
Abstract
Introduction:
Epigastric hernia repair is a common procedure performed on pediatric patients. These hernias have been demonstrated to be readily identified by ultrasound. This manuscript describes and assesses a novel technique in which ultrasound is used to identify and repair the hernias in a minimally invasive manner.
Methods:
A retrospective chart review evaluates all the ultrasound-guided epigastric hernia repairs done with prolene suture at one institution over 20 months. Operative details and postoperative complications were compared to patients who underwent traditional open epigastric hernia repair at the same institution during the same time frame.
Results:
Thirty-two pediatric patients underwent epigastric hernia repair between May 2021 and December 2022. Thirteen (41%) underwent the ultrasound-guided technique with prolene suture and using only a meniscus needle and no incision. Nineteen (59%) underwent standard open repair. There were no recurrences or postoperative complications in either group. The average operative time for the ultrasound hernia repair was 24.4 minutes, which was shorter than the average operative time of 33.6 minutes for the open repair (P = .08). In 3 ultrasound cases (23%), an additional epigastric hernia that had not been clinically apparent was identified and simultaneously repaired.
Conclusions:
Ultrasound-guided epigastria hernia repair is a feasible alternative to traditional open repair. It has a comparable safety and efficacy profile, has a short operative time, and has the advantages of being minimally invasive and having the ability to identify and repair concurrent epigastric hernias.
Introduction
Epigastric hernias make up about 5% of the hernias in the pediatric population. 1 They are caused by failure of the linea alba to approximate during fetal development, and usually appear as a sporadically painful bulge in the epigastric area at a median presenting age of 39 months.2,3 Repair is recommended even for asymptomatic lesions as these fascial defects can increase over time and become painful. 4 Repair is usually done through a 1–2 cm transverse incision made directly over the defect. The incision sometimes has to be enlarged when there is difficulty finding the fascial opening.4,5 Although the skin incision is small, it still heals with the appearance of a scar, and there have been several studies suggesting laparoscopic repair as a possible way to improve aesthetic outcomes, decrease operating time, and identify and repair other simultaneous epigastric hernias.4,6,7 These are limited studies, and ultimately, no laparoscopic procedure has gained wide acceptance. 5
This study describes a new novel technique: ultrasound-guided epigastric hernia repair (UEHR). Ultrasound has already been demonstrated to successfully identify fascial defects in pediatric epigastric hernias. 3 In UEHR, the epigastric hernia is repaired with the use of an ultrasound and a curved meniscus repair needle. The use of ultrasound allows for identification of other hernias, and the technique requires only two small needle pokes in the patient's skin, thus avoiding any incisional scar. This manuscript describes the UEHR technique used as well as the outcomes and safety profile in comparison to the standard open technique at one institution.
Materials and Methods
A retrospective chart review evaluated all pediatric patients who underwent UEHR as well as traditional open hernia repair between May 2021 and December 2022. The initial start of May 2021 was selected because that is when the specific UEHR technique described below was first implemented. IRB approval was obtained through the University of Michigan Institutional Review Board (HUM00231746). Patients were excluded if their hernia repairs did not include epigastric hernia, or if they were outside this date range. Data collected included demographics, operative details, as well as postoperative outcomes and complications. Major complications included hernia recurrence requiring reoperation. Minor complications included return to clinic or emergency department with any other postoperative-related problem, including skin infection or granuloma. All data were collected and analyzed in Microsoft Excel (Microsoft Corporation: Redmond, WA). Bivariate analyses were conducted using t-tests to assess for differences between the two groups. Analyses of significance were conducted with P < .05.
Description of procedures
The traditional open repairs were done in the operating room under general endotracheal anesthesia after the hernias were identified and marked in the preoperative areas. The procedures were done in the usual manner, in which an incision was made directly over the site of the hernia. The subcutaneous tissues are dissected down to the level of the fascia, herniated preperitoneal fat is reduced into the abdomen, and the defect is closed primarily with absorbable suture. The subcutaneous tissues and skin are then approximated.
The UEHRs were also done in the operating room after the hernias were identified and marked in the preoperative areas. After the induction of general endotracheal anesthesia, a linear ultrasound probe (L20-5 Linear Array, Zonare, Mountain View, CA) is used to visualize the entire linea alba to identify the site of the known hernia (Fig. 1) as well as discover any other fascial defects to be repaired. A meniscus repair needle (Smith & Nephew, Andover, MA; Fig. 2) is then inserted into the skin just inferior to the defect under ultrasound guidance. The needle is then pushed ∼1–2 mm lateral to the defect and then driven through the fascia at a point inferior to the defect (Fig. 3). The needle is then advanced deep to the fascia to a point superior to the defect and still ∼1–2 mm lateral to the defect, in vertical alignment with the inferior fascial entry point. It is then traversed back through the fascia again until it is superficial to the fascia (Fig. 4) and is then driven medially back in vertical alignment with the defect and the inferior skin insertion before exiting the skin superior to the defect. A size 2-0 prolene suture is then passed through the needle with the help of suction and the needle is removed, leaving the suture in place. The needle is then passed, via ultrasound-guidance, through the same needle skin sites and through the fascia inferior and superior to the fascia at two points ∼1–2 mm lateral to the defect on the opposite side of the first fascial entry points. The superior end of the suture is then passed through the needle with the help of suction, and the needle is again removed. This effectively makes a “U” stitch loop around the defect with the two suture ends both exiting the inferior needle entry point (Fig. 5). The suture is then pulled taught, tied, and the knot is buried beneath the skin. Local anesthetic is injected and a bilateral rectus sheath block is done under ultrasound guidance for further postoperative pain control.

Ultrasound identification of fascial defect.

The meniscus repair needle used in the procedure.

The curved meniscus needle can be seen piercing the fascia and traversing deep to it.

The curved meniscus needle can be seen pointing back up superficially before exiting the skin.
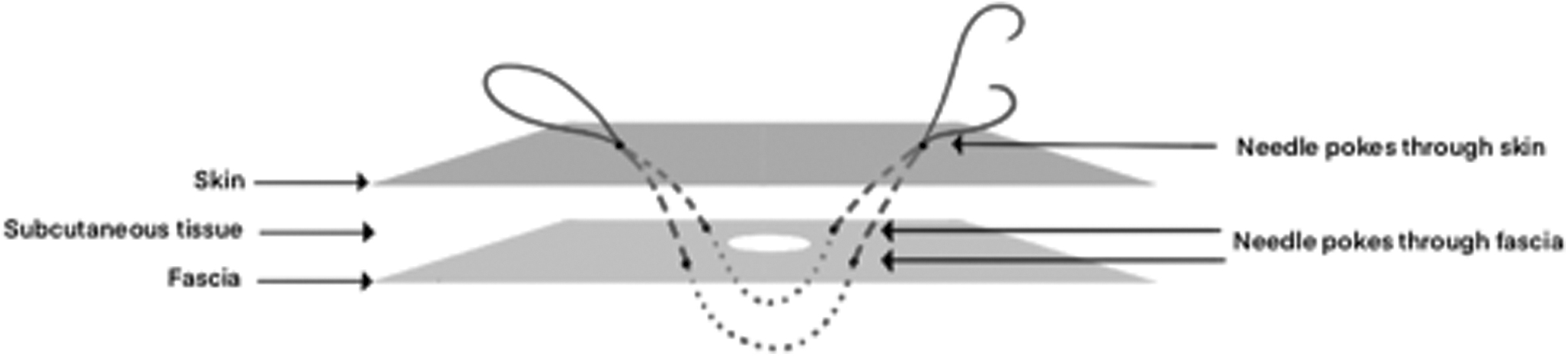
Illustration of the U-stitch that is ultimately achieved with this technique.
Of note, the procedure outlined above describes a repair done in a vertical manner, but the procedure can also be done in a manner that is transverse to the hernia defect, following the same general method. The prolene remains in place and is not removed.
Results
A total of 32 patients underwent epigastric hernia repair at C.S. Mott Children's Hospital between May 1, 2021 and December 31, 2022 (20 months). Thirteen patients (41%) underwent UEHR and 19 (59%) underwent traditional open repair. Each open repair was done by one of 11 pediatric surgeons, and vicryl was the suture used for closure of all the fascial defects except for one, which used polydioxanone suture. The 13 UEHR procedures were all performed by 1 pediatric surgeon who also has formal interventional radiology training, although most of the procedures included another attending surgeon or a fellow who was being trained in the procedure. Of note, although the option to convert to an open procedure existed in hypothetical cases of poor visualization or inability to reduce the hernia, none of the UEHR required conversion to the traditional open repair method.
The average age at time of operation for the traditional operation was 65.3 months (range: 11–206, standard deviation [SD]: 57.4). This was not significantly different than the average age of the patients who underwent UEHR patients, which was 50.5 months (range: 6–162, SD: 44.2, P = .41). Four of the traditional open patients (21%) underwent another procedure in addition to the epigastric hernia repair, including two umbilical hernia repairs, one incisional hernia repair, and one adenectomy. The average operating time for the patients who underwent open epigastric hernia repair only was 33.6 minutes (range: 23–73, SD: 14.7). In the UEHR group, there was 1 patient who underwent an additional procedure of orchiopexy. Also, in 3 cases (23%), a second epigastric hernia was discovered with the ultrasound and was subsequently repaired in addition to the known hernia. The average operating time for the remaining 9 patients who underwent single epigastric hernia repair only was 24.4 minutes (range: 10–36, SD: 9.9), which was on average 9.2 minutes shorter than the open repair (P = .08).
The average follow-up time for the open repair was 9.8 months (range: 3–19, SD: 5.2), and the average UEHR follow-up time of 14.4 months (range: 6–22, SD: 6, P = .04). There were no reported recurrences in either group and no patient in either group presented to the clinic or emergency room with any concerns for any other type of postoperative complication, including skin infection, seroma, and granuloma (Table 1).
Comparison of Operative Details Between Traditional Repair Versus Ultrasound-Guided Epigastric Hernia Repair
UEHR, ultrasound-guided epigastric hernia repair.
Discussion
This research demonstrates both the safety and efficacy of UEHR and is the first study to describe the use of this technique. The outcomes reported in this manuscript demonstrate that the procedure described above is not inferior to the standard open technique, with 13 patients demonstrating no recurrences and no other form of postoperative problems after an average follow-up time of over 1 year. The main benefits of UEHR over the traditional open technique include decreased average operative time, the ability to quickly identify and concurrently repair additional epigastric hernias, and improved cosmesis. Regarding decreased operative time, it should be noted that the UEHRs that are reported in this study also included a rectus sheath block. This was incorporated into the total procedure length, thus suggesting that the true operative times of the UEHRs alone are likely even shorter than what is reported. With regards to being able to identify additional hernias, both a laparoscopic repair and the UEHR described here highlight this important advantage over the traditional open repair. In this study, an additional epigastric hernia was found in 23% of the patients, while laparoscopic studies have similarly described a rate of newly discovered concurrent epigastric hernias between 10% 5 and 22%. 8
As mentioned previously, the third benefit of the procedure is improved cosmesis when compared to the traditional open repair, which requires an incision. Improved cosmesis has also been described as a benefit of the laparoscopic repair, with studies describing a transumbilical approach to hide the incision and thus decrease scarring.8,9 However, laparoscopic procedures still make incisions to insert the trocars and require tissue dissection which the ultrasound technique does not. Unlike both the open repair and the laparoscopic repair, the UEHR does not require any incision. The skin is only entered twice with a needle, and the resulting cosmesis is comparable to two simple needle pokes. Figure 6 demonstrates the cosmesis on a patient who underwent transverse UEHR repair. The needle pokes are barely visible 2 weeks after the procedure.

Cosmetic results of a transverse UEHR patient 2 weeks after the procedure. UEHR, ultrasound-guided epigastric hernia repair.
It should be noted that at our institution, the UEHR procedure details described above are the final successful result of multiple attempts using different techniques. Previous attempts had been made to perform an ultrasound-guided repair using other sutures such as silk and vicryl, as well as employing a simple interrupted stitch through the fascia. Ultimately, these techniques demonstrated some suture reactions and a low recurrence rate. This led to the development of the U-stitch procedure using prolene, described above, which produced the favorable results reported here.
There are several limitations to this study. The first includes the small sample size. Now that this procedure has been proven safe and effective, its continued application should result in larger studies analyzing the results, focusing on both recurrences as well as the quantity of additional epigastric hernias that are found. Further studies could also possibly incorporate parents' satisfaction with the cosmesis. Finally, it should be noted that the procedure is currently only performed by 1 pediatric surgeon. However, this surgeon has been training several attending surgeons and fellows to perform the procedure successfully, which promotes the idea that UEHR is an easy, reproducible, and feasible technique to perform epigastric hernia repair in the pediatric population.
Conclusions
UEHR is a novel technique that can be used for epigastric hernias in the pediatric population. It is safe, with no recurrences reported in this study, has a short operative time, and has the advantages of improved cosmesis as well as the ability to discover and simultaneously repair concurrent epigastric hernias that were not clinically apparent.
Footnotes
Acknowledgments
We would like to thank Sarah Fox and the entire Pediatric Surgery Research Team at the University of Michigan for assistance with IRB submission and project design.
Authors' Confirmation Statement
All authors attest that they meet the current ICMJE criteria for authorship.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant or funding from funding agencies in the public, commercial, or not-for-profit sectors.