
Abstract
Objective:
To investigate the application value, feasibility, and safety of modified single-port laparoscopic surgery in the treatment of pediatric inguinal hernia.
Methods:
One hundred and twenty cases of children with indirect inguinal hernia admitted from 2017 to 2022 were enrolled in the Control and Observation groups, with 80 and 40 cases, respectively. They underwent traditional open high ligation of the hernia sac and modified single-port laparoscopic high ligation of the hernia sac, respectively. The operation duration, surgical incision size, intraoperative bleeding, postoperative hospital stay, first ambulation time, and hospitalization expenses were compared between the two groups, as well as the incidence of surgical complications in the two groups.
Results:
The surgical incision size, intraoperative bleeding, postoperative hospital stay, and first ambulation time of the Observation group were less than those of the Control group. There was no significant difference in operation duration or hospitalization expenses between the two groups. Only two cases in the Observation group showed suture knot reactions after surgery, with no incision infection, inguinal hematoma, iatrogenic cryptorchidism, etc. The overall incidence of complications in the Observation group was lower than that of the Control group.
Conclusion:
Modified single-port laparoscopic surgery for inguinal hernia in children has the advantages of minimal invasiveness, and enhanced recovery, along with fewer complications and recurrence, hence it is worthy of recommendation in clinical practice.
Introduction
Inguinal hernia in children, usually referred to as pediatric hernia, is mostly the indirect inguinal hernia. It is a common and frequently occurring disease in pediatric surgery, with a higher incidence among males. Its pathogenesis indicates that the peritoneal sheath is either not closed after birth or just closed incompletely. In some instances such as violent crying or chronic cough, the pressure in the abdominal cavity becomes too high that the abdominal organs or tissues protrude from the internal ring to form an indirect inguinal hernia. If the hernia contents are incarcerated and not returned in time, it could lead to ischemia of those tissues and organs, causing severe consequences such as intestinal necrosis, intestinal perforation, and more. Therefore, timely surgical treatment is of great importance to the health and life of these pediatric patients.
Because abdominal wall muscles may continue to enhance during the growth of children, the vast majority of indirect hernia in children can be just treated with high ligation of the hernia sac. In the early days, conventional open surgery for high ligation of the hernia sacs was mainly used in the treatment of children’s hernia disease. In recent years, with the development of minimally invasive surgery, laparoscopic techniques are also widely used in pediatric hernia surgery.1–4 Laparoscopic hernia ring ligation has the same basic purpose as traditional high ligation of the hernia sac via the inguinal incision. According to the number of trocars, it can be categorized into the three-port method, double-port method, and single-port method.5–7 The hernia ring is ligated either by completely laparoscopic intraperitoneal knotting or by laparoscopy combined with extraperitoneal knotting using various hernia needles.8–9
In the single-port method, laparoscopy is used for observing only, without additional trocar or operating instruments. Thus, no chopsticks effect is caused by instrument collision. It assists in the extracorporeal ligation and closure of the hernia rings under laparoscopic vision. 10 Most literature reported the use of end-close hernia needles, modified Kirschner wires, straight abdominal suture needles, large round needles, # 9 gauge needles, and channel puncture devices.11–13 Lately, some experts and scholars have attempted to use double-hook hernia needles and pediatric hernia sac closure devices to perform the surgery. 14 All these methods have certain drawbacks such as difficult operating and restructuring, insufficient effective length, sharp and easy to injure, unable to inject water for separation, or requiring specialized equipment. In addition, using the double-strand thread formed in the first puncture to pull the single-strand thread from the second puncture out of the abdominal cavity is cumbersome and requires a second puncture, which increases the chance of soft tissue injury and bleeding, and inevitably leads to the ligating or hooking of other abdominal wall tissues.
Therefore, based on continuous clinical practice, we modified and improved the techniques. Using the epidural puncture needle and green guidewire, with the aid of saline or air separating, the hernia ring was accurately ligated by Prolene suture outside the peritoneum via transumbilical single-port laparoscopy. In this work, surgical data of children with indirect inguinal hernia admitted to our hospital from 2017 to 2022 were collected for comparative analysis, aiming to investigate the application value, feasibility, and safety of modified single-port laparoscopic surgery in the treatment of pediatric inguinal hernia.
Materials and Methods
Clinical materials
Children with indirect inguinal hernia admitted to our hospital from 2017 to 2022 were randomly enrolled as the research subjects. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. The study was approved by the Medical Ethics Committee of the Affiliated Hospital of Medical University [Approval Number [2019] FYFELLSZ No. (209)]. All cases were confirmed by ultrasonography before surgery, which met the diagnostic criteria for indirect inguinal hernia. The advantages and limitations of each surgical method were preoperatively informed, allowing the guardians of the children to choose independently. Written informed consent was obtained from the legal guardians of all children before surgery. According to the different surgical methods chosen, patients were included in the Control and Observation groups, with 80 and 40 cases, respectively. All children had non-incarcerated hernias. There were no significant differences in age, body weight, and other medical conditions between the two groups, which were comparable (Table 1). Exclusion Criteria: Patients who had undergone abdominal surgery within 3 months, and those with cryptorchidism, severe cardiopulmonary impairment or coagulopathy, and loss of consciousness.
Comparison of General Data Between Two Groups
P < 0.05 considered statistically significant.
Statistical analysis
SPSS statistical software was used for data analysis. After the normality test, measurement data were expressed as mean ± standard Deviation (x̄ ± s) with the t-test for comparison between groups, whereas counting data was represented as percentages (%) with the χ2 test. P < 0.05 was considered statistically significant.
Surgical methods
Control group
The patient underwent general anesthesia and traditional open high ligation of the hernia sac. In his supine position, a transverse incision of about 2 cm was made in the suprapubic crease above the inguinal ligament. The incision was carried through the subcutaneous tissue down to the external oblique aponeurosis. The external oblique was cleared to expose the external ring and inguinal ligament. The cremasteric fibers were separated in order to approach the hernia sac, which lay in front and toward the inner side of the spermatic cord. The sac was opened and inspected carefully before its contents were replaced within the peritoneal cavity. The inferior epigastric artery could be identified by palpation just outside the internal ring. The sac bridge was transected and divided. The proximal sac was dissected up to the level of the internal ring, with care taken to avoid injury to the vas deferens. The sac neck was closed by placing a suture ligature proximal to the internal ring. The distal sac was amputated or left untouched. Electrocautery was used when necessary. No other abnormalities were present during the inspection. The external oblique and subcutaneous tissue were interruptedly sutured, followed by an absorbable subcuticular suture for the skin. A normal diet was resumed around 6 hours after the operation, and no routine anti-infection medication was given.
Observation group
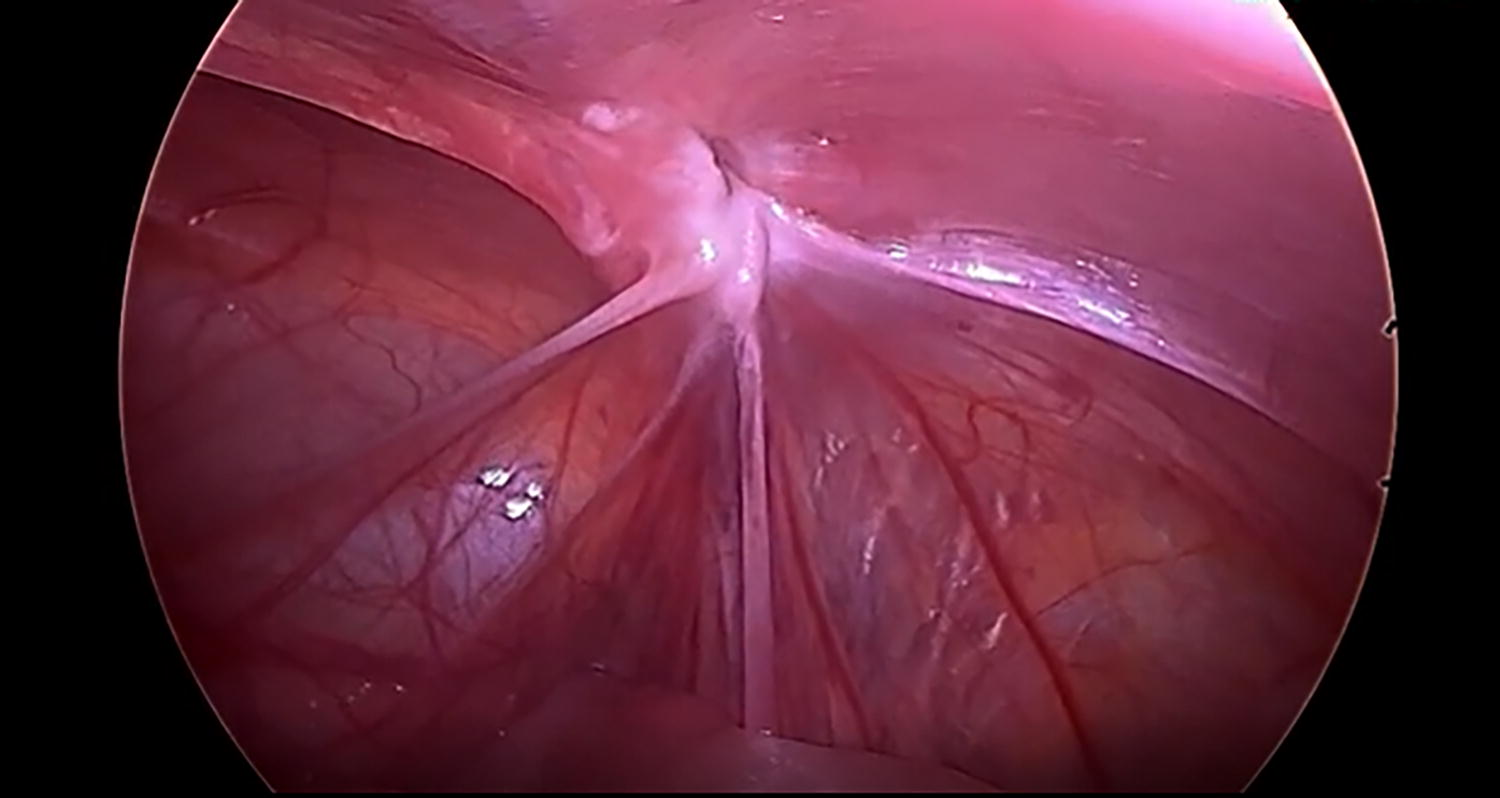
The patient underwent general anesthesia and modified single-port laparoscopic high ligation of the hernia sac. Preoperative urination was required to empty the bladder. A supraumbilical incision of about 0.5 cm was made, before establishing pneumoperitoneum pressure of about 7 mmHg by pneumoperitoneum needle puncturing. Through incision puncture, a 5-mm trocar and then a laparoscope were passed as the observing port. In a supine position with the feet higher than the head, it was shown under laparoscopic vision that the internal inguinal ring was enlarged, with the inferior epigastric vessels lying on its inner side, while the inguinal canal and sometimes the scrotum were inflated. Equivalent to 12 o’clock of the internal ring under laparoscopic vision, a skin incision of about 1 mm was made, through which an epidural needle (SCW Medicath Ltd.) punctured to the extraperitoneal space slightly above the internal ring and separated the medial half-circle of peritoneum along the extraperitoneal space (Fig. 1). A few milliliters of normal saline or air was filled via the epidural needle sleeve to facilitate the separation, while care should be taken to avoid injury to the inferior epigastric vessels, vas deferens, and spermatic vessels. After the epidural needle bypassed the vas deferens and spermatic vessels, it was penetrated into the peritoneal cavity, and a folded 3-0 Prolene thread was inserted through the needle sleeve to retain the thread loop in the abdominal cavity (Fig. 2). 15 After introducing a green-0.025″ guidewire into the abdominal cavity through the epidural needle sleeve, the sleeve was withdrawn away from the unfolded ends of the Prolene thread. Guided by the green guidewire, the needle sleeve navigated back to the extraperitoneal space following the original needle passage. The guidewire was removed, and the lateral half-circle of the peritoneum was separated from above the internal ring along the extraperitoneal space before the needle reentered the peritoneal cavity through the previous peritoneal puncture. Then the needle sleeve, with a single 3-0 Prolene thread passed inside, was introduced into the preset folded thread loop (Fig. 3). The sleeve was removed, and the unfolded ends of the preset thread loop were pulled out, which in turn would take out the single 3-0 thread within the loop. After extruding air and fluid from the inguinal canal and scrotum, the 3-0 Prolene suture was closed and multi-knotted outside the body, which would retract beneath the skin (Fig. 4). No active bleeding was detected. After counting gauzes and instruments, the laparoscope set was removed, and the CO2 was drained out of the abdominal cavity. The trocar incision was closed by the layered suture with absorbable thread. A normal diet was resumed around 6 hours after the operation, and no routine anti-infection medication was given.
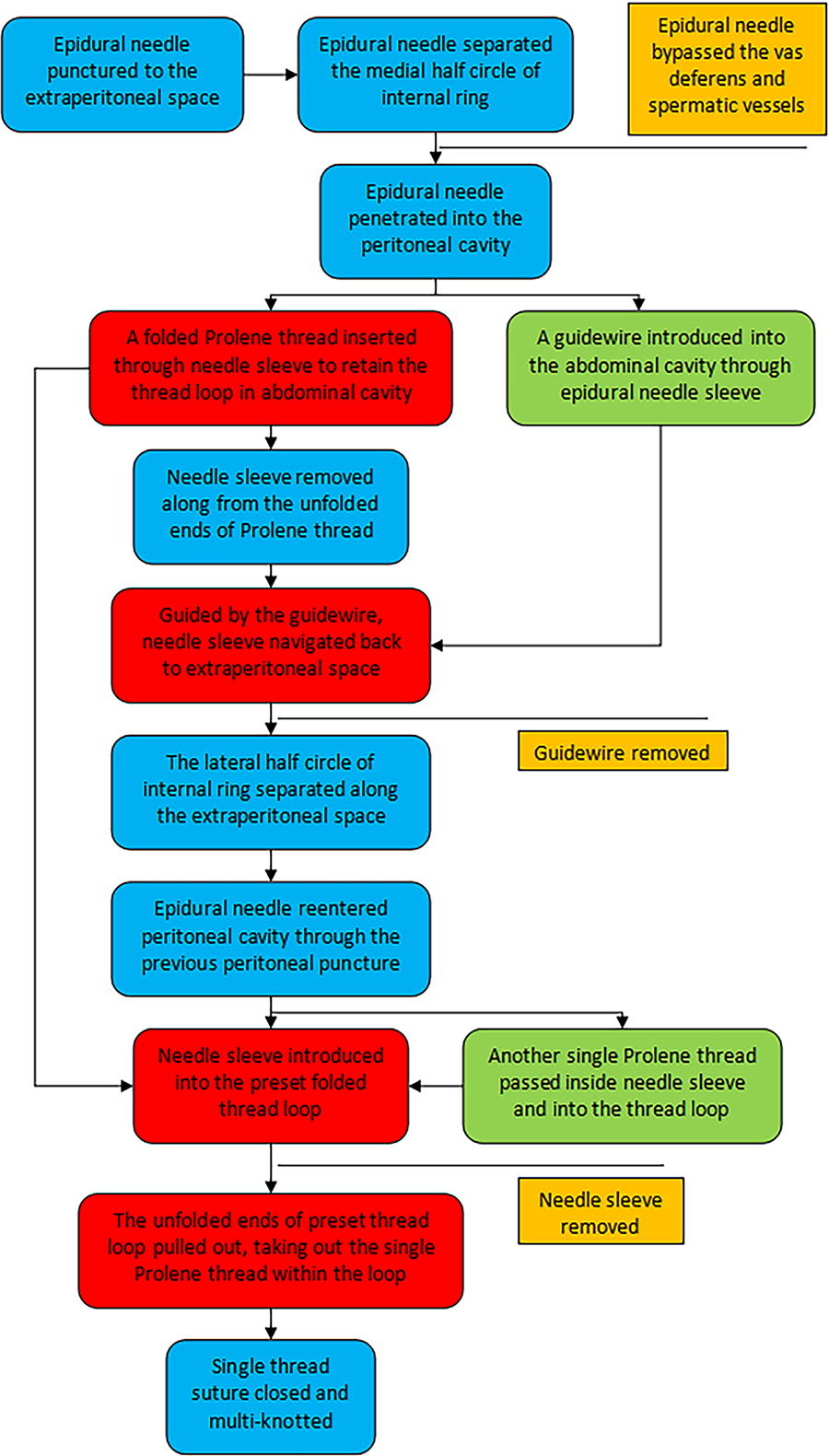
Flow chart of the modified single-port laparoscopic surgery for pediatric inguinal hernia.

Illustrations of the modified single-port laparoscopic surgery for pediatric inguinal hernia (

The needle sleeve, with a single 3-0 Prolene thread passed inside, was introduced into the preset folded thread loop.
Pulling out the unfolded ends of the preset thread loop would, in turn, take out the single 3-0 thread within the loop, which was tightened and knotted outside the body.
Outcome measures and follow-up
The operation duration, surgical incision size, intraoperative bleeding, postoperative hospital stay, first ambulation time, and hospitalization expenses of the two groups were observed and measured. The incidence of surgical complications was compared between the two groups, including postoperative uroschesis, suture knot reaction, or foreign body sensation, incision infection, inguinal and scrotal hematoma or obvious edema, testicular atrophy or iatrogenic cryptorchidism, hydrocele, or hernia recurrence. All cases were followed up for 12–36 months through outpatient revisits and telephone calls.
Results
The surgical incision size, intraoperative bleeding, postoperative hospital stay, and first ambulation time of the Observation group were less than those of the Control group. There was no significant difference in operation duration or hospitalization expenses between the two groups (Table 2). Only two cases in the Observation group showed suture knot reaction after surgery, with no incision infection, inguinal hematoma, iatrogenic cryptorchidism, etc. The overall incidence of complications in the Observation group was lower than that of the Control group (Table 3).
Comparison of Intraoperative and Postoperative Indices Between Two Groups (
P < 0.05 considered statistically significant.
Comparison of Postoperative Complications Between Two Groups [n (%)]
P < 0.05 considered statistically significant.
Discussion
In contrast to adult inguinal hernia, the anatomical layers of the inguinal region in children are hard to recognize, while the hernia sac (peritoneum) is thin. The sac in traditional high ligation of the hernia sac, sometimes difficult to find, is highly vulnerable to ripping during dissection. This is more likely to cause tissue injury to iliohypogastric/ilioinguinal nerves, spermatic vessels, and vas deferens, as well as postoperative hematoma/scrotal edema, iatrogenic cryptorchidism/testicular atrophy, even impairing reproductive ability in adulthood. In some instances, the hernia sac is not ligated enough, or there is too much tissue to be ligated tightly, either of which could result in a small secondary hernia sac, leading to the increased recurrence. In addition, there are other risks such as the difficulty in detecting occult hernia. In contrast, laparoscopic surgery does not damage the anatomical structure of the inguinal region. Moreover, due to the amplification effect of laparoscopy plus the expansion of the hernia sac caused by pneumoperitoneum, the internal ring is easy to find, and the inferior epigastric vessels, spermatic vessels, and vas deferens can be more clearly identified, thereby reducing the injury to vessels, nerves, vas deferens, and the incidence of related complications.
In clinical practice, we attempted to implement the ambulatory surgical mode for the modified single-port laparoscopic procedure and gained promising results. Compared to other techniques, its special characteristics and advantages are considered as follows: (1) With its suitable size and particular arc and slope on the tip, the epidural puncture needle of 16G size is conducive to elevating the peritoneum during the procedure and can proceed beneath the peritoneum by adjusting the direction, all of which makes it preferable to the traditional hernia needle for separating the extraperitoneal space.16–18 (2) The use of guiding material, such as an epidural catheter or guidewire, is necessary for this operation to assure the same puncture path. By one puncture in the abdominal wall, the entry and exit tunnels are maintained on the same path under its guidance, avoiding the postoperative pain induced by multiple punctures and the ligation on different layers. In terms of guidewire selection, the green-0.025″ guidewire is of appropriate thickness, hardness, and good compliance (Fig. 5). It has a flexible atraumatic tip for optimal flexibility and minimized trauma. (3) A small amount of normal saline or air (total vol. < 5 mL) is filled into the extraperitoneal space through the needle during the procedure. With the aid of saline or air separating, the vas deferens and vessels can be separated from the peritoneum more easily, which prevents iatrogenic ligation. Extruding air and fluid before closing the suture also reduces postoperative inguinal and scrotal edema. (4) In terms of suture selection for hernia ring ligation, 3-0 Prolene thread has higher strength and is less prone to suture knot reaction than absorbable or silk thread.

Green-0.025″ guidewire has the appropriate thickness, hardness, and good compliance.
However, the single-port laparoscopic method may also have a certain degree of risks or complications.19–21 Such laparoscopic ligation of the hernia ring requires a relatively high level of operator skill. 22 Sometimes in the single-port method, the needle instrument is unable to puncture into the extraperitoneal space and bypass the vas deferens/spermatic cord in one-time success and may need repeated punctures, which can lead to bleeding and a blurred anatomical structure in the vas deferens/spermatic cord region, thereby increasing the risk of injury to vas deferens, spermatic, or iliac vessels, leading to complications such as extraperitoneal hematoma, testicular atrophy, etc. If the hernia sac is too thickened or edematous to identify the vas deferens and pampiniform spermatic vessels, it becomes more likely to puncture and injure the vas deferens or spermatic vessels, leading to bleeding. Especially when the needle instrument approaches the branch of inferior epigastric vessels on the inner side of the internal ring, it is not easy to manage the needle direction, which once too deep, may injure epigastric vessels, resulting in hematoma at the internal ring. In addition, there is the risk of postoperative hydrocele or recurrence due to neglect of the peritoneal gap.23–24
To avoid injury, reduce related complications, and ensure optimal outcomes, several guidelines should be followed during the procedure: (1) Preoperative urination is required to avoid interference with intraoperative exposure and maneuver or accidental injury to the bladder. (2) Blunt dissection of the peritoneum using the spoon-like epidural needle is less likely to injure adjacent vessels or cause a hematoma. Moreover, it is safer with the aid of saline or air separating to push aside the vas deferens and the vessels. (3) When separating the medial peritoneum of the internal ring, the puncture needle should proceed right beneath the peritoneum. It should neither go through the spermatic cord and vas deferens to avoid accidental ligation nor excessively jack the sac toward the abdominal cavity to avoid ligation of the sac body rather than the sac neck and decrease the chance of hernia recurrence. (4) When threading for suture of the medial and lateral half circles, the inlet and outlet for the needle should be at the same point and single path so that the hernia sac neck is tightly closed without leaving a gap, which prevents recurrence or hydrocele to the greatest extent. (5) Before closing the suture, the testis is repositioned, and the air is extruded from the hernia sac to avoid iatrogenic cryptorchidism and postoperative emphysema of the hernia sac. Non-absorbable thread like Prolene is used for ligation and is tied with multiple knots firmly, which could help reduce hernia recurrence.
However, this study has some limitations. Although it showed enhanced recovery and fewer complications, there was no significant decrease in operation duration or hospitalization expenses. In addition, the follow-up period was relatively short. Lastly, this was a single-center research, so it would be of greater value to include further data involving multi-centers.
Conclusion
In summary, this study investigates the modified single-port laparoscopic surgery in the treatment of inguinal hernia in children. Using the epidural puncture needle and green guidewire, with the aid of saline or air separating, the hernia ring was accurately ligated by Prolene suture outside the peritoneum via transumbilical single-port laparoscopy. It has the advantages of minimal invasiveness and enhanced recovery, along with fewer complications and recurrence; hence, it is worthy of recommendation in clinical practice.
Footnotes
Acknowledgments
The authors would like to acknowledge the support of the Operating Room and Medical Records Department of the Second Affiliated Hospital of Fujian Medical University.
Ethics Approval and Consent
The procedures used in this study adhere to the tenets of the Declaration of Helsinki. The study was approved by the Medical Ethics Committee of the Second Affiliated Hospital of Fujian Medical University [Approval Number [2019] FYFELLSZ No. (209)]. Written informed consent was obtained from the legal guardians of all children before surgery.
Data Availability
The data that support the findings of this study are available from the Medical Records Department of the Second Affiliated Hospital of Fujian Medical University, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the corresponding author upon reasonable request and with permission of the Medical Records Department.
Authors’ Contributions
Study conception and design: ZP. Zhou, JS. Huang, HP. Lin; Data acquisition: HP. Lin, JF. Zeng, ZZ. Qiu; Analysis and data interpretation: HP. Lin, JF. Zeng; Drafting of the manuscript: HP. Lin, JF. Zeng; Critical revision: ZP. Zhou, JS. Huang. All authors reviewed the manuscript and agreed to submit it for publication.
Disclosure Statement
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
Funding Information
This work was funded by the Quanzhou City Science & Technology Program of China [Grant Number 2019N100S].