
Abstract
Background:
Minimally invasive surgery has been demonstrated to have clear advantages in colon cancer management, with a decrease in the morbidity and mortality associated with surgery. With the introduction of intracorporeal anastomosis (ICA), the entire mesenteric dissection and division is performed under vision laparoscopically and may lead to superior lymph node harvest. The aim of our study is to evaluate lymph node harvest in patients undergoing totally laparoscopic right hemicolectomy with ICA compared to laparoscopic-assisted right hemicolectomy with extracorporeal anastomosis (ECA).
Methods:
This is a single institution retrospective cohort study. Eligible patients underwent laparoscopic right hemicolectomy at our institution between 2012 and 2022. Patients were identified using a hospital database, and surgeon office databases. Patients included underwent laparoscopic right hemicolectomy for neoplastic lesions (colon cancer/unresectable polyps), or benign etiologies. We excluded patients who underwent laparotomy (intra-operative conversion), resection without anastomosis, resection for IBD, or lack of documented lymph node number. Data were compared using two-sided t-test evaluation with a 95% confidence interval.
Results:
A total of 679 patients were included, 493 ECA (72.6%) and 186 ICA (27.4%). Patient demographics (age, biologic sex, American Society of Anesthesiologists and body mass index) were not significantly different. Lymph node harvest was significantly higher in those with ICA (24 ± 14 versus 21 ± 1, P < .05). In subgroup analysis, this difference was maintained in patients with malignant processes (27 ± 14 versus 23 ± 10, P < .05).
Conclusions:
In our experience, ICA has higher lymph node harvest in comparison to ECA. This may improve outcomes and options for adjuvant therapies in malignant indications.
Introduction
Colon cancer is the fourth most commonly diagnosed cancer in Canada, with an estimated 67 new patients diagnosed every day. 1 The initial treatment for almost all patients with colon cancer is surgical resection, which has associated rates of morbidity and mortality. Previously, the standard of care was resection via laparotomy. The safety and noninferiority of laparoscopic-assisted colon resections was proven through multiple randomized trials in the early 2000s.2–7 These studies demonstrated decreased morbidity, length of stay, decreased analgesia requirements, and quicker return of bowel function.3,5,7
Further improvements in patient outcomes have been shown with the development of intracorporeal anastomosis (ICA). These improvements include decreased conversion rates, decreased time to return of bowel function, shorter hospital stay, and decreased incisional hernia rates.8–13 Unfortunately, the uptake of this technique has been slow, due to increased operative time and technical skills required. A recent survey done in collaboration with the Research Institute Against Digestive Cancer (IRCAD), found that only 31.4% of respondents frequently perform ICA. 14
The aim of our study is to evaluate the extent of lymph node harvest in patients undergoing totally laparoscopic right hemicolectomy with ICA compared to those undergoing laparoscopic-assisted right hemicolectomy with extracorporeal anastomosis (ECA).
Materials and Methods
This study was approved by the Health Science Research Ethics Board at the University of Western Ontario.
The STROBE checklist was utilized to ensure completeness of reporting. 15 A single institution, retrospective cohort study was carried out between January 2012 and July 2022. Patients eligible to be included in the study were those undergoing laparoscopic right hemicolectomy and were identified using a hospital database, as well as surgeon office databases. All patients underwent resection at London Health Sciences Centre (University Hospital and Victoria Hospital) in London, Canada.
Patients were divided into two groups, according to the type of anastomosis, intracorporeal versus extracorporeal. ICA was defined as a totally laparoscopic right hemicolectomy and anastomosis, with the only nonport site incision made for extraction. ECA was defined as laparoscopic-assisted right hemicolectomy where the anastomosis was created after exteriorizing the bowel through the extraction incision.
Inclusion criteria for the study were those patients older than the age of 18 years who underwent laparoscopic right hemicolectomy for neoplastic lesions (colon cancer/unresectable polyps), or benign etiologies. Both elective and emergent cases were included. Exclusion criteria were patients who underwent laparotomy (intraoperative conversion), resection without anastomosis, resection for IBD, or lack of reported lymph node yield in the pathology report.
Electronic charts of all patients deemed to be eligible according to the inclusion criteria were reviewed and the required data were extracted and recorded. Patient demographic data were obtained to ensure that groups were similar with respect to age, biological sex, body mass index (BMI), and American Society of Anesthesiologists (ASA) score. Procedure related data collected included type of anastomosis, operative time, and preoperative diagnosis. Operative time was calculated based on time from first skin incision to skin closure. Lymph node count and final diagnosis was obtained from the pathology report.
Morbidity data collected included postoperative hospital length of stay (calculated from day of surgery to day of discharge), anastomotic leak rate, and rate of surgical site infection (SSI). Presence of anastomotic leak and SSI were determined by chart review. Oncologic outcomes collected included nodal upstaging, implementation of chemotherapy, completion of adjuvant chemotherapy, chemotherapy-associated complications, rate of cancer recurrence, and 1, 3, and 5 year survival.
Analysis of the two groups was undertaken using a two-sided unpaired t-test to assess for differences between those undergoing ICA and ECA, with a 95% confidence interval. Subgroup analysis was also done comparing patients with underlying malignant processes (ICA versus ECA), as well as those with benign etiologies (ICA versus ECA).
Results
Patient demographics
A total of 679 patients underwent right hemicolectomy between January 2012 and July 2022 at our institution and met inclusion criteria (Fig. 1). Of the 679 patients, 493 patients had ECA (72.6%) and 186 had ICA (27.4%). Patient demographics were similar between the two groups (Table 1).
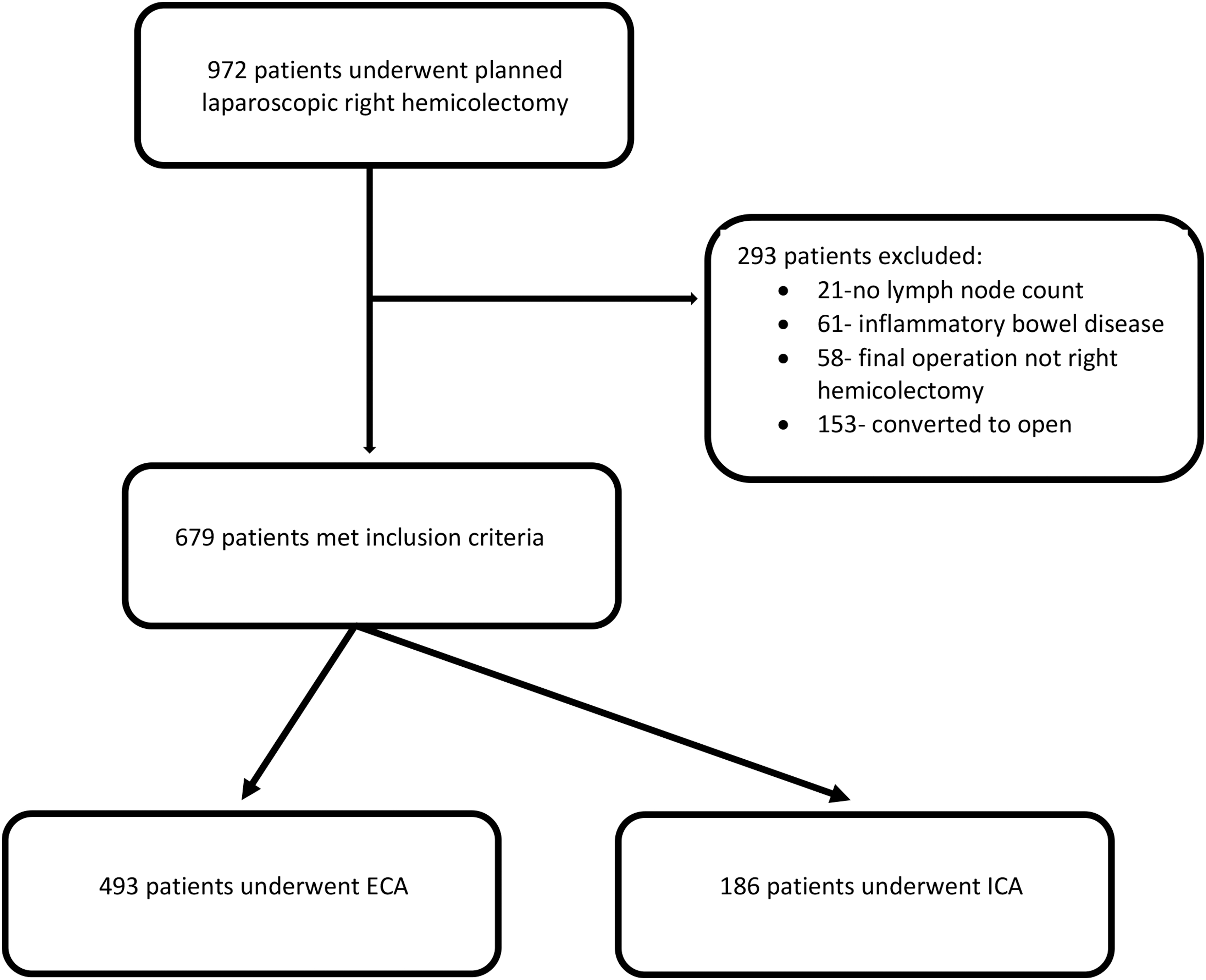
Schematic depiction of patient eligibility for study inclusion.
Patient Demographics
ASA, American Society of Anesthesiologists; BMI, body mass index; ECA, extracorporeal anastomosis; ICA, intracorporeal anastomosis.
Operative indications and time
There was a total of 21 surgeons included in our study, of these surgeons, only 7 were involved in the ICA group. Four fellowship trained, minimally invasive surgeons accounted for 97% of the ICA operations. Indications for operative intervention are indicated in Table 2 and are similar between the two groups. The mean operative time was significantly longer in patients undergoing ICA by an average of 48 minutes (ICA 192 ± 52 minutes versus ECA 144 ± 46 minutes, P < .05). This difference was maintained regardless of the indication for operation (Malignant: ICA 193 ± 53 minutes versus ECA 144 ± 47 minutes, P < .05) (Benign: ICA 191 ± 50 minutes versus ECA 144 ± 42 minutes, P < .05).
Indication for Operative Intervention
ECA, extracorporeal anastomosis; ICA, intracorporeal anastomosis; NET, neuroendocrine tumor.
Length of stay and complication rate
Length of stay was significantly shorter for ICA when isolating for malignant indications (ICA 4.7 ± 4.2 days versus ECA 5.8 ± 5.4 days, P < .05), but not different when all indications were grouped (ICA 4.7 ± 3.9 days versus ECA 5.6 ± 5.2 days, P = .06). Rates of SSI and anastomotic leak were similar between the two groups (Anastomotic leak: ICA n = 4 (2%) versus ECA n = 20 (4%), P = .23) (SSI: ICA n = 9 (5%) versus ECA n = 35 (7%), P = .29)
Lymph node harvest
Patients undergoing ICA had significantly more lymph nodes collected, with a mean of 24 ± 14 nodes compared to 21 ± 11 nodes in those undergoing ECA (P = .004). This difference was maintained when isolated for patients undergoing resection for malignant indications (ICA 27 ± 14 nodes versus ECA 23 ± 10 nodes, P = .003), but not for benign cases (ICA 14 ± 10 nodes versus ECA 12 ± 8 nodes, P = .32). In patients who had their right hemicolectomy for malignant indications, the adequacy of lymph node harvest, defined by at least 12 lymph nodes collected, was equivalent between the two groups (ICA n = 140 (99%) versus ECA n = 359 (96%), P = .11).
Oncologic outcomes
Oncologic outcomes were similar between the two groups (Table 3). There was no difference in nodal upstaging of specimens, number of patients who received/completed adjuvant chemotherapy or rates of chemotherapy-related complications (Table 3). The overall rates of cancer recurrence and overall survival were also similar between the two groups (Table 3).
Oncologic Outcomes
ECA, extracorporeal anastomosis; ICA, intracorporeal anastomosis.
Discussion
This study is a retrospective, single institution, cohort study, evaluating patients undergoing laparoscopic right hemicolectomy, with the objective of evaluating differences in lymph node harvest between ICA and ECA. The two key findings of this study are that both techniques have similar safety profiles, and ICA is associated with higher lymph node retrieval.
Both groups had very similar demographics and are comparable to the general North American population. The average BMI for men is 29.1 and 29.6 for women, which is very similar to our patient population. 16 Our patient age is also consistent with the average age of diagnosis of colorectal cancer in North America (68 in men, 72 in women). 17 Therefore, the patient population evaluated in this study is representative of the North American population.
Several previous studies have demonstrated that ICA leads to longer operative times, which was replicated here in this study.10–12,18,19 However, our previous report has shown that operative time for ICA decreases with surgeon experience. 11 In this study, the increased length of operative time may be confounded by trainee involvement in cases, as this study was conducted at an academic institution. Many trainees often have minimal prior exposure to laparoscopic suturing before their training with the MIS surgeons who performed the vast majority of the ICA cases. We feel that the increased operative time is justified by the reduced postoperative opioid use and reduced rates of reintervention for incisional hernia.8,10,11,20
All cancer-related specimens were examined by specialized GI pathologists utilizing established protocols to evaluate for number of lymph nodes, and positive lymph node number. Although minor difference in technique between pathologists may occur, there appears to be an even distribution of pathologists between the ICA and ECA group for malignant cases. Lymph node harvest was significantly higher in the ICA group in this study. This is likely due to better visualization of the colonic mesentery and ability to complete a complete mesocolic excision (CME) when completing ICA.
In our study, when the ECA was completed, the mesentery was often ligated after exteriorizing the bowel for anastomosis. Due to this, the mesentery is generally divided closer to the bowel due to reduced visualization of the vascular pedicle, and thus an incomplete CME was more likely obtained. Overall, the increase lymph node yield achieved in patients undergoing ICA is likely secondary to achieving a CME in these patients, compared to their ECA counterparts.
The oncologic adequacy, defined as at least 12 lymph nodes, was equivalent between the two groups. This has been shown in several previous studies that demonstrated similar oncologic outcomes and lymph node harvest between ICA and ECA.9,11,18,20–23 The standard metric for oncologic adequacy is currently at least 12 lymph nodes, but evidence suggests that the number of lymph nodes in a surgical specimen is an independent prognostic factor for survival in colon cancer.24–27 A recent retrospective study has shown that a lymph node yield of at least 22 nodes may improve overall survival and disease-free survival. 28 This was found to be especially applicable to right sided colon cancers. 28 This raises the possibility that improved lymph node yield may be beneficial for long-term oncologic outcomes. This is another possible benefit of ICA over ECA that will be evaluated in future analyses.
Overall, oncologic outcomes evaluated in our study were similar between the two groups despite an average increase in lymph node yield in the ICA group. This provides further data that ICA is a safe and effective option in patients with colorectal malignancies. This is, however, contrary to a recent retrospective study which demonstrated that a lymph node yield of at least 22 nodes led to improved overall survival and disease-free survival. However, our study is limited by its retrospective nature, and thus further research needs to be done to further evaluate the potential oncologic benefits of a higher lymph node yield in colorectal cancer.
Although our study did not evaluate rates of incisional hernia, a study conducted by our group published in 2022, demonstrated significantly reduced rates of incisional hernia at 2 years in patients undergoing right hemicolectomy with ICA. They demonstrated a decrease in extraction site hernias from 7.1% in the ECA group to 1.5% in the ICA group (P = .02). 11 Therefore, decreased incisional hernia rates appear to be a benefit of ICA over ECA.
This study has limitations, primarily, it is a retrospective analysis which utilized a review of electronic medical records to obtain certain outcomes (i.e., complication rate/SSI) and therefore events occurring outside the region may not have been captured. This study also did not assess long-term outcomes. A randomized control trial would provide improved confidence in the data. Further, it has yet to be elucidated in the literature the optimal number of lymph nodes needed to improve long-term patient outcomes. We believe that more lymph nodes obtained lead to more accurate staging and thus likely better outcomes.
Future studies should be done to determine the long-term benefits of higher lymph node harvest in patients with colon cancer. Moving forward, we feel that increased access to training in ICA through residency training programs is necessary to increase surgeon comfort with this approach and increase uptake. This can be facilitated through the implementation of dedicated laparoscopic suturing simulation tasks incorporated into training programs.
Conclusion
In conclusion, ICA is a safe approach for a laparoscopic right hemicolectomy for both benign and malignant indications. ICA leads to increased lymph node harvest, which may lead to improved oncologic outcomes. However, further work needs to be done to determine the optimal number of lymph nodes needed. Increased opportunities for trainees to become more comfortable and adept at ICA are needed, which in turn will lead to decreased operative time and further improvements in patient outcomes.
Footnotes
Acknowledgments
The authors acknowledge Dr. Jordan Levy and Dr. Sydney Selznick for their work on examining the effect of ICA versus ECA on postoperative incisional hernia rates in patients undergoing laparoscopic right colectomies at our institution.
Authors' Contributions
K.M.: conceptualization (equal), methodology (equal), investigation (lead), data curation (lead), formal analysis (lead), writing—original draft (lead), writing—review and editing (equal), and visualization (lead). C.M.S.: conceptualization (equal), methodology (equal), writing—review and editing (equal), visualization (supporting), and supervision (equal). J.H.: conceptualization (equal), methodology (equal), and writing—review and editing (equal). A.E.: conceptualization (equal), methodology (equal), and writing—review and editing (equal). N.A.A.: conceptualization (equal), methodology (equal), writing—review and editing (equal), visualization (supporting), supervision (equal), and project administration (lead).
Disclosure Statement
C.M.S. is a consultant for Ethicon, Canada. N.A.A. is on the editorial board for the Journal of Laparoendoscopic and Advanced Surgical Techniques. K.M., J.H.,, and A.E. have no conflicts of interest to declare.
Funding Information
No funding was received for this article.