then, a lateral decubitus position (operative side upwards) was made with a roll inserted under the flank to increase the distance between costal margin and iliac crest (Figs. 1a, 2a). Video monitor was placed behind the patient and the surgeon with the assistants stood facing the patient on the side opposite the side of the adrenal tumor (Fig. 2a). The head end of the operating table was raised to ∼15°–25° reverse Trendelenburg position. Open technique was used to insert the first 10-mm port at the umbilicus and gain access to the abdomen.
Laparoscopic right adrenalectomy in a 42-month-old girl who presented with precocious puberty

Laparoscopic left adrenalectomy in an 11-month-old boy with Cushing's syndrome
Pneumoperitoneum of 8–10 mmHg was maintained with a carbon dioxide flow of 2–4 L/minutes. Three 5-mm ports were then inserted under direct vision of a 30° telescope; one in upper midline, close to xiphoid process, and two more laterally, close to costal margin (Figs. 1a, 2a).
On the right side, after division of the right triangular ligament, liver was retracted medially and superiorly with a grasper, thus exposing the upper pole of right kidney, right adrenal, and the inferior vena cava (IVC) (Fig. 1b). The posterior peritoneum was then incised over the lateral border of the IVC in a craniocaudal direction to expose the adrenal vein, which is short on the right side and enters the IVC laterally (Fig. 1c). The adrenal vein was carefully dissected, doubly clipped with application of hemlock clips on either side, and divided in between (Fig. 1d). Dissection of the adrenal gland was performed in a medial to lateral direction with a Harmonic scalpel (Ethicon Endosurgery, Inc., Cincinnati, OH) or a monopolar cautery hook, carefully cauterizing and sectioning all small vessels (Fig. 1e).
Once the adrenal was completely free of all attachments, the adrenalectomy specimen was placed in an endobag (Covidien, Mansfield, MA) and removed intact through an augmented port incision (Fig. 1f). The tumor bed was inspected, adequate hemostasis was ensured, and port sites were closed without routine use of abdominal drains.
On the left side, the dissection was started by medial mobilization of the left colon, spleen, and tail of the pancreas, which then exposes the renal fascia. The fascia covering the renal hilum was incised and the main trunk of the left renal vein was identified. The left adrenal vein was then visualized at the superior border of the left renal vein, dissected carefully, doubly clipped on either side with hemlock clips, and divided (Fig. 1b, c). The left adrenal was then further dissected all around circumferentially, as described for the right side (Fig. 1d). After extraction of the adrenalectomy specimen in an endobag (Fig. 1e, f), hemostasis was ensured, the left colon was repositioned to its normal anatomical location, the port sites were closed, and drains were not routinely used.
Postoperative protocol
Extubation was carried out on table at the end of surgery. Orogastric tube was routinely removed in all patients before extubation. The patients were allowed liquid diet 6 hours after surgery and gradually progressed to solids by the first postoperative day. Intravenous analgesia was administered with a patient-controlled analgesia pump. Patients were discharged home once they resumed full feeds and were pain free with oral analgesics.
Follow-up
All patients were followed-up at regular intervals with clinical examination, imaging, and hormonal studies. The frequency and duration of follow-up and also the type of imaging and hormonal assays varied depending on the final histopathology report and the preoperative functional status of the tumor.
Results
During the study period between January 2016 and April 2023, 11 children (5 girls and 6 boys) with a mean age of 46.3 (8–120) months underwent LA. Mean weight and height of the cohort was 17.2 (7.4–26.9) kg and 93 (64.5–121) cm, respectively. Six (54.5%) children presented with a functional (hormonally active) tumor, clinically manifesting as Cushing's syndrome (3), virilization (1), feminization (1) or Conn's syndrome (1). One of the Cushing's syndrome patients also had features of virilization, indicating a mixed tumor. Hypertension was noted in 5 of the 6 patients with functional tumors at presentation, the only exception being the patient with feminization. Tumor laterality was 7 (63.6%) tumors arising from the right adrenal, and 4 (36.4%) arising from the left adrenal gland (Tables 1, 2).
Demographic, Clinical, and Diagnostic Features of Children Undergoing Laparoscopic Adrenalectomy (2016–2023)
Criteria positive for calculating Weineke score.
BP, blood pressure; HPE, histopathology.
Hormonal Profile of Children Undergoing Laparoscopic Adrenalectomy (2016–2023)
17-OHP, 17-hydroxyprogesterone; ACTH, adrenocorticotropic hormone; DHEA, dehydroepiandrosterone; FSH: follicle-stimulating hormone; LH, luteinizing hormone; ONDST, overnight dexamethasone suppression test; PRA, plasma rennin activity.
The mean tumor size and weight was 5.6 (3–8) cm and 49.1 (10–80) g, respectively. The mean operating time was 186.6 (120–265) minutes. Intraoperative blood transfusion was required in 2 (18.2%) patients owing to bleeding during dissection. None of the patients had any other intraoperative complication, tumor rupture/spill, or conversion to an open procedure (Table 3). One patient required hand assistance at the end of the dissection for transfixing the stump of an unusually large adrenal vein and for intact removal of the tumor (Fig. 3). Abdominal drains were placed in only 2 (18.2%) patients in the initial part of the learning curve, which were removed 48 hours after surgery in both patients.
Intra-Operative and Post-Operative Outcomes of Children Undergoing Laparoscopic Adrenalectomy (2016–2023)
Details of “terminal hand assist” modification have been provided under “Discussion”.
Postoperative complications were observed in 5 (45.5%) patients and all were classified as Clavien–Dindo grade I complications. These included fever (1), port site infection (1), muscular strain (1), polyuria (1), and metabolic alkalosis with hypokalemia (1). All complications resolved with conservative management. Full feeds were resumed at a mean duration of 42.7 (24–60) hours. The mean duration of i.v. analgesia use and hospital stay was 54.5 (36–72) hours and 5.1 (3–8) days, respectively (Table 3).
The final histopathology included adenoma (5), ganglioneuroma (3), ganglioneuroblastoma (1), myelolipoma (1), and intermediate ACT (1). At a mean follow-up of 50.6 (3–83) months, all children are symptom-free with normal hormonal status and no evidence of recurrence (Tables 1, 3).
Discussion
In children, small body habitus, need for fine instrumentation, and acquisition of advanced laparoscopic skills among surgeons poses unique challenges for LA. Several issues regarding LA in children continue to be debated which have been addressed in parts by various authors in the published literature previously. These include the minimum age or weight criteria, the maximum size limit for the adrenal tumor, and the role of LA for malignant lesions.1,2,6–9
Tumor size is not unanimously accepted as a predictive factor of LA outcome in children and an upper size limit that can be considered safe for LA is not well established.2,11 Previous recommendation of 6 cm upper limit was based on the risk of malignancy of adrenal tumors in adults and may not be applicable to children. 12 Sturgeon et al. studied 457 adults with adrenocortical carcinoma (ACC) from the Surveillance, Epidemiology, and End Results database and reported that the risk of a cortical tumor being ACC rises from 10% when ≥4 cm to 19% when ≥6 cm, and to as high as 47% when ≥8 cm. 13 In recent years, various authors have indicated the feasibility of LA for resection of large tumors >6 cm in adults, assuming there is no evidence of significant local infiltration.14,15
In pediatrics, consideration should be given to the tumor size relative to the patient's size and individualized decision should be taken for every case. 12 Other features such as adjacent organ involvement or vascular encasement should also be considered before proceeding for LA. In this study, all tumors up to 8 cm in diameter (mean diameter 5.6 cm) were safely resected by LA, all of whom had no vascular or adjacent visceral involvement on the preoperative image studies (Figs. 1–3, Table 1).
Most authors have previously concluded that there is no minimum weight or age criteria for selecting patients for LA.7,16 Our series reaffirms this suggestion as there were 3 (27.3%) infants in our cohort with the youngest patient being 8 months old and weighing 7.4 kg (Table 1). Of these 3 infants, 2 had presented with florid Cushing's syndrome, which is associated with significant physiological (hypertension, poor healing, perioperative stress steroids) and technical (increased intraperitoneal fat, difficult conversion) challenges. However, LA could be safely performed in all without any adverse events (Table 3). This suggests that irrespective of age or weight of the patient, it is reasonable to proceed laparoscopically if the surgical team is experienced in performing LA.
The application of minimal access surgery for treating malignant adrenal tumors in children has remained challenging and controversial owing to the infiltrative nature of these lesions (e.g., neuroblastoma) and concerns for recurrence in case of spillage (e.g., ACC). An open approach is usually considered mandatory for treating ACC as it often presents with necrosis, hemorrhage, or fibrosis. These make the lesions particularly susceptible for rupture, bleeding, or peritoneal and trocar site seeding, even when local infiltration is absent. 2 There is a lack of high level evidence regarding the optimal surgical strategy for ACC owing to its rarity and also because of the fact that determination of the type of cortical tumor (i.e., adenoma versus carcinoma) can only be determined after adrenalectomy, as preoperative biopsy for ACT is usually not recommended. 17 In our study, we excluded any patient for LA whenever there was a strong clinical and/or imaging suspicion of ACC.
The mainstay of treatment for most neuroblastomas remains the traditional open approach, because of its large size and propensity for local infiltration. At present, the experience with laparoscopic resection of smaller tumors is growing with increasing use of minimal access surgery for diagnosis and staging of larger and infiltrative lesions (e.g., laparoscopic biopsy).8,18 In a recent article, Chang et al. compared 87 patients with neuroblastoma treated either by open approach or by laparoscopy. The authors concluded that for children with localized neuroblastoma who have no image-defined risk factors, LA is safe and effective with similar survival and recurrence rates compared with open surgery. 19
Another important concern about LA for adrenal tumors in children is tumor spillage and trocar site recurrence, which if occurs in cases of ACC, can significantly upstage the tumor and result in an unfavorable outcome. 20 To prevent trocar site implantation, an endoscopic retrieval bag (endobag) should always be used to retrieve the tumor that prevents direct contact between the tumor and port site. If the tumor is too large to be easily removed through the enlarged umbilical port, a Pfannenstiel (supra-pubic) incision may be needed to retrieve the endobag with the tumor. In our experience, none of the patients had any of these complications as it is our protocol to never morcellate the adrenal tumor and always place it in an endobag for retrieval through one of the enlarged port sites (Figs. 1f, 2e).
The transperitoneal approach for LA has several advantages compared with the retroperitoneal approach. Transperitoneal approach allows good exposure of hilar structures with adequate working space, bilateral control when needed, sampling of abdominal lymph nodes, and most surgeons are familiar with this approach. 2 The retroperitoneal approach is favored by few authors as it gives direct access to the adrenal gland, avoids mobilization of the colon, and has a low risk of adjacent intraperitoneal organ damage. 21 However, we concur with suggestions by various authors to avoid the retroperitoneal approach for large tumors (>5 cm), right-sided tumors, and bilateral tumors; the risk of hemorrhage owing to poor vascular control, limited working space, and long learning curve being the main hindrances.7,11,22
Owing to their multiplicity and fragility, the dissection and sealing of adrenal blood vessels is usually considered technically challenging. The right adrenal vein is generally more difficult to dissect and ligate than the left adrenal vein because of its short length between the gland and the IVC. Studies have previously reported an intraoperative hemorrhage rate of 1.4%–2.2%2,16 and rate of conversion of 9%–10%16,23 consequent to bleeding. In our series, we used hemlock clips in all patients to ligate the adrenal vein (Figs. 1d, 2c) after careful dissection, and adrenal arteries were usually divided with a Harmonic scalpel (Ethicon Endosurgery, Inc.) or monopolar cautery hook (Fig. 1e). Intraoperative blood transfusion was required in 2 (18.2%) patients in our cohort owing to bleeding during dissection and none of the patients required conversion.
The “terminal hand assist” modification has been used previously in adults to complete difficult laparoscopic procedures, without conversion to an open procedure. 24 It helps during difficult mobilization in the final stages of the procedure, while avoiding a hand port in the early part of dissection. In one of our patients with a large left adrenocortical adenoma causing Cushing's syndrome (patient No. 4), an unusually large and dilated adrenal vein was found intraoperatively (Fig. 3). It was not possible to safely ligate this large vein with laparoscopic instrumentation. Surgeon's right hand was inserted into the abdomen by enlarging the left subcostal port site by a transverse muscle splitting incision. Incision is given in such a way that the hand is snugly fitting in the wound to prevent any gas leakage from the lateral edges. Hand assistance was useful in this case in safely clamping (with surgeon's fingers) and transfixing the adrenal vein stump and excising the relatively large mass without any tumor rupture or spillage.
In our series, the mean time to full feeds of 42.7 (24–60) hours, i.v. analgesia requirement of 54.5 (36–72) hours, and mean hospital stay of 5.1 (3–8) days are longer than reported in literature previously.6–8,10–12 Reasons for these could be variable, for example, few outliers in the series like patient No. 10 with Cushing's syndrome had postoperative polyuria with associated hypokalemia, leading to paralytic ileus and achieved full feeds at 72 hours, thus affecting the mean. In addition, most of our patients had large tumors >5 cm (mean tumor diameter 5.6 cm), which were retrieved intact through an enlarged port incision. This can probably explain the longer requirement of i.v. analgesia in these patients. Ours is a tertiary care referral institute catering to a large population from far flung areas in North India. Sometimes, the patients may stay for an extra 24–36 hours in the hospital for safe observation before embarking on a long journey home. This might explain the longer mean hospital stay of 5.1 (3–8) days.
In this study, we have described our initial surgical experience with LA in children with adrenal tumors. Patient selection for LA by detailed hormonal and imaging evaluation is critical to avoid pitfalls and complications. We selected children with localized adrenal tumors without signs of local infiltration or vascular involvement. We did not have a lower limit for age/weight or an upper limit for the size of the adrenal tumor. One of the limitations of our study is the diverse histopathological diagnosis of the tumors that makes the cohort heterogeneous. In addition, the small number of cases and absence of a control group offers only level 4 evidence. However, the predominant level for publications in pediatric minimally invasive surgery is level 4 as very often like in the case of adrenalectomy, open approach is used for more infiltrative and malignant tumors, and randomizing patients to a control arm is neither feasible nor ethical.
Conclusion
In children with well-circumscribed, localized, and noninvasive adrenal tumors, LA is feasible, effective, and safe with all advantages of minimally invasive surgery. The patient selection for this procedure is of critical importance to avoid complications and have a good oncologic outcome. LA may soon become the preferred operative approach in this select group of patients.
Footnotes
Acknowledgment
The authors express deep gratitude to all their colleagues from Departments of Pediatric Endocrinology, Pathology, Radiology, and Anesthesiology, who were involved in the care of these patients.
Authors' Contributions
A.M.: Conceptualization (lead); writing—original draft (lead); writing—review and editing (equal). S.M.: Methodology (lead); Writing—original draft (supporting); writing—review and editing (equal). P.B.N.: Conceptualization (supporting); writing—review and editing (equal). P.K.: Writing—original draft (supporting); Writing—review and editing (equal).
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the Declaration of Helsinki as revised in 2013 or comparable ethical standards. Ethical approval was waived in view of the retrospective nature of the study and all the procedures performed were part of the routine care.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.