
Abstract
Background:
Intracorporeal esophagojejunostomy (EJ) in the context of laparoscopic total gastrectomy remains a complex and technically demanding procedure. We have previously introduced a novel method of intracorporeal circular stapled EJ utilizing a conventional purse-string suture instrument. Since May 2018, we have refined this technique, and the aim of this study was to assess its safety and efficacy.
Methods:
Between May 2018 and June 2022, we enrolled 92 patients who underwent laparoscopic total gastrectomy with the modified intracorporeal reconstruction method. In addition, between March 2014 and June 2022, we enrolled 121 patients who underwent the procedure with the extracorporeal reconstruction method. We retrospectively collected and compared the clinical data of these 2 patient cohorts.
Results:
Intracorporeal reconstruction group experienced lower postoperative pain scores (2.7 ± 1.3 versus 4.5 ± 1.4, P = .032), reduced administration of analgesics (3.1 ± 2.2 versus 5.0 ± 3.5, P = .041), and shorter postoperative hospital stays (4.9 ± 2.3 versus 6.3 ± 3.5, P = .045) compared with the extracorporeal reconstruction group. In addition, anastomotic time and postoperative pain score were not increased in the overweight patients in the intracorporeal reconstruction group. Anastomotic leakage occurred in 2 (2.2%) patients in the intracorporeal reconstruction group and 4 (3.3%) patients in the extracorporeal reconstruction group. Anastomotic stricture occurred in 1 (1.1% and 0.8%) patient in each group. There was no significant difference in the overall postoperative complication rate between the 2 groups.
Conclusions:
The modified intracorporeal purse-string stapling technique for EJ during laparoscopic total gastrectomy is a safe and viable option, exhibiting less invasiveness and comparable outcomes to the extracorporeal reconstruction method, especially suitable for obese patients.
Introduction
Laparoscopic gastrectomy for gastric cancer has gained increasing acceptance in recent years owing to its surgical and pathological outcomes that are comparable, or even superior, with those of open surgery.1–3 Nevertheless, alimentary reconstruction following laparoscopic gastrectomy remains a subject of debate, particularly regarding esophagojejunostomy (EJ) reconstruction after laparoscopic total gastrectomy. 4 Intracorporeal EJ continues to be a complex and technically challenging procedure, leading some surgeons to opt for laparoscopically assisted total gastrectomy with extracorporeal EJ anastomosis via mini-laparotomy. However, mini-laparotomy may diminish the advantages of a laparoscopic approach. In addition, the surgical space created by mini-laparotomy is often insufficient for anvil insertion and instrument manipulation. The length of the mini-laparotomy incision may also be influenced by the patient's body habitus and may necessitate further extension in obese individuals.
We previously introduced a novel method of intracorporeal circular stapled EJ using a conventional purse-string suture instrument (PSI) during laparoscopic total gastrectomy and demonstrated the safety and feasibility of this approach in an initial cohort of 45 consecutive patients with gastric cancer. 5 Since May 2018, we have refined this technique to enhance its ease of execution and have implemented it in 92 consecutive patients with gastric cancer. The aim of this study was to present our modified purse-string stapling technique for intracorporeal EJ and compare it with extracorporeal EJ via mini-laparotomy during laparoscopic total gastrectomy in patients with gastric cancer.
Methods
Patients
Between March 2014 and June 2022, a total of 293 patients with diagnosed gastric cancer in the middle or upper stomach underwent total gastrectomy at our institution. This study included 92 patients who underwent intracorporeal circular stapled EJ using an improved purse-string stapling technique and 121 patients who underwent extracorporeal circular stapled EJ via mini-laparotomy. The inclusion criteria were as follows: histologically confirmed gastric adenocarcinoma, clinical stage I–III, and esophageal invasion <2 cm above the cardia. The clinical data for these 2 patient groups were retrospectively collected and compared. Informed consent was obtained from each patient before surgery in all cases. The Institutional Review Board of Qingdao University approved this retrospective study.
Surgical Technique
Intracorporeal EJ using improved purse-string stapling technique
Intracorporeal purse-string suturing was performed utilizing a modified conventional PSI prepared preoperatively, as previously described. 5 In brief, a surgical glove was cut open at the thumb and pinkie, allowing the two hand shafts of the PSI to pass through separately and be sealed with a wire to maintain pneumoperitoneum (Fig. 1).
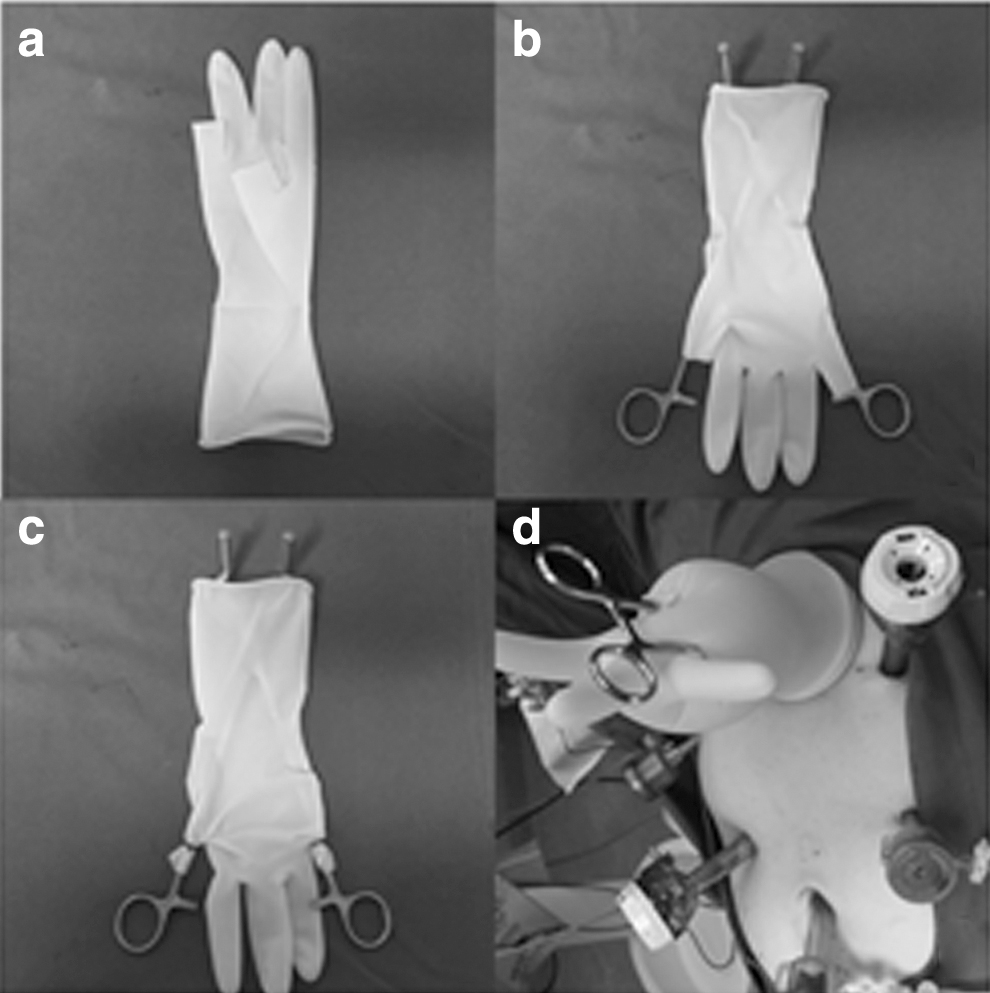
Surgical glove prepared for the PSI and attached to the wound retractor
Following the induction of general anesthesia, the patient was placed in a supine and slight reverse Trendelenburg position with legs parted. An umbilical port trocar was inserted using an open technique, and pneumoperitoneum was established. Subsequently, four additional ports were created in the upper abdomen. After radical lymphadenectomy and total mobilization of the stomach, the distal esophagus was ligated with a thick thread below the planned resection line. A 3-cm incision was made in the left midclavicular line and protected and retracted with a wound protector. The anvil of a 25-mm circular stapler (ECS; Ethicon Endo-Surgery) was introduced into the abdominal cavity. Next, the previously prepared surgical glove with PSI was attached to the wound retractor, and the distal esophagus was clamped with the PSI at the planned resection line (Fig. 2a).

Intracorporeal purse string suture and anvil insertion.
A purse-string suture with two straight needles was introduced into the abdominal cavity and passed through the PSI entrance hole under direct laparoscopic vision (Fig. 2b). The esophagus was then incised from the right wall just below the clamp line with an ultrasonic scalpel, preserving a small portion of the left wall to maintain self-traction and prevent retraction into the mediastinum during subsequent procedures (Fig. 2c). Following the removal of the PSI, the anvil head was gently inserted into the esophagus stump, and the purse-string suture was first tied with a surgical knot, followed by several additional knots to secure the anvil (Fig. 2d). The remaining left wall of the esophagus was then transected, completing total gastrectomy.
Reconstruction was performed using the Roux-en-Y method. The jejunojejunostomy was conducted intracorporeally, and the distal limb of the jejunum was brought up anteriorly to the colon. The previously prepared surgical glove with a circular stapler was attached to the wound retractor to maintain pneumoperitoneum after the body of the circular stapler was inserted into the distal limb of the jejunum, which was secured with an elastic tape to prevent slippage. Pneumoperitoneum was reestablished, and the tip of the circular stapler was introduced into the abdominal cavity and combined with the anvil head under laparoscopic vision. Finally, the jejunal stump was closed laparoscopically with a 45-mm endoscopic linear stapler (ETS45; Ethicon Endo-Surgery).
Circular stapled EJ through mini-laparotomy
After completing radical lymphadenectomy and total gastric mobilization, a 7- to 10-cm long mini-laparotomy was performed to reconstruct the EJ using a method similar to conventional open surgery.
Statistical analysis
Statistical analysis was performed using SPSS version 18.0. Data were expressed as mean ± standard deviation values. Categorical variables were analyzed by chi-squared test and Fisher's exact test, and continuous variables were analyzed using Student's t-test. A value of P < .05 was considered statistically significant.
Results
The clinicopathological characteristics of the patients are given in Table 1. There were no significant differences in age, sex, body mass index (BMI), American Society of Anesthesiologists physical status, neoadjuvant chemotherapy, and clinical stage between the intracorporeal and extracorporeal reconstruction groups.
Clinicopathological Characteristics of the Patients
Data are given as mean ± standard deviation or number (%).
ASA-PS, American Society of Anesthesiologists physical status; BMI, body mass index; cStage, clinical stage; EJ, esophagojejunostomy; NAC, neoadjuvant chemotherapy.
Operative and postoperative results are given in Table 2. The operative time and anastomosis time in the intracorporeal reconstruction group were significantly longer than those in the extracorporeal reconstruction group. The visual analogue scale (VAS) scores in the extracorporeal reconstruction group were higher than those in the intracorporeal reconstruction group, with significant differences between the 2 groups when VAS scores were recorded 1, 2, and 3 days after surgery. Accordingly, the postoperative analgesic dosage used in the extracorporeal reconstruction group was significantly higher than that in the intracorporeal reconstruction group. In addition, the postoperative hospitalization time for patients in the intracorporeal reconstruction group was significantly shorter than that for patients in the extracorporeal reconstruction group.
Operative and Postoperative Outcomes
Data are given as mean ± standard deviation.
EJ, esophagojejunostomy; POD, postoperative day; VAS, visual analogue scale.
Surgical outcomes for patients with different BMIs are presented in Table 3. The operative time for overweight patients was longer than that for normal-weight patients in both the extracorporeal and intracorporeal reconstruction groups, and the reconstruction time for overweight patients in the extracorporeal reconstruction group was also longer than that for normal-weight patients. However, there was no significant difference in reconstruction time between overweight patients and normal-weight patients in the intracorporeal reconstruction group. Furthermore, the postoperative VAS score and analgesic dosage on the first postoperative day were significantly higher in the extracorporeal reconstruction group's overweight patients than in the normal-weight patients, whereas there were no significant differences in these two indices in the intracorporeal reconstruction group.
Surgical Outcomes for Patients with Different Body Mass Index Intracorporeal Esophagojejunostomy Group (n = 92) and Extracorporeal Esophagojejunostomy Group (n = 121)
Data are given as mean ± standard deviation.
BMI, body mass index; EJ, esophagojejunostomy; POD, postoperative day; VAS, visual analogue scale.
Postoperative complications are given in Table 4. The total EJ-related complications occurred in 6 cases in the intracorporeal reconstruction group and 7 cases in the extracorporeal reconstruction group, with no significant difference. Two patients in the intracorporeal reconstruction group and 4 patients in the extracorporeal reconstruction group developed anastomotic leakage, all of which were managed with enhanced drainage and supportive treatment. Anastomotic stenosis occurred in 1 case in the intracorporeal reconstruction group and 1 case in the extracorporeal reconstruction group, which were resolved by endoscopic balloon dilation.
Postoperative Complications
Data are given as number (%).
EJ, esophagojejunostomy.
Non-EJ-related complications were observed in 11 patients in the intracorporeal reconstruction group and 20 patients in the extracorporeal reconstruction group, with no significant difference. Pancreatic fistula accounted for the majority of complications, followed by intraperitoneal hemorrhage and stump leakage. All patients with pancreatic fistula and stump leakage were successfully treated conservatively. Six patients with intraperitoneal hemorrhage were managed with blood transfusion, and the other 2 patients underwent reoperation to stop the bleeding. Of the 4 patients with intraperitoneal fluid collection, 3 were treated with ultrasound-guided catheterization, and the other patient received conservative treatment.
Discussion
The standard technique of EJ in open surgery and laparoscopic-assisted total gastrectomy employs circular stapled anastomosis using PSIs, which is a single stapling technique. However, with the advent of intracorporeal reconstruction, intracorporeal purse-string suture and anvil insertion have become challenging procedures, as traditional PSIs are not suitable for laparoscopic surgery. Consequently, several alternative solutions have emerged to circumvent laparoscopic purse-string sutures, including linear stapling technique and double or hemi-double stapling technique.6–10 Some surgeons opt for using a single stapling technique by performing hand-sewn purse-string suture, but this method is technically demanding and time-consuming. A specialized instrument called Endo-PSI(II) (Hope Electronics, Chiba, Japan) was developed for laparoscopic purse-string suture, but it has not gained widespread use.
The technique described herein was devised and modified by the author. It is straightforward, closely resembling the open surgery technique, and is both feasible and effective. The primary drawback of the original method is that after transecting the esophagus above the esophagogastric junction, the esophagus stump retracts into the thoracic cavity, necessitating its retrieval into the abdominal cavity for purse-string suture, anvil insertion, and fixation. However, the esophagus stump is fragile and susceptible to tearing, making laparoscopic instrument manipulation difficult. To address this issue, we modified the original technique using a self-traction method, in which a small portion of the left esophagus wall is retained during esophagotomy until anvil insertion and fixation are completed. With this modified method, anvil insertion into the esophagus stump and fixation are much easier.
Furthermore, the modified method has another advantage: it can reduce the risk of esophageal mucosa detachment from the esophageal muscular layer during anvil insertion. However, the modified method carries the risk of tumor cell spillage, so in this group of cases, the esophagus was ligated and blocked with thick wire at the distal end of the predetermined incision line before it was cut open.
To further evaluate the feasibility and effectiveness of the modified purse-string stapling technique for intracorporeal EJ during laparoscopic total gastrectomy, we compared the surgical results with those of the extracorporeal reconstruction technique through mini-laparotomy. Our findings revealed that although the intracorporeal reconstruction group required longer anastomotic time than the extracorporeal reconstruction group, patients in the former group experienced less postoperative pain and had shorter postoperative hospital stays. A study comparing the short-term surgical outcomes of intracorporeal and extracorporeal gastroduodenal anastomosis after laparoscopic distal gastrectomy also found that the intracorporeal anastomosis group experienced less postoperative pain and required fewer analgesic medications. 11 The small incision size required for intracorporeal reconstruction may be the reason for these results, as smaller incisions cause less pain and allow patients to ambulate earlier and recover more quickly. Obesity is a risk factor for most abdominal surgeries, as it increases the overall postoperative complication rate.12,13
However, laparoscopic approaches may reduce the occurrence of these complications. 14 In this study, we evaluated the effectiveness of intracorporeal and extracorporeal reconstruction techniques in overweight patients and compared them with normal weight patients. We discovered that the anastomotic time in the intracorporeal reconstruction group was not affected by the patient's body size. Conversely, patients with high BMI in the extracorporeal reconstruction group required longer anastomotic times than those with low BMI. This may be owing to the esophagojejunal anastomosis site in obese patients being deeper, leading to poor exposure of the surgical field, which is challenging to complete through mini-laparotomy. However, the intracorporeal reconstruction technique can still provide a clear and stable surgical field of vision even in obese patients. In addition, unlike the extracorporeal reconstruction technique, there was no increase in postoperative pain score and analgesic dosage for overweight patients using the intracorporeal reconstruction technique. Thus, the intracorporeal reconstruction technique may be particularly suitable for obese patients.
The incidence of EJ leakage and stenosis in this study is acceptable compared with previous reports.15,16 However, several studies comparing the effects of using a linear stapler and a circular stapler in EJ have found that although both procedures are safe and feasible, the incidence of postoperative complications, such as anastomotic leakage and stenosis with the circular stapler method, is higher than with the linear stapler method.17,18 The reason for this discrepancy may be that these studies have not conducted subgroup analysis based on different types of circular stapled EJ. In fact, there are three distinct types of circular stapled EJ, including the use of single stapling, hemi-double stapling, and double stapling techniques. Unlike single stapling technique, hemi-double stapling technique forms one overlapped staple line, whereas double stapling technique forms two overlapped staple lines.
Although there are several possible explanations for anastomotic leakage and stenosis, local ischemia at the intersection of the staples may be the main cause, and subsequent fibrosis may result in anastomotic stenosis. Using only the single stapling technique in this study may be the primary reason for the low complication rate in our patients. Consistent with the findings of this study, a recently published propensity-matched analysis comparing the surgical outcomes of the “Lap-Jack” purse-string circular stapler method, a type of single stapling technique, and the linear stapler method in totally laparoscopic total gastrectomy, found that the early and late postoperative complication rates in the circular stapler group were lower than those in the linear stapler group, although the results were not statistically significant. 19 Other studies comparing single stapling technique and hemi-double stapling technique for intracorporeal circular stapled EJ have also shown that single stapling technique can reduce the incidence of anastomotic complications after laparoscopic total gastrectomy.20,21
In this study, we divided patients into an extracorporeal reconstruction group and an intracorporeal reconstruction group, rather than a laparoscopic-assisted total gastrectomy group and a totally laparoscopic total gastrectomy group, because the definition of totally laparoscopic total gastrectomy is currently a controversial topic. Some scholars suggested that only laparoscopic total gastrectomy with intracorporeal linear stapled EJ can be defined as totally laparoscopic total gastrectomy, as it requires no additional incision to conduct EJ reconstruction. 22 In fact, regardless of the method used, the excised specimen always requires an additional incision to be extracted, so we believe that using linear and circular staplers for intracorporeal EJ reconstruction is similar in terms of incision trauma. Using the technique described in this article, a 3-cm incision is sufficient to complete a 25-mm circular stapler reconstruction surgery, and the actual incision length depends on the size of the specimen or tumor.
However, the additional incision of the linear stapler method can be located at any position in the abdomen, such as in the lower abdomen, where the incision is less painful and more comfortable. However, the incision of the circular stapler method can only be located at the umbilicus or epigastrium, which may be a disadvantage of the circular stapler method.23,24
So far, there is no consensus on the standard method for EJ in laparoscopic total gastrectomy. The linear stapler method has the advantage of having a larger diameter of anastomosis than the circular stapler method, which may reduce the incidence of anastomotic stenosis. However, the linear stapler method requires a longer esophagus to be freed to ensure sufficient distance for anastomosis, which may increase the risk of subsequent mediastinitis in the event of anastomotic leakage. We chose the intracorporeal circular stapled EJ using a single stapling method because it is a mature method widely used in open surgery. It is also a better method when patients with tumors located at the gastroesophageal junction or gastric fundus tumors invading the esophagus need to remove more esophagus. 5 Further investigations comparing the linear stapler EJ reconstruction with the circular stapler EJ reconstruction using single stapling technique are warranted.
This study has some limitations. First, this is a single-center retrospective study, and there will inevitably be some biases. Second, the procedures of the 2 groups of patients were performed in different periods, and the extracorporeal reconstruction group started from 2014, whereas the intracorporeal reconstruction group started from 2018. There may be some differences in technical maturity of surgeons, surgical instruments, and postoperative care protocols.
Conclusions
The modified intracorporeal purse-string stapling technique for EJ during laparoscopic total gastrectomy is a safe and viable option, exhibiting less invasiveness and comparable outcomes with the extracorporeal reconstruction method, especially suitable for obese patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.