
Abstract
Background:
The momentum of robotic surgery is increasing, and it has great prospects in pancreatic surgery. It has been widely accepted and expanding to more and more centers. Robotic distal pancreatectomy (RDP) is the most recent advanced minimally invasive approach for pancreatic lesions and malignancies. However, laparoscopic distal pancreatectomy (LDP) also showed good efficacy. We compared the effect of RDP with LDP using a meta-analysis.
Methods:
From January 2010 to June 2023, clinical trials of RDP versus LDP were determined by searching PubMed, Medline, and EMBASE. A meta-analysis was conducted to compare the effect of RDP with LDP. This meta-analysis evaluated the R0 resection rate, lymph node metastasis rate, conversion to open surgery rate, spleen preservation rate, intraoperative blood loss, postoperative pancreatic fistula, postoperative hospital stay, 90-day mortality rate, surgical cost, and total cost.
Results:
This meta-analysis included 38 studies. Conversion to open surgery, blood loss, and 90-day mortality in the RDP group were all significantly less than that in the LDP group (P < .05). There was no difference in lymph node resection rate, R0 resection rate, or postoperative pancreatic fistula between the two groups (P > .05). Spleen preservation rate in the LDP group was higher than that in the RDP group (P < .05). Operation cost and total cost in the RDP group were both more than that in the LDP group (P < .05). It is uncertain which group has an advantage in postoperative hospital stay.
Conclusions:
To some degree, RDP and LDP were indeed worth comparing in clinical practice. However, it may be difficult to determine which is absolute advantage according to current data. Large sample randomized controlled trials are needed to confirm which is better treatment.
PROSPERO ID: CRD4202345576.
Introduction
Long ago, open distal pancreatectomy was the standard method for treating benign or malignant lesions in the body or tail of the pancreas. However, now, laparoscopic distal pancreatectomy (LDP) and robotic distal pancreatectomy (RDP) are both minimally invasive treatments and are considered the preferred methods due to reduced intraoperative blood loss, higher spleen preservation rate, and faster postoperative recovery.1–5 A large international multicenter study 6 elaborated on the results of oncology and surgery for comparing RDP and LDP. The R0 resection rates of both are equivalent (75.7% RDP versus 69.3% LDP, P = .404), while RDP was associated with an increase in the number of lymph node resections (18 versus 16 nodes, P = .021).
There was no difference in overall survival and disease-free interval between RDP and LDP. From the perspective of surgical outcomes, RDP was associated with lower conversion rate (4.9% versus 17.3%, P = 0.001), more major complications (26.2% versus 16.3%, P = .019), and longer hospital stay (10 versus 8 days, P = .001). There was no unified conclusion yet on the clinical efficacy about comparison between RDP and LDP. To evaluate the true impact of RDP and LDP on clinical efficacy, a meta-analysis was conducted.
Materials and Methods
Study design
According to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, this study obtained a PROSPERO (registration) ID “CRD4202345576,” without the approval of the ethics committee.
Literature retrieval strategy
The literature from January 2010 to June 2023 was retrieved from Medline, EMBASE, and PubMed electronic databases. The keywords are as follows: “Robotic distal pancreatectomy,” “RDP,” “Laparoscopic distal pancreatectomy,”and “LDP.” In addition, all relevant publications, review articles, and citation lists included in the study were manually searched. The language of the literature was limited to English. Duplicate articles were deleted before the selected article was studied.
Data extraction and quality assessment
The authors (Liu Junguo, Yao Junchao, Jinjuan Zhang, and Cheng Lou) reviewed and screened the selected articles. And we extracted data from perioperative results. The Newcastle Ottawa Scale (NOS) was used to evaluate the quality of nonrandomized studies.
Study inclusion and exclusion criteria
The selected articles had to meet the following criteria
(1) All enrolled patients performed robotic or LDP; (2) studies about R0 resection, lymph node yield, conversion to open surgery, spleen preservation rate, intraoperative blood loss, postoperative pancreatic fistula, postoperative hospital stay, 90-day mortality, operation cost and total cost. (3) Randomized or nonrandomized controlled studies conducted or published over the years. (4) Clearly defined sample size, such as the number of cases in the RDP and LDP groups. (5) This study only involved English literature.
Exclusion criteria were as follows
(1) Sudy protocols; (2) letters to the editor; (3) summary of the meeting; (4) editorial; (5) posters; (6) case report; and (7) animal research.
Statistical analysis
Dichotomous variables were assessed using the odds ratios (ORs) with 95% confidence interval (CI), and continuous variables were evaluated by the weighted mean difference with a 95% CI. All results were performed for meta-analysis by using the Review Manager 5.3 software. Chi-square statistics was used to evaluate differences among studies. When there was no heterogeneity, a fixed-effect model was used. Otherwise, a random-effect model was used. The Begg's test and funnel plot were used to evaluate the likelihood of publication bias in the research. Statistical significance was set at a P < .05.
Results
Study population
A total of 38 studies were included through the inclusion and exclusion criteria of the study7–44 (Fig. 1). A total of 6743 patients received RDP (n = 2370) or LDP (n = 4373) treatment from January 2010 to June 2023. These articals were all nonrandomized controlled trials with high quality (Table 1).
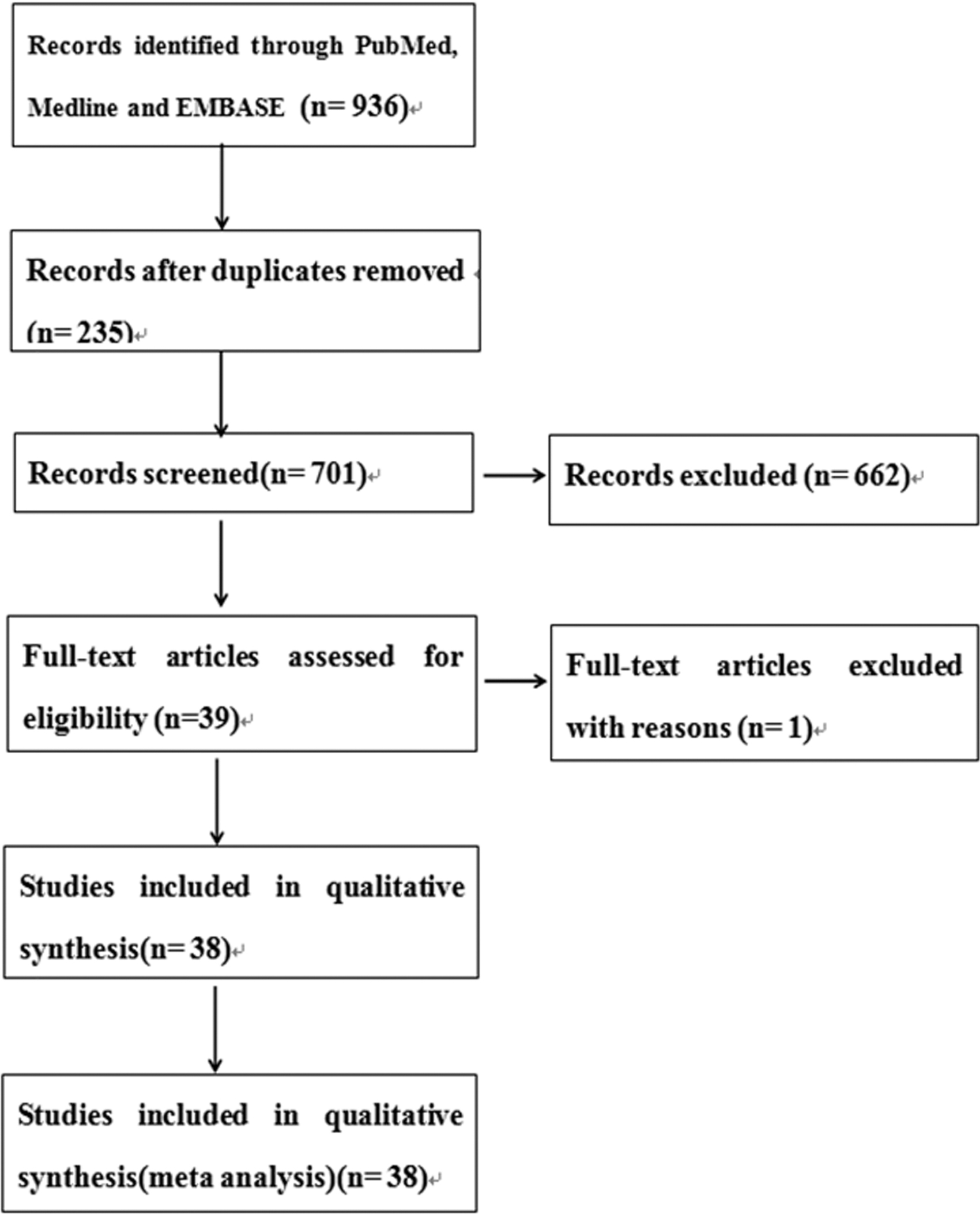
Diagram of the search strategy.
Methodological Quality of Studies Included in Meta-Analysis
According to the NOS for assessing the quality of nonrandomized studies, ≥5* is divided into meta-analyses.
LDP, laparoscopic distal pancreatectomy; NOS, Newcastle Ottawa Scale; RDP, robotic distal pancreatectomy.
Meta-analysis
Conversion to open surgery
There were 31 studies about analyzing conversion to open surgery (Fig. 2). Heterogeneity test among studies did not show difference (P = .12). A fixed-effect model was performed. Conversion to open surgery in the RDP group was less than that in the LDP group with a combined OR of 0.42 (95% CI: 0.34 to 0.53; P < .00001).
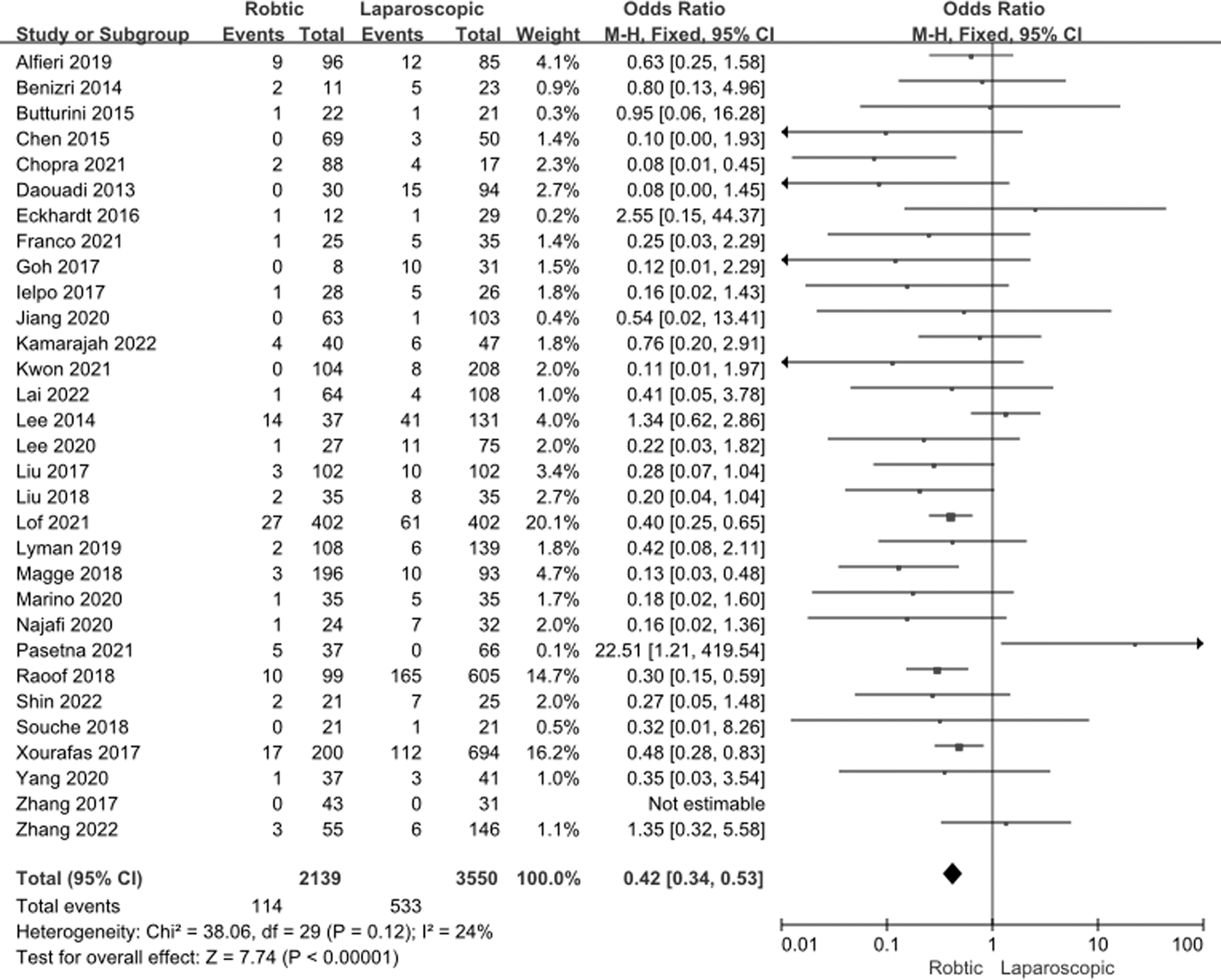
Fixed-effect statistical model of OR for conversion to open surgery after RDP versus LDP. LDP, laparoscopic distal pancreatectomy; OR, odds ratio; RDP, robotic distal pancreatectomy.
Spleen preservation rate
There were 14 studies about analyzing spleen preservation rate (Fig. 3). Heterogeneity test among studies did not show difference (P = .11). A fixed-effect model was used. Spleen preservation rate in the LDP group was higher than that in the RDP group with a combined OR of 3.01 (95% CI: 2.33 to 3.90; P < .00001)
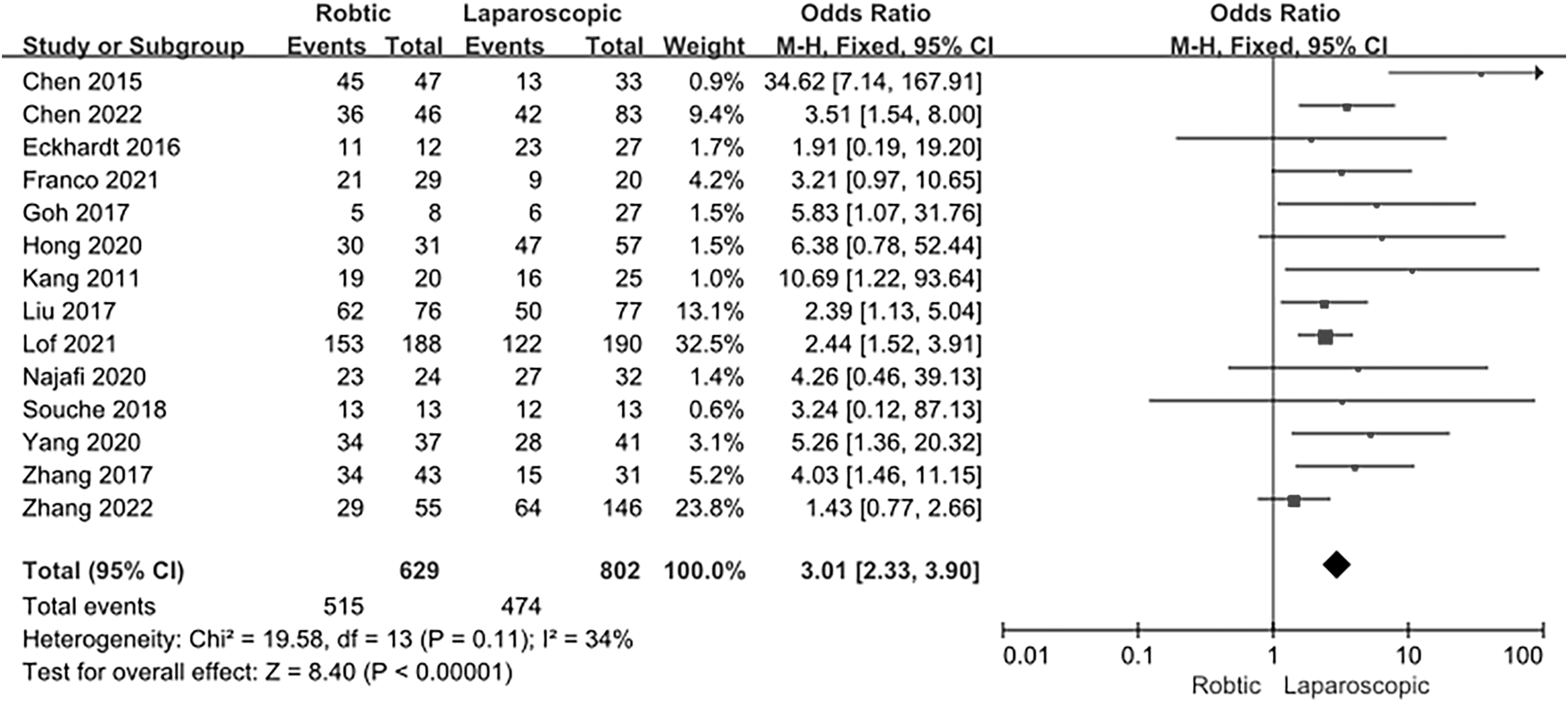
Fixed-effect statistical model of OR for spleen preservation rate after RDP versus LDP. LDP, laparoscopic distal pancreatectomy; OR, odds ratio; RDP, robotic distal pancreatectomy.
Intraoperative blood loss
There were 15 studies about analyzing intraoperative blood loss (Fig. 4). Heterogeneity test among studies showed statistical differences (P < .00001). A random-effect model was performed. Intraoperative blood loss in the RDP group was less than that in the LDP group with a combined OR of −53.9 (95% CI: −85.54 to −22.27; P = .0008)
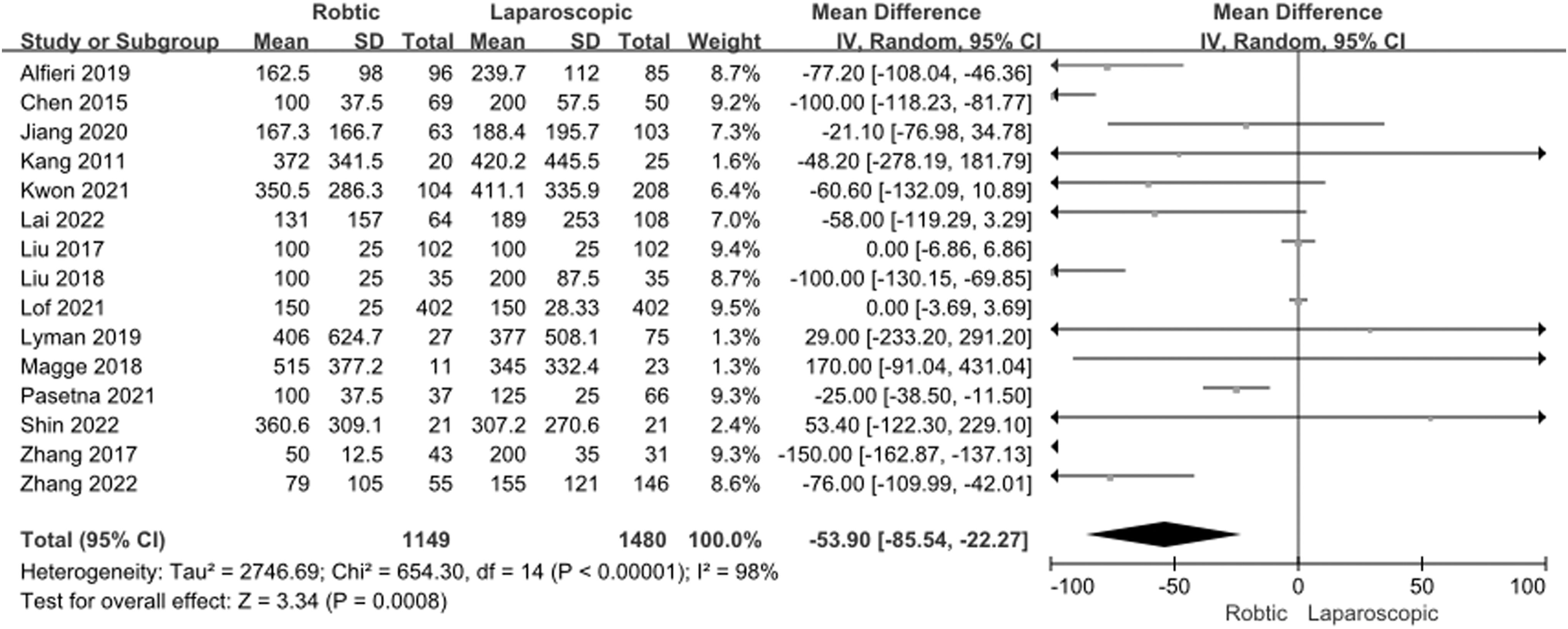
Random-effect statistical model of OR for intraoperative blood loss after RDP versus LDP. LDP, laparoscopic distal pancreatectomy; OR, odds ratio; RDP, robotic distal pancreatectomy.
Postoperative pancreatic fistula
There were 31 studies about analyzing postoperative pancreatic fistula (Fig. 5). Heterogeneity test among studies did not show difference (P = .99). A fixed-effect model was used. There was no statistical difference in postoperative pancreatic fistula between the two groups with a combined OR of 0.9 (95% CI: 0.76 to 1.06; P = .19)

Fixed-effect statistical model of OR for postoperative pancreatic fistula after RDP versus LDP. LDP, laparoscopic distal pancreatectomy; OR, odds ratio; RDP, robotic distal pancreatectomy.
Ninety-day mortality
There were 19 studies about analyzing 90-day mortality (Fig. 6). Heterogeneity test among studies did not show difference (P = .19). A fixed-effect model was used. Ninety-day mortality in the RDP group was less than that in the LDP group with a combined OR of 0.47 (95% CI: 0.24 to 0.93; P = .03)
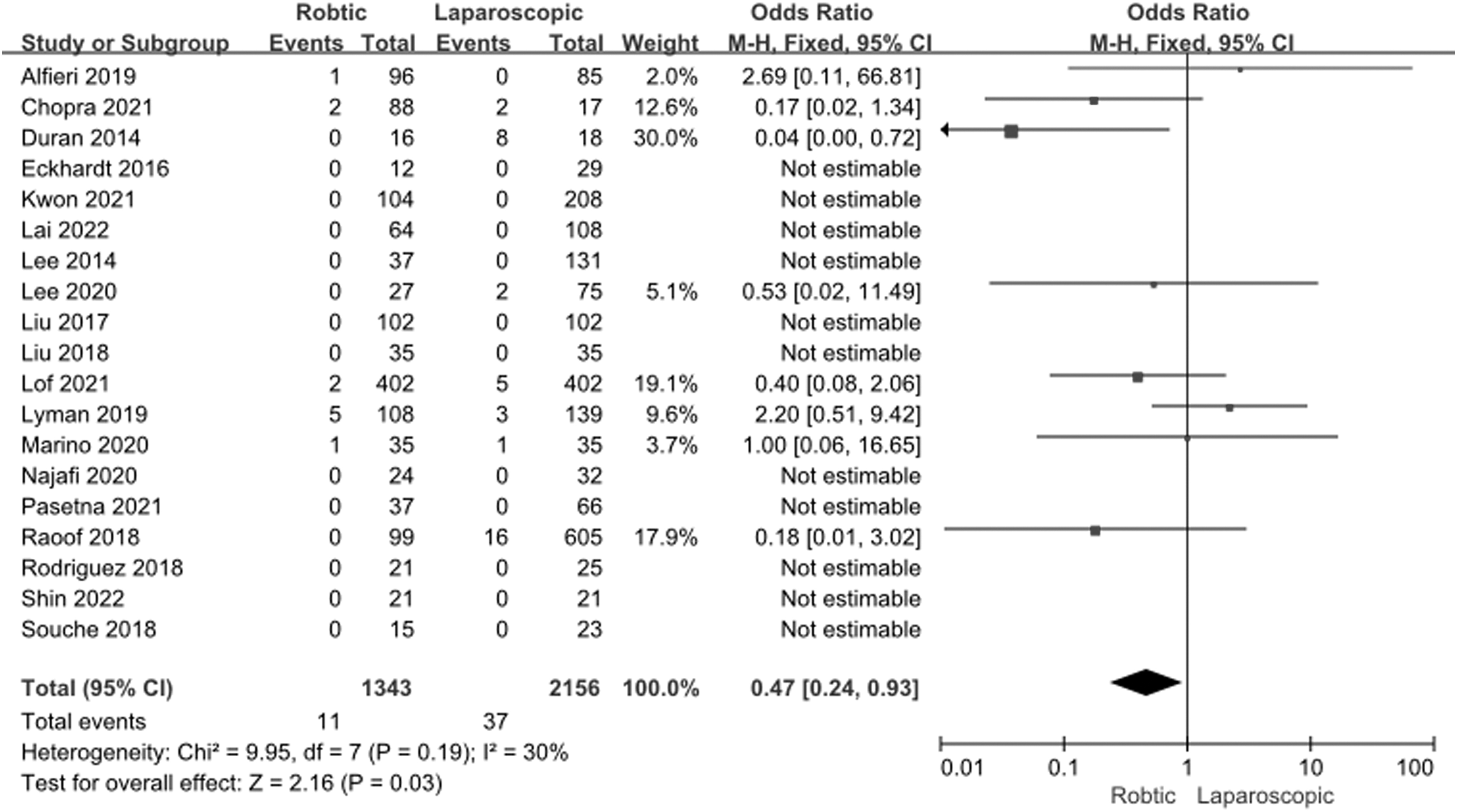
Fixed-effect statistical model of OR for 90-day mortality after RDP versus LDP. LDP, laparoscopic distal pancreatectomy; OR, odds ratio; RDP, robotic distal pancreatectomy.
R0 resection rate
There were 13 studies about analyzing R0 resection rate (Supplementary Fig. S1). Heterogeneity test (Chi-square statistics) among studies did not show difference (P = .16). A fixed-effect model was used. There was no statistical difference in R0 resection rate between the RDP and LDP groups with a combined OR of 1.11 (95% CI: 0.78 to 1.57; P = .56)
Lymph node yield
There were six studies about analyzing lymph node yield (Supplementary Fig. S2). Heterogeneity test among studies did not show difference (P = .80). A fixed-effect model was performed. There was no statistical difference in lymph node yield between the two groups with a combined OR of 0.76 (95% CI: −0.57 to 2.10; P = .26).
Postoperative hospital stay
There were 23 studies about analyzing postoperative hospital stay (Supplementary Fig. S3). Heterogeneity test among studies showed statistical differences (P < .00001). A random-effect model was performed. There was no statistical difference in postoperative hospital stay between the two groups with a combined OR of −0.54 (95% CI: −1.07 to −0.00; P = .05).
Operation cost
There were four studies about analyzing operation cost (Supplementary Fig. S4). Heterogeneity test among studies showed statistical differences (P < .00001). A random-effect model was performed. Operation cost in the RDP group was more than that in the LDP group with a combined OR of 3059.16 (95% CI: 857.27 to 5261.04; P = .006).
Total cost
There were seven studies about analyzing total cost (Supplementary Fig. S5). Heterogeneity test among studies showed statistical differences (P < .00001). A random-effect model was used. Total cost in the RDP group was more than that in the LDP group with a combined OR of 3647.28 (95% CI: 2332.70 to 4961.85; P < .00001).
Sensitivity analysis and publication bias
The data of R0 resection rate, lymph node yield, conversion to open surgery, spleen preservation rate, intraoperative blood loss, postoperative pancreatic fistula, operation cost, and total cost were analyzed using either fixed-effect or random-effect statistical models. The results were similar and the combined results were highly reliable. However, there were differences in postoperative hospital stay and 90-day mortality data between fixed- and random-effect statistical models. The results were not very reliable.
The funnel plot of Begg's test in R0 resection rate, lymph node yield, conversion to open surgery, spleen preservation rate, intraoperative blood loss, postoperative pancreatic fistula, postoperative hospital stay, and 90-day mortality showed symmetry. There was no publication bias in the study, which indicated that the results of the meta-analysis were statistically reliable. However, the funnel plot of Begg's test in operation cost and total cost did not show symmetry. There was publication bias in the study, which indicated that the results of the meta-analysis were not statistically reliable.
Discussion
LDP was first reported by Cuschieri in 1994, while RDP was first reported by Melvin in 2003.45,46 They have developed rapidly in recent years and been made popular in minimally invasive pancreatic surgery. However, which one is safer and more feasible treatment to distal pancreatectomy is not absolutly confirmed.
As we all know, conversion to open surgery, blood loss, and 90-day mortality are used to evaluate minimally invasive surgery. RDP was developed to overcome the limitations of LDP. Conversion to open surgery and blood loss in the RDP group were both significantly less than that in the LDP group (P < .05).
There are several technical advantages in robotic surgery, as follows: (1) The enhanced dexterity of robotic arms and tremor filtration, (2) wide range endo-wrist movements or motion scaling, (3) the three-dimensional surgical view of the surgical site facilitates surgery in a narrow surgical space, (4) convenience in achieving suturing and hemostasis, and 5. the two lenses of the robot may play an important role. When bleeding contaminates one lens, surgeons can replace it with a second “eye” to quickly stop the bleeding and avoid undergoing a laparotomy due to excessive bleeding. And 90-day mortality in the RDP group was also significantly less than that in the LDP group (P < .05). This can be explained by precise intraoperation manipulation and adequate hemostasis in robotic surgery.
Lymph nodes harvested, R0 resection rate, and postoperative pancreatic fistula showed no difference between the two groups (P > .05). These factors showed that RDP is better than LDP in safety. The data of postoperative hospital stay and 90-day mortality were both different between the fixed- and random-effect statistical model. The results were not highly reliable.
It is uncertain which group has an advantage in postoperative hospital stay. Meanwhile, the funnel plot of Begg's test in operation cost and total cost did not exhibit symmetry. There was publication bias in the study, which indicated that the results of the meta-analysis about operation cost and total cost were not statistically reliable. Operation cost and total cost in the RDP group were both more than that in the LDP group(P < .05). The cost of RDP limited the widespread use of RDP. With the development and modernization of robot technology, the cost can be reduced.
This study included 38 studies to compare RDP and LDP. However, there are still several limitations to our study. First, our study included retrospective studies and caused selection biases. Second, a short follow-up period of included studies cannot assess long-term outcomes. Third, the studies had benign or malignant lesions,which may affect the prognosis. Finally, only search for English academic journals in the database of Medline, EMBASE, or PubMed.
Conclusion
RDP and LDP were indeed worth comparing in clinical practice. However, it may be difficult to determine which is absolute advantage according to current data. Prospective randomized controlled trial with large sample and reliable methodology could take into account the current limitations and are needed to confirm which is better treatment.
Footnotes
Authors' Contributions
Contributed to the conception of the study: J.L. Made significant contribution to article preparation: J.L. and J.Y. Conducted statistical analysis and wrote the artical: J.L. Assisted in analysis through constructive discussionstomng: J.L., J.Y., J.Z., Y.W., G.S., C.L., and Z.D.
Ethical Approval
This study has obtained a PROSPERO (registration) ID “CRD4202345576,” without the approval of the ethics committee.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.