
Abstract
Background:
Inflammatory bowel disease (IBD) affects all ages and backgrounds, and many individuals require surgical intervention during their disease course. The adoption of laparoscopic techniques in this patient population has been slow, including intracorporeal anastomosis (ICA). The aim of our study was to determine if ICA was feasible and safe in patients with IBD undergoing laparoscopic right hemicolectomy (LRHC).
Methods:
This is a retrospective, single institution cohort study of elective and emergent cases of LRHC at a single academic center. Patients included underwent LRHC or ileocolic resection for IBD. Exclusion criteria: conversion to laparotomy, resection without anastomosis, or unconfirmed diagnosis of IBD. Main outcomes studied were anastomotic leak rate, surgical site infection (SSI), postoperative length of stay, 30-day readmission/reoperation, and operative time. Secondary outcomes were incisional hernia rates and rates of disease recurrence.
Results:
A total of 70 patients were included, 12 underwent ICA and 58 extracorporeal anastomosis. Anastomotic leak rate (intracorporeal 8.3% [n = 1], extracorporeal 8.6% [n = 5], P = .97), and SSI rates (intracorporeal 0%, extracorporeal 6.9% [n = 4], P = .36) were similar. Mean postoperative length of stay, rates of 30-day readmission/reoperation and diagnosis of hernia at 1 year were not significantly different. Rates of IBD recurrence and location of recurrence at 1 year were similar. However, operative time was significantly longer in those undergoing ICA (intracorporeal 187 minutes versus extracorporeal 139 minutes, P = < .05).
Conclusions:
ICA is a safe option in patients with IBD undergoing LRHC.
Introduction
Inflammatory bowel disease (IBD) is a chronic disease of the gastrointestinal tract, encompassing both Crohn's disease and ulcerative colitis. North America has the highest prevalence of IBD in the world, with nearly one quarter of all the patients living with IBD residing within the United States of America.1,2 Unfortunately, the prevalence continues to increase. 2 Many of these patients will require surgical intervention during their disease course which contributes to the large health burden that IBD presents.1,2
Due to the complex nature of the interventions required, previously all interventions were performed via laparotomy. However, multiple randomized trials in the early 2000s demonstrated the safety and noninferiority of laparoscopic colon resections.3–8 These studies demonstrated significantly improved morbidity, decreased length of stay, quicker return of bowel function, and decreased analgesia requirements.4,6,8 Intracorporeal anastomosis (ICA) has shown further improvements in patient outcomes, with shorter hospital stays and decreased incisional hernia rates.9–14 The uptake of laparoscopic techniques and ICA has been slow in the IBD population, and research is limited. 15 Specifically in the IBD population, ICA has been shown to significantly reduce incisional hernia rates. 16
The aim of our study was to evaluate the feasibility and safety of ICA in IBD patients undergoing laparoscopic right hemicolectomy (LRHC) or ileocolic resection (ICR) in comparison to extracorporeal anastomosis (ECA).
Materials and Methods
This study has been approved by the Health Science Research Ethics Board at the University of Western Ontario. The STROBE checklist was utilized to ensure completeness of reporting. 17 A single institution, retrospective cohort study was carried out between January 2012 and July 2022. Patients eligible to be included in the study were those undergoing LRHC or ICR and were identified using a hospital database, as well as surgeon office databases. All patients underwent resection at London Health Sciences Centre (University Hospital and Victoria Hospital) in London, Canada.
LRHC was defined as mobilization and resection of the ascending colon including the hepatic flexure. Laparoscopic ICR was defined as mobilization and resection of the terminal ileum and ascending colon, but the hepatic flexure was left in place. Patients were divided into two groups, according to the type of anastomosis, intracorporeal versus extracorporeal. ICA was defined as a totally LRHC or ICR and anastomosis, with the only nonport site incision made for extraction. ECA was defined as laparoscopic-assisted right hemicolectomy or ICR where the anastomosis was created after exteriorizing the bowel through the extraction incision. Inclusion criteria for the study were those patients over the age of 18 that underwent LRHC or ICR for IBD. Both elective and emergent cases were included. Exclusion criteria were patients who underwent laparotomy (intraoperative conversion), or resection without anastomosis.
Electronic charts of all patients deemed to be eligible according to the inclusion criteria were reviewed, and the required data was extracted and recorded. Patient demographic data were obtained to ensure that groups were similar with respect to age, biological sex, body mass index (BMI), American Society of Anesthesiologists (ASA) score, smoking status (including marijuana), IBD subtype (Crohn's disease, ulcerative colitis), and current IBD medication class (steroids, aminosalicylates, immunomodulators, and biologics) and number. Procedure-related data collected included operation completed, type of anastomosis, operative time, preoperative diagnosis, urgency of intervention (elective versus emergent), and extraction site. Operative time was calculated based on time from first skin incision to skin closure.
Morbidity data collected included postoperative hospital length of stay (calculated from day of surgery to day of discharge), anastomotic leak rate, rate of surgical site infection (SSI), 30-day readmission/reoperation and incisional hernia rate at 1 year. Presence of anastomotic leak and SSI was determined by chart review. IBD recurrence rates at 1 year were evaluated, as well as if the recurrence occurred at the site of anastomosis.
Analysis of the two groups was undertaken using a two-sided unpaired t-test to assess for differences between those undergoing ICA and ECA, with a 95% confidence interval.
Results
Patient demographics
A total of 70 patients underwent LRHC or ICR between January 2012 and July 2022 at our institution and met inclusion criteria (Fig. 1). Of the 70 patients, 12 (17.1%) patients underwent ICA and 58 (82.9%) underwent ECA. Patient demographics and smoking status were similar between the two groups (Table 1). Number and type of IBD specific medications were also similar (Table 2). There were a significantly higher number of patients in the ICA group treated with medications classified as biologics at the time of operative intervention.
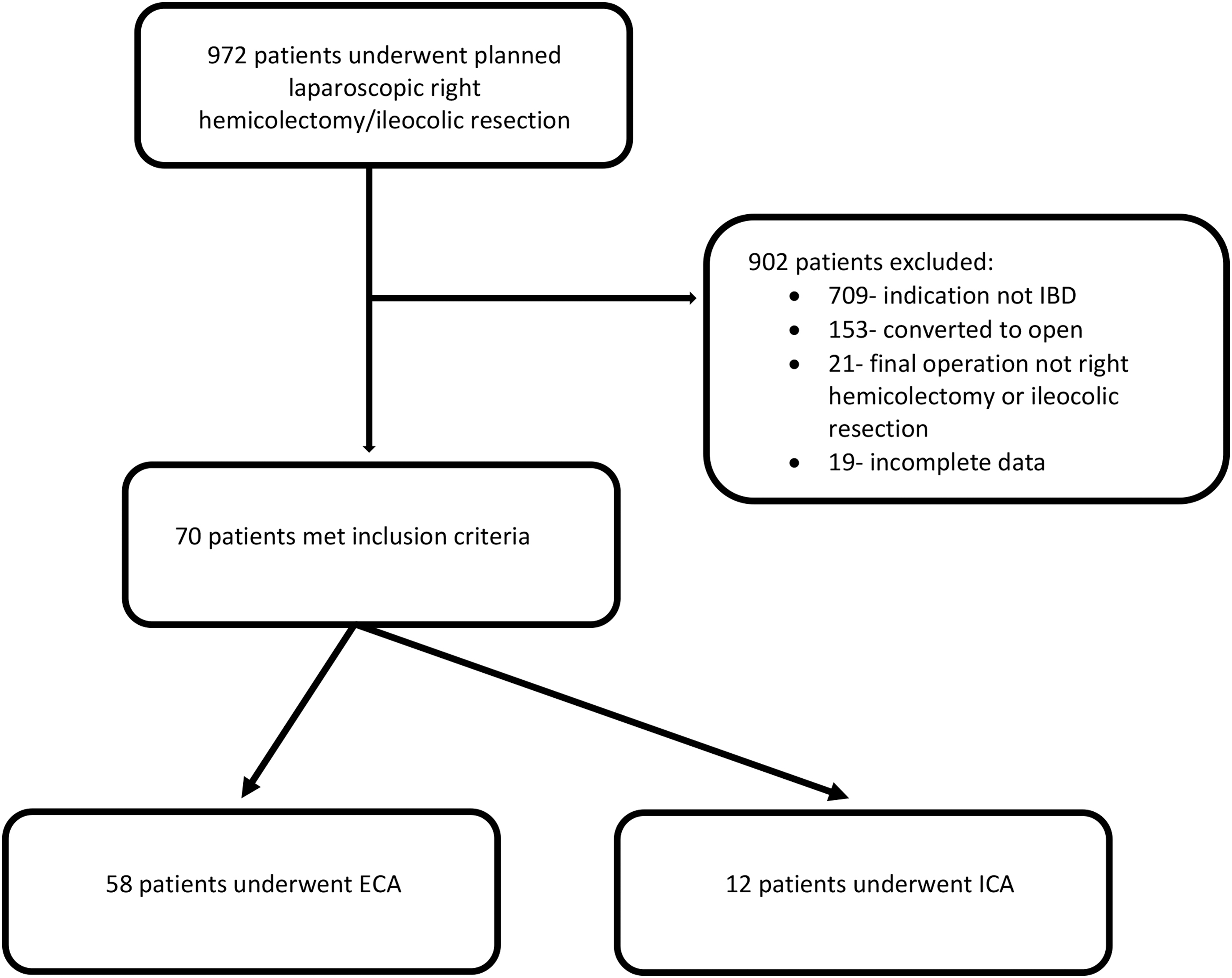
Flow diagram demonstrating patients included in the study/analyzed and those excluded at each stage.
Patient Demographics and Smoking Status
ASA, American Society of Anesthesiologists; BMI, body mass index; ECA, extracorporeal anastomosis; ICA, intracorporeal anastomosis; n/a, not applicable.
Number and Class of Inflammatory Bowel Disease Specific Medications
ECA, extracorporeal anastomosis; IBD, inflammatory bowel disease; ICA, intracorporeal anastomosis.
Operative indications and time
Indications for operative intervention are indicated in Table 3 and are similar between the two groups. LRHC was significantly more frequent in the ICA group, while ICR was more common in the ECA group (LRHC: ICA- n = 11, ECA-n = 22, P value .0005) (ICR: ICA-n = 1, ECA- n = 36, P value .0005). Operative time was longer in the ICA group by an average of 49 minutes (ICA: 188 ± 63 minutes, ECA: 139 ± 42 minutes; P-value: .001). Location of extraction incision was different between the two groups, with the majority of those in the ICA undergoing Pfannenstiel extraction, while those in the ECA group were more likely to have a midline incision (Pfannenstiel: ICA-n = 11 [91.7%], ECA- n = 7 [12.1%]; P value <.00001) (Midline: ICA- n = 1 [8.3%], ECA- n = 47 [81.0%]; P value <.000001) (Other: ICA- n = 0 [0%], ECA- n = 4 [6.9%]; P value .86).
Reason and Urgency of Operative Intervention
ECA, extracorporeal anastomosis; ICA, intracorporeal anastomosis.
Length of stay and complication rate
Mean length of stay was similar between the two groups (ICA: 6.0 ± 2.7 days, ECA: 5.0 ± 2.7; P value .34). SSI rates and rates of anastomotic leak were similar between both groups (SSI: ICA-n = 0 [0%], ECA- n = 4 [6.9%]; P value .36) (Anastomotic Leak: ICA- n = 1 [8.3%], ECA- n = 5 [8.6%]; P value .97). Wound class for all cases was documented as class 2 in both the ICA and the ECA group. In the ICA group, all anastomoses were performed in a side-to-side stapled fashion, with the common enterotomy closed with suture (either barbed suture or vicryl suture) in two layers. In the ECA group, all anastomoses were constructed in a side-to-side stapled fashion utilizing standard Barcelona technique. There was no difference among both groups with regards to use of techniques known to decrease SSI rates (Table 4). As well, all patients received perioperative prophylactic antibiotics as per protocol. Rates of 30-day readmission and reoperation, as well as rate of incisional hernia at 1 year were not statistically different (Table 5).
Interventions Employed to Decrease Surgical Site Infection Risk
ECA, extracorporeal anastomosis; ICA, intracorporeal anastomosis.
Thirty-Day Readmission/Re-Operation Rates and Incisional Hernia Rates
ECA, extracorporeal anastomosis; ICA, intracorporeal anastomosis.
Recurrence rates
There was no statistically significant difference in recurrence rates in the two groups; however, there was a strong trend toward decreased recurrence rates in the ICA group (ICA: n = 3 [25%], ECA: n = 29 [50%]; P value .12). The vast majority of patients experiencing disease recurrence in both the ICA and ECA groups occurred at the site of anastomosis (ICA: n = 3 [100%], ECA: n = 26 [89.7%]; P value .57).
Discussion
This study is a single institution, retrospective cohort study evaluating patients with IBD undergoing LRHC or ICR. The objective of this study was to evaluate the safety and feasibility of ICA in this patient population. The three key findings or this study are that there were similar rates of readmission or reoperation at 30 days, no difference in SSI or anastomotic leak rates, but a trend toward decreased disease recurrence in the ICA group.
The patient demographics in both groups were similar, and on average, patients had lower BMI than that of an average North American adult. 18 This discrepancy has been demonstrated in multiple studies, specifically with patients with Crohn's disease thought to be a surrogate of an element of malnutrition.19,20 Our patient population was slightly female predominant, consistent with the female predominance of autoimmune conditions including IBD. 1 Given that IBD tends to present at between 18 and 35 years of age and the required time to develop complications requiring operative intervention, the mean age of patients in our study (ICA: 38, ECA: 40) is appropriate.21,22
The vast majority of patients in both groups had underlying diagnosis of Crohn's disease. This discrepancy is likely due to the underlying differences between the two subtypes of IBD. Crohn's disease can affect the entire gastrointestinal tract, and therefore, conservation of bowel is paramount to avoid devastating complications like short gut syndrome. 23 Complications like stricture or fistula are also isolated to Crohn's disease. 23 On the other hand, UC is isolated to the colon, and therefore, significant disease is dealt with by undertaking a total colectomy. 24
A large proportion of patients in our study were active smokers (either tobacco or marijuana) at the time of their surgical intervention. Previous studies have demonstrated that patients with Crohn's disease who are active smokers tend to have higher rates of complications and higher rates of penetrating or stricturing disease.25,26 In fact, there were a higher percentage (although it did not meet significance) of smokers in the ICA group, along with significantly more patients on biologic therapy. This is in keeping with the evidence that Crohn's patients whom are smokers tend to have more significant disease complications.25,26
Patients undergoing ICA in our study had longer operative times than those undergoing ECA. Longer operative times has been associated with ICA in many previous studies.11–13,27,28 However, operative time has also shown to decrease as surgeon's experience with ICA increases. 12 The results in our study may be confounded by the disproportionate number of LRHC observed in the ICA group compared to the ECA group. Trainee involvement in cases is also likely to increase operative time given that all cases were conducted at designated teaching hospitals. Many trainees have minimal exposure to laparoscopic suturing before training with our minimally invasive surgery team, who conducted the vast majority of the ICA cases.
Furthermore, a study conducted by our group published in 2022 demonstrated that median operative time significantly decreased over time when comparing ICA to ECA in all patients undergoing LRHC at our institution. 12 They noted that the difference in operative was 70 minutes in 2015, but decreased to 35 minutes in 2020. 12 Therefore, with increased utilization of and familiarity of this technique, there is unlikely to be a significant difference in operative time. As well, due to the nature of academic teaching sites like ours, the resident turnover on services where they have access to fostering these skills is quick, and therefore, operative time for a technically proficient laparoscopic surgeon is likely to be very similar between the two techniques. Thus, as laparoscopic intracorporeal suturing becomes more common, operative times are sure to substantially decrease. This can best be facilitated by increased use of the technique by general surgeons. Ultimately, we also feel that even with an upfront increased operative time, ICA is justified due to the reduced need for postoperative narcotics and decreased rates of incisional hernia demonstrated in the literature.9,11–13
The anastomotic leak rate demonstrated in our study in both groups was slightly higher than the mean quoted in most recent studies.29–32 However, patients in both groups demonstrated several risk factors for development of an anastomotic leak, and previous studies have demonstrated higher rates in patients with IBD. 33 Multiple studies have demonstrated the increased risk of anastomotic leak with emergent operations, smokers, use of immunosuppressive medications (i.e., steroids), ASA class ≥2, and malnutrition.30,34,35 The effect of other IBD medications such as aminosalicylates, immunomodulators, and biologics is still highly debated.33,35–39
There were no statistical differences in SSI rates between the two groups. Both groups employed several techniques that have been shown to decrease SSI risk, including increased use of chlorhexidine skin prep, wound protector use, and use of absorbable suture for skin closure. As well, the low rates of SSI associated with ECA may be attributable to the use of the Barcelona technique coupled with the use of wound protector, as this ensures minimal spillage/contamination of the wound with enteric contents.
Previous studies have demonstrated decreased incisional hernia rates with ICA, including a previous study conducted by our group which demonstrated significantly reduced rates of incisional hernias at 2 years in patients undergoing right hemicolectomy for all indications.11,12 This study demonstrated a decrease in extraction site hernias from 7.1% in the ECA group, to 1.5% in the ICA group (P = .02). 12 It has been postulated that a reduction in incisional hernia rates with ICA is related to the avoidance of midline incisions by utilizing a Pfannenstiel incision for extraction. However, it is well known that the development of incisional hernias is multifactorial, including preoperative, intraoperative, and postoperative variables. Thus, it remains difficult to attribute decreased incisional hernia rates solely to one variable. Our current study failed to demonstrate a significant difference in incisional hernia rates at 1 year despite the use of a Pfannenstiel incision for most patients in the ICA group. Therefore, although in general ICA is associated with decreased incisional hernia rates, further data are needed to support this conclusion in the IBD population.
Disease recurrence in IBD can be exceptionally detrimental to patients, leading to additional surgical interventions, thus mitigating disease recurrence is vital. There was no difference in recurrence between the two types of anastomoses evaluated in our study; however, there was a strong trend toward decreased recurrence in the ICA group. Previous studies have suggested that a stapled side-to-side anastomosis is favored compared to end-to-side and end-to-end.33,35 However, more recently the “Kono-S” technique has been shown to potentially decrease recurrence rates in small trials.35,40 The optimal type of anastomosis has yet to be elucidated and further studies should be done comparing these various methods employing Minimally Invasive Surgery (MIS) techniques.
This study does have its limitations. Given the retrospective nature of the study, events not captured within the electronic medical record may not have been accounted for. Further, long-term outcomes, including need for repeat operative intervention or development of incisional hernia beyond 1 year, were not assessed in this study.
The main criticism of ICA has been the increased operative time. However, with improved resident access to minimally invasive techniques and dedicated laparoscopic suturing simulation curriculums, operative time will improve and lead to increased utilization. Future studies should continue to evaluate MIS anastomotic techniques in patients with IBD to determine the optimal technique to decrease recurrence rates and facilitate future interventions if required.
Conclusion
In conclusion, ICA is a very feasible and safe approach in patients with IBD undergoing LRHC/ICR. ICA leads to comparative outcomes to ECA, with smaller extraction incisions which may lead to decreased incisional hernia rates, although it is associated with longer operative times. However, further work needs to be done to determine optimal anastomotic technique to reduce IBD recurrence.
Footnotes
Authors' Contributions
K.M.: Conceptualization (equal), methodology (equal), investigation (lead), data curation (lead), formal analysis (lead), writing-original draft (lead), writing—review and editing (equal), visualization (lead). C.M.S.: Conceptualization (equal), methodology (equal), writing—review and editing (equal), visualization (supporting), supervision (equal). J.H.: Conceptualization (equal), methodology (equal), writing—review and editing (equal). A.E.: Conceptualization (equal), methodology (equal), writing—review and editing (equal). N.A.A.: Conceptualization (equal), methodology (equal), writing—review and editing (equal), visualization (supporting), supervision (equal), project administration (lead).
Disclosure Statement
C.M.S. is a consultant for Ethicon, Canada. N.A.A. is on the editorial board for the Journal of Laparoendoscopic & Advanced Surgical Techniques and Videoscopy. The remainder of the authors have no conflicts of interests to declare.
Funding Information
No funding was received for this article.