
Abstract
Background:
Total extraperitoneal approach for laparoscopic inguinal hernia repair (L-TEP) allows for better dissection, lesser chance of bowel injury, and quicker operating time. However robotic groin hernia repair is currently performed only through transabdominal route as it allows for more mobility of the arms. This study is aimed at studying the feasibility and outcomes of robotic totally extraperitoneal (R-TEP).
Methods:
A prospective nonrandomized comparative study was conducted to compare R-TEP with L-TEP. Out of a total of 88 patients with inguinal hernia, 44 patients underwent R-TEP and other 44 patients underwent L-TEP over a period of 15 months. All R-TEP were performed with Cambridge Medical Robotics (CMR) Versius. The outcomes were analyzed over a minimum follow-up period of 6 months.
Results:
All patients were males with a mean age of 45.9 years. Average body mass index was 28.7. Mean docking time for R-TEP was 12.7 minutes. Overall time taken for R-TEP (mean 60.47 minutes) was significantly higher (P < .001) than L-TEP (mean 38.45 minutes). When the console time of R-TEP and overall time of L-TEP were compared, there was no significant difference (P = .053). A RCT (RIVAL Trial) conducted by Prabhu et al. showed their robotic transabdominal preperitoneal (R-TAPP) time of median 75.5 (59.0–93.8) minutes. Kimberly et al. had their overall time of 77.5 minutes and Andre Luiz et al. had a console time of 58 minutes. When we compared the data, the overall time of R-TEP is lesser compared with R-TAPP. Postoperative pain on POD-1 showed that the robotic group had significantly lower pain. There were no recurrences noted in the study period.
Conclusion:
With our study, we have shown that R-TEP performed using the principle of laparoscopic triangulation technique with CMR Versius is feasible and reproducible. Although the overall time is significantly more in R-TEP when compared with L-TEP, console times of R-TEP and overall times of L-TEP were very similar. Console times of R-TEP are much lesser compared with other studies on R-TAPP. R-TEP can be a better alternative to R-TAPP and can be considered at par with L-TEP. A systematic RCT would provide a better picture.
Introduction
The earliest evidence of hernia repair dates to ∼1552 BC in ancient Egypt. 1 The word “hernia” originates from the Latin word for ‘Prolapse’. Henri Fruchaud initially coined the term groin hernia, 1 which is used even to this day. Edoardo Bassini established a modern herniorrhaphy tissue repair technique. Irving L Lichtenstein introduced the first tensionless technique based on strengthening of the posterior wall of inguinal canal with prosthetic material in 1968. 2 By 1990, laparoscopy was gaining popularity and surgeons had to reimagine ways to do the same surgeries. Arregui et al. described transabdominal preperitoneal (TAPP) technique for the first time in 1992. 3 A year later J B McKernan found a way to reach the same hernia site between the abdominal planes by a totally extraperitoneal (TEP) approach. He described a laparoscopic procedure for prosthetic repair of inguinal hernias using an extraperitoneal approach. 4 European Hernia Society's international guidelines recommended laparoscopic inguinal hernia repair for improved postoperative pain outcomes compared with open surgery and now a laparoscopic approach has become a benchmark for most of groin hernias.
As with the change in era from open to laparoscopy, we are at the beginning of the Robotic era. In 2007, the first robotic inguinal hernia repair was performed. 5 The most common approach in robotic groin hernia repair is a transabdominal route as it allows for more mobility of the arms. There are few robotic groin hernia repairs being done through preperitoneal approach as it is considered to be difficult to approach with the robotic equipment due to restricted mobility of the arms. After initial experience with robotic transabdominal preperitoneal (R-TAPP), we attempted and completed robotic totally extraperitoneal (R-TEP) at the first attempt, including placement of mesh and fixing it. Hence, we set out to perform R-TEP to see the feasibility and if it could be easily reproducible. Here we present the data from our initial experience.
Materials and Methods
A prospective nonrandomized comparative study was conducted to see the feasibility of R-TEP, for analyzing the short-term outcomes and to compare the data with laparoscopic totally extraperitoneal (L-TEP) performed by the same operating team. An Institutional Ethics Committee approval was obtained. The study was conducted from July 2022 to September 2023 and followed up until March 2023. Surgeries were performed by the same surgical team. Forty-four patients underwent robotic inguinal hernia repair, and 44 patients underwent laparoscopic hernia repair around the same time. The robotic cases were funded by the institution.
All patients above the age of 25 years with inguinal hernias were included. We excluded patients with inguinoscrotal hernias, recurrent hernias, previously operated contralateral hernias irrespective of open or laparoscopy, and patients who had previous surgery with infraumbilical scar. Patients with ASA III and above were also excluded. All the patients underwent preoperative ultrasound of abdomen for confirmation of clinical diagnosis. Patients were admitted the previous evening of the surgery.
All robotic hernia surgeries in this study were performed with Cambridge Medical Robotics (CMR) Versius robot. For evaluation purpose, we divided the robotic operative times into three parts:
Docking time (Time from incision to docking) Console time (exclusively surgery, including the port adjustments during the procedure until skin closure) Overall Time (Docking time+Console time)
Primary outcome was to see if R-TEP was feasible and reproducible with CMR Versius and compare the timings with L-TEP and R-TAPP. There were no preset secondary outcomes as this was a pilot study. Parameters that could be assessed were taken into consideration.
Postoperatively, pain assessment was done using the Visual Analog Scale (VAS), where 0 was no pain and 10 being worst pain, with 5 being moderate pain. VAS was taken on first postoperative day, at the end of 1 week, and at 1 month. Patients were followed up in outpatient at the end of 1 week, 1 month, 3 months, and 6 months.
Statistical analysis was performed with SPSS software version 21. Continuous data were analyzed with Mann–Whitney U test. Categorical data were assessed by Pearson's chi-square test. P value of <.05 was considered significant.
Operative Techniques
Patient and equipment position
Under General Anaesthesia, patients were placed in supine position with Trendelenburg tilt. Urinary bladder catheterization was performed and patient was draped (Fig. 1). The surgeon console was placed facing the direction of the target organ and procedures were performed in three-dimensional (3D) mode. The Vision cart was placed as shown in the Figure 1. Monopolar scissors and curved bipolar were connected to right and left bedside units (BSUs), respectively. The units were placed adjacent to the patient on the right and left side close to the lumbar region. The camera arm was constantly adjacent to the left shoulder. BSU positions varied by few inches depending on the body habitus of the patient and triangulated toward the side of the hernia being worked.

OT setup. (1) Right side hernia. (2) Left side hernia. OT, operation theater.
Port placement and port training
We have been following the triangulation technique for laparoscopy, where the working ports are placed on either side of the camera and all three are triangulated toward the target organ. We replicated this robotically. A vertical incision of ∼12 mm was placed at the inferior border of the umbilicus and extraperitoneal space entered. The 12 mm port was introduced and the balloon at the tip of the port was inflated with 10 cc of air. CO2 pressure was maintained at 12 mm Hg. With the 0-degree camera, the rectus muscle on the right was displaced anteriorly by sliding the scope on the posterior rectus sheath until the border of the rectus was reached (Fig. 2).

BSU positions and port placement. (1) BSU positions. (2) Port positions. BSU, bedside unit.
A 7 mm incision was placed 7–8 cm away from the camera port at the lateral border of the right rectus. A 7 mm right working port was placed into the extraperitoneal space under vision. With scissor through the right working port, the opposite side was dissected, space created, and the left-hand working port was placed. Robotic bipolar and curved scissors were introduced through left and right ports, respectively, and individually ports were trained toward the initial site of dissection. Once both were in place, then camera was fixed to the visualization arm and port trained.
Dissection of extraperitoneal space
The space of Retzius
The surgery began with the dissection of the space of Retzius, in between the two layers of the transversalis fascia (Fig. 3). Retzius space was completely freed of the loose areolar tissue from the arcuate line to pubic bone and laterally until the fusion at the inferior epigastric vessels. Direct hernias encountered in this space was reduced with traction and sharply dissecting away the pseudo sac. If a large sac was present, it was plicated and fixed to Cooper's ligament with Prolene 1 suture.
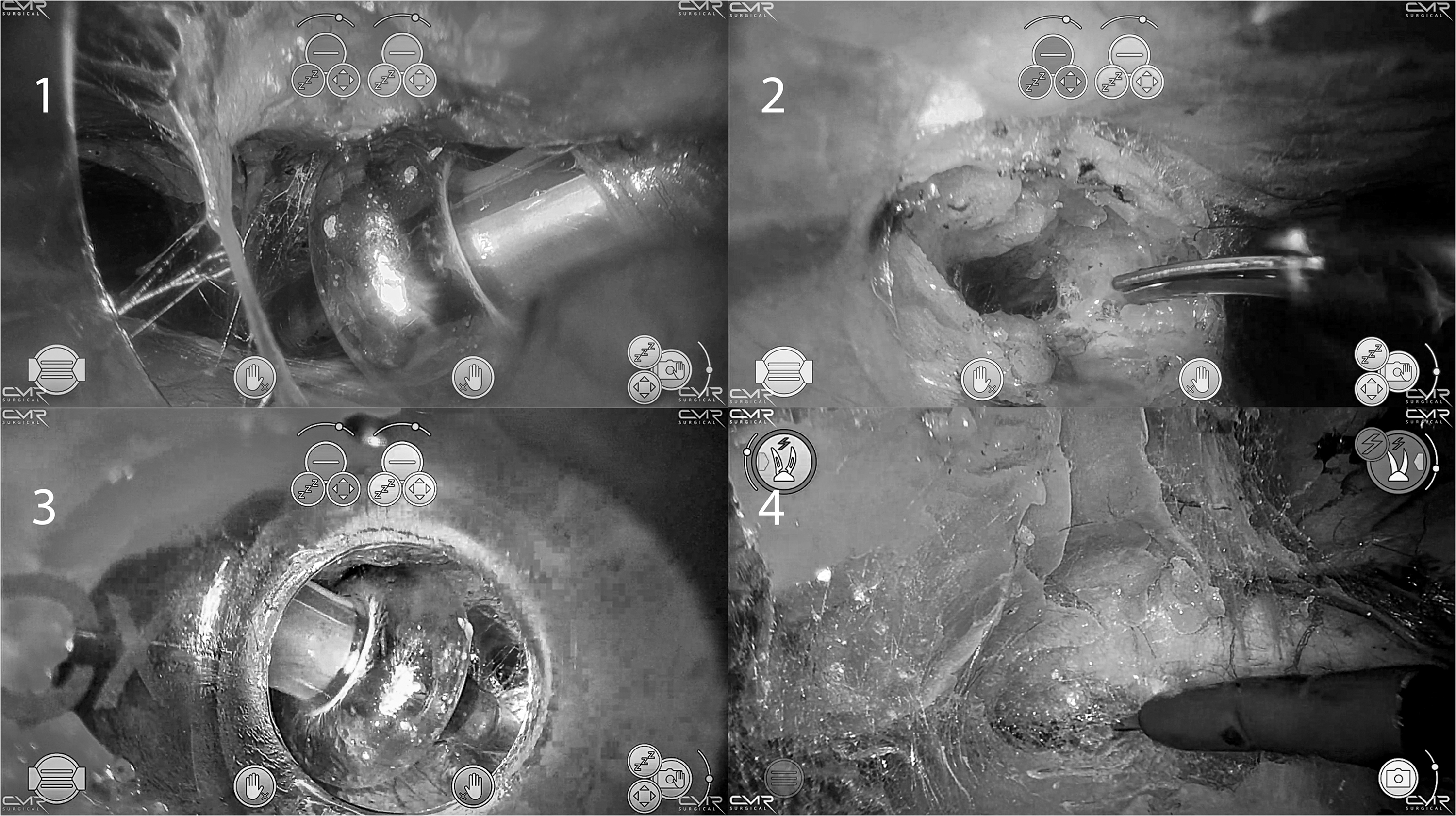
Port placement. (1) Right hand working port. (2) Midline crossover for left port. (3) Left hand working port. (4) Retzius dissection.
In most cases, dissection of extraperitoneal space was performed with a single port training. Initial extent of coverage of instruments through port training for left side hernia extended from right pubic ramus close to the anterior superior iliac spine and vice versa. At times, repositioning the BSU and a report training was required for better triangulating while dissecting beyond the anterior superior iliac spine. For example, the left side hernia, the right BSU was moved slightly caudally and closer to the bed. This maneuver freed up the mobility of the elbow of the right BSU and rectified the clash. Similar procedure with left BSU was performed while dissecting the right side hernia.
The Bogros space
The fascia transversalis attachment was taken down adjacent to the inferior epigastric vessels and Bogros space was entered (Fig. 4). The transversalis sling was sharply cut and the indirect sac when present was reduced. The gonadal vessels and vas deferens were dissected from the peritoneum and parietalization of the spermatic cord structures was done.
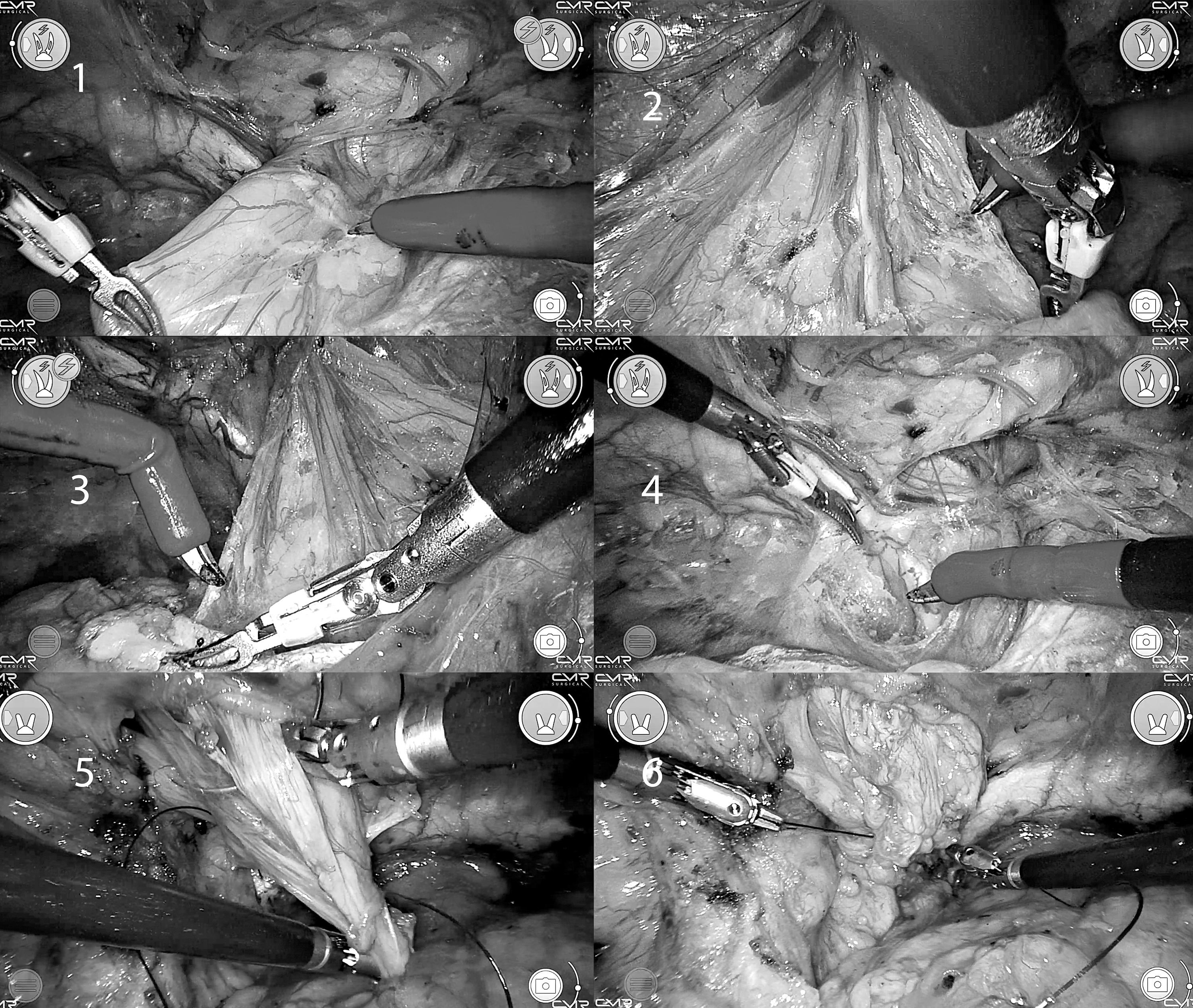
Retzius space dissection. (1) Dissection of direct sac. (2) Medial dissection. (3) Parietalization of peritoneum. (4) Completed Retzius space dissection. (5) Plication of direct sac. (6) Sac fixation to Cooper's ligament.
While working on the lateral space of the left side hernia, the dominant right hand can perform the dissection at a comfortable angle. While dissecting the lateral space of the right side with dominant right working arm, BSU works at an angle, which slightly restricts the mobility of the arm. This is solved by repositioning the BSU. Alternatively, we changed the scissors to the left working arm and performed the right lateral dissection (Fig. 5).
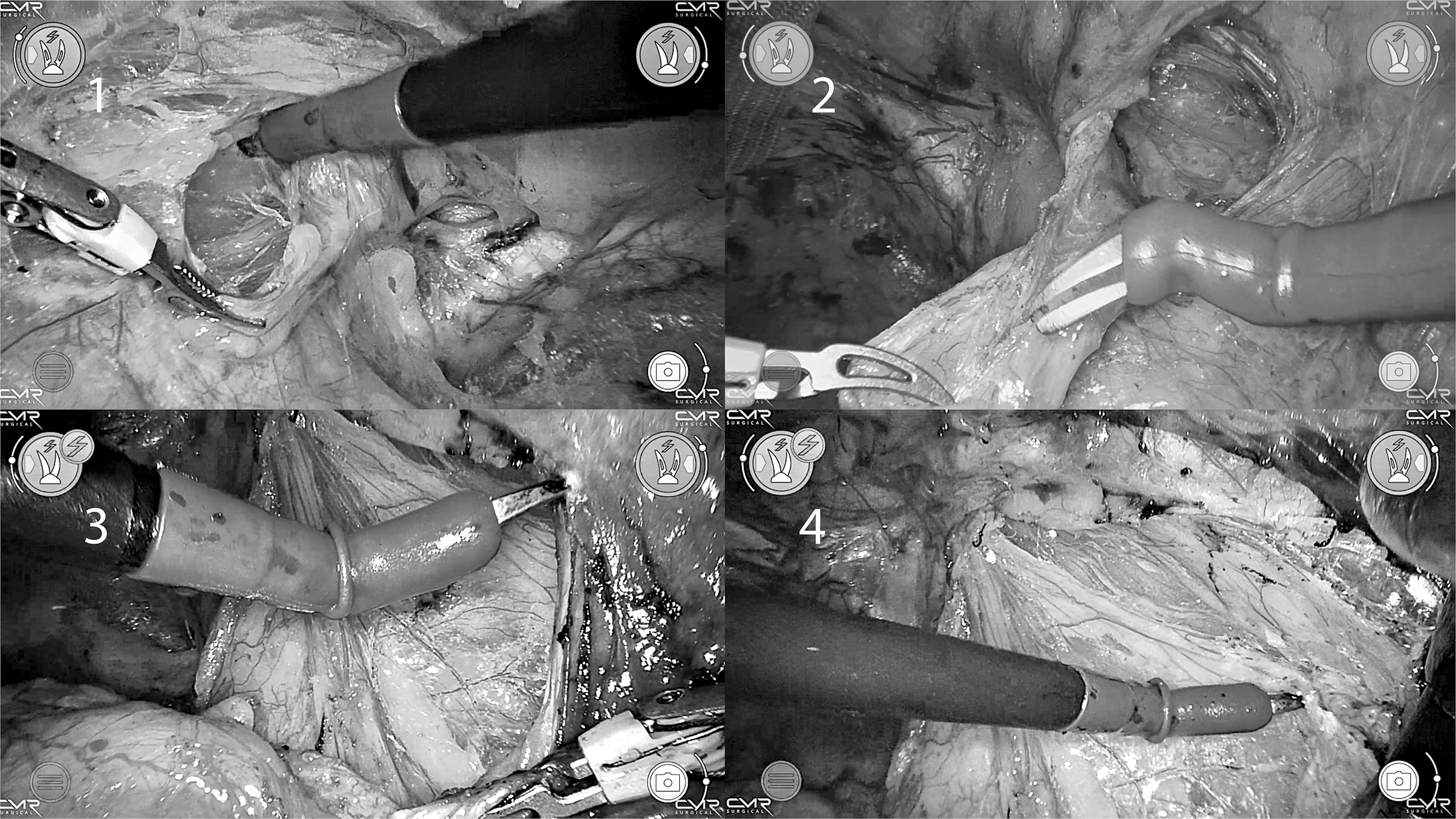
Bogros space dissection. (1) Bogros space entry. (2) Indirect sac dissection. (3, 4) Lateral peritoneal dissection.
Mesh placement
A polypropylene mesh of size 12 by 18 cm was used (Fig. 6). Mesh was introduced into the dissected Retzius space with a needle holder. It was unfolded in the extraperitoneal space and spread over the myopectineal orifice with robotic arms. The mesh was fixed to Cooper's ligament on the initial side of dissection and once similar fixation was done on the opposite side, a single suture was placed on the rectus muscle incorporating both the meshes where they overlap. At the end of procedure, intra-abdominal inspection was done and found the mesh was well placed.
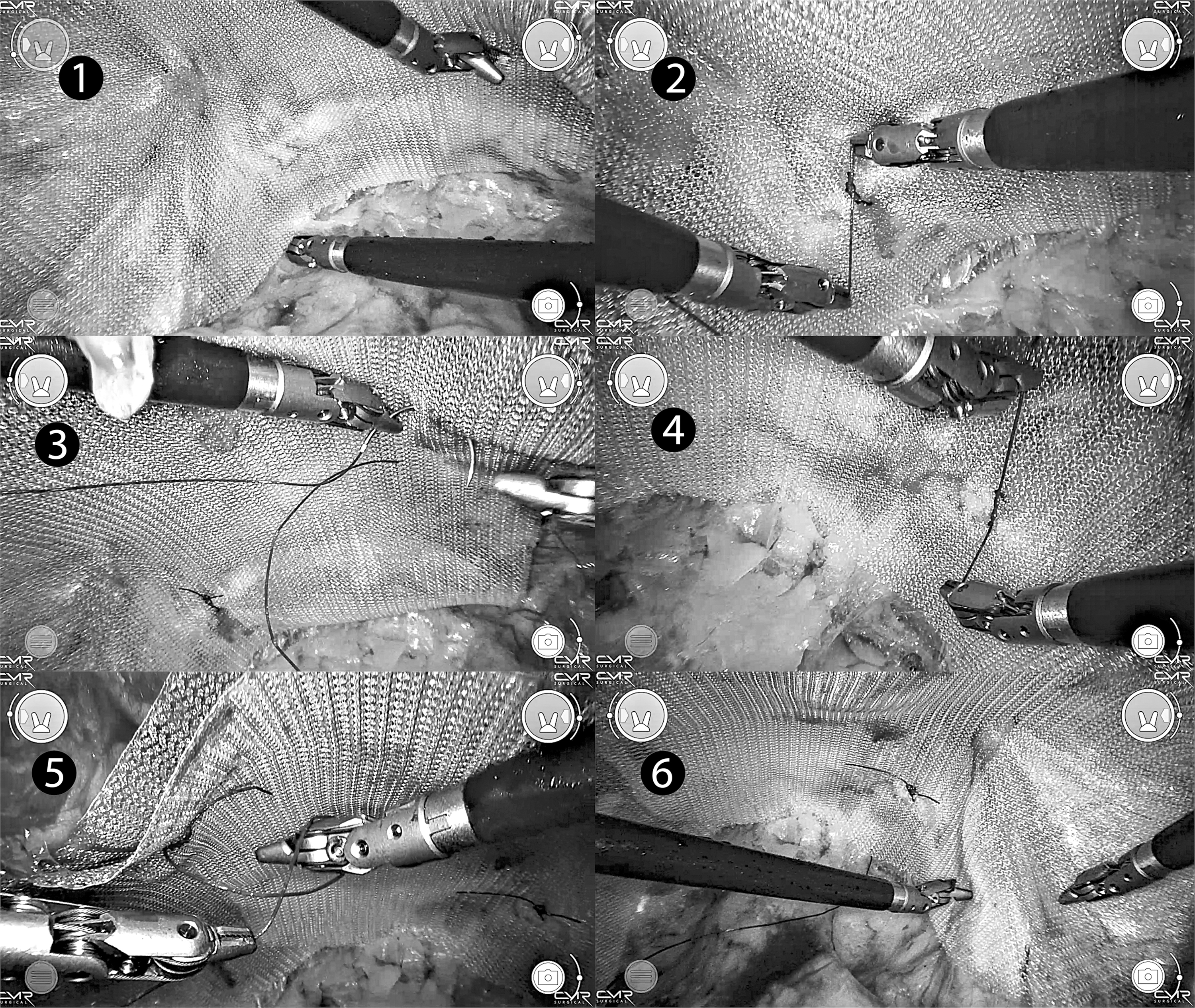
Mesh placement. (1) Left side mesh placement. (2) Fixation to left Cooper's ligament. (3) Left mesh-midline fixation. (4) Fixation to right Cooper's ligament. (5) Both mesh-midline fixation. (6) Holding the mesh in situ before deflation.
Postoperative course
Patients were made to walk and were started on clear liquids within 4 hours of the surgery and by night a soft diet was started. The urinary catheter was removed on POD-1 and the patients were discharged in the morning.
Postoperative pain was estimated with Visual Analog Score. Initial postoperative analgesia with 1 g paracetamol and 50 mg Tramadol was given after induction. One gram of paracetamol was given at 6 hours and on demand thereafter with a repeat of paracetamol 1 g.
Results
Eighty-eight patients who fit the inclusion criteria were included in the study. All patients were males with a mean age of 45.9 years (26–79 years). Average body mass index was 28.7 (26.4–32.6) (Table 1). Out of 44 in each group, there were 29 unilateral hernias in the robotic group and 21 in the laparoscopy group. Bilateral hernias contributed to 15 and 23 in the robotic and laparoscopic group, respectively. Mean docking time for R-TEP was 12.7 minutes. Mean overall time taken for R-TEP was 60.47 minutes (95% confidence interval [CI]: 53.87–67.08) and for L-TEP was 38.45 minutes (95% CI: 35.34–41.57). Comparison of overall times between robotic and L-TEP showed that time taken was significantly lower in L-TEP (P value <.001). While unilateral R-TEP took a mean of 53.0 minutes (37.0–69.0), bilateral R-TEP took 99.6 minutes (79.5–119.7). Subsequently when we compared with the console time of R-TEP with overall time of L-TEP, there was no significant difference (P value: .053).
Robotic Totally Extraperitoneal Compared with Laparoscopic Totally Extraperitoneal
BMI, body mass index; L-TEP, laparoscopic totally extraperitoneal; R-TEP, robotic totally extraperitoneal.
The time comparison is consolidated in Table 2.
Robotic Totally Extraperitoneal Versus Laparoscopic Totally Extraperitoneal Time Comparison
L-TEP, laparoscopic totally extraperitoneal; R-TEP, robotic totally extraperitoneal.
Intraoperative deviations
Two patients had rents in the peritoneum, which were sutured robotically with 3–0 PDS, in a continuous fashion. One patient had a small rent in the peritoneum, which was looped with 3–0 PDS. Two patients had large direct sac and was plicated robotically. One patient had bilateral lipomas of the cord, which was reduced robotically. There was one port site bleed, which occurred while inserting the 7 mm right hand working port. We inflated the port balloon and applied traction with the balloon, which arrested the bleed.
Postoperative pain assessment on POD-1 showed that the robotic group had significantly lower pain (P = .023) with a mean score of 1.43 (0–4), while the laparoscopy group had a scoring of 2.06 (0–6). At 1 week and at 1 month, both groups did not exhibit any significant differences in pain.
Complications
Subcutaneous emphysema: In one case, the left hand port balloon had deflated and tip had retracted into the rectus plane causing subcutaneous emphysema. The patient complained of a crackling sensation under the skin on POD-1. It resolved in 7 days.
One patient developed a seroma of 3 cm by 2 cm size in the robotic group, which resolved on its own.
There was no recurrence in robotic or laparoscopic series we studied.
There were no surgical-site infections, postoperative bleeding, or patients with chronic pain. All cases were completed with three ports and there was no requirement for additional port placement. There were no conversions to laparoscopy or open techniques in our study. No drains were placed. All patients were discharged on POD-1.
Postoperative follow-up
All patients were followed up for a period of 6 months, starting at even days, 30 days, and at the end of 6 months. All the patients had returned to their routine activities by the first follow-up. There were no recurrences noted in the study period.
Discussion
When learning a new procedure, performance tends to improve with experience; this is known as the “learning curve.” 6 If the laparoscopic method can be replicated equally well with a robot, then adopting the technique requires only to know how to use the robot. Minimally invasive hernia repairs have lots of merits when compared with that of the open repairs. They include reduced hospital stay, earlier return to normal activities, and more importantly reduced postoperative pain.7–10 As we enter the era of robotics, rate of robotics in inguinal hernia repairs are increasing exponentially. 11
All the robotic inguinal hernia repairs reported to date have been through the transabdominal (R-TAPP) route. Few attempts have been made through the extraperitoneal space and usually are attempted with prostatectomy. 12 Our institute is a high-volume center, and with our expertise most of the groin hernias are managed by L-TEP; the need for laparoscopic TAPP seldom arises. With adequate experience most of the groin hernias can be managed by TEP instead of TAPP. Hence, we decided to see if we can replicate the same L-TEP procedure with the Versius robot without modifying our existing triangulation technique.
This study revealed that our primary outcome, R-TEP, was feasible and easily reproducible, as evidenced by completion of 44 cases without any conversions to laparoscopy or open. The principles of L-TEP technique that we follow at our institution were easily replicated with the CMR Versius Robot. Other outcomes that are identifiable from this study are included as well.
Port placement
All our laparoscopic hernias are performed through camera port placed at the inferior border of the umbilicus, as it gives equal access to both the sides. The intention was to replicate our laparoscopic technique. Placing the incision above the level of umbilicus would have required more extraperitoneal dissection and risk peritoneal breach causing the CO2 to escape into the peritoneal cavity. With the present technique, minimal dissection is needed for port placement and no dissection is required above the level of the umbilicus.
Docking time
This study was conducted after a certain level of experience with performing R-TAPP with CMR Versius. This had allowed us to understand the robot, docking principle, and arm clashes. Over the period of 44 cases, we gradually improved over the docking methods and once we standardized the BSU position, it was easy to train the operating team. Mean time taken for docking for first 16 cases was 15.8 minutes and mean of 12.31 minutes for next 16 cases and mean time of 9.76 minutes for last 12 cases, with an overall mean of 12.77 minutes. This shows that with targeted and conscious training, docking times can be reasonably reduced and thus reducing the overall operating time. It is now widely known that robotic surgery takes more time compared with laparoscopy, hence every small step taken to save time in robotic contributes in improving the overall time.
3D vision
The camera is self-controlled and has 3D vision. Approaching the surgical planes and dissecting through them is far superior compared with the hand-held camera by the assistant in laparoscopy.
Dexterity
Due to dexterity of the instrument, while performing parietalization of peritoneum and lateral peritoneal dissection, the instrument could be turned 90 degrees and approached safely from above without contact of the instrument with the underlying bowel as opposed to a laparoscopic instrument such as the Maryland forceps, which approaches the same point more tangentially with a possibility of the metal portion of the instrument forceps coming in contact with the bowel. The peritoneal rents were sutured robotically. Most movements of suturing occurred at the wrist of the needle holder and minimal movements at elbow of the BSU. This task was accomplished easily in the extraperitoneal space without the need of laparoscopic conversion.
R-TAPP versus R-TEP: dissection and time
In R-TAPP, pushing the bladder posteriorly while dissecting the Retzius space is difficult as the peritoneum blocks the view in the midline between the two medial umbilical ligaments. It is more difficult in a unilateral hernia as completion of midline dissection cannot be done from the opposite side. In an R-TEP approach, the Retzius Space dissection is done at the beginning itself pushing the bladder posteriorly freeing the space for movement of the instruments. Prolonged operating time remains one of the arguments against robot-assisted surgery. 13 Operating in the extraperitoneal plane allows us access to both hernias without need for the intentional breaching of peritoneum. Furthermore, peritoneal flap closure is not required, which saves time. L-TEP approach is considered to be more difficult than TAPP, but may have fewer complications. 14 Extrapolating the principles of L-TEP and TAPP, it could be safely assumed that bowel injury and solid organ injury and infection rates would be lower when surgery is performed in extraperitoneal plane.
We searched the data for R-TAPP and referenced those times. A RCT (RIVAL Trial) conducted by Prabhu et al. showed their R-TAPP time of median 75.5 (59.0–93.8) minutes. Kimberly et al. had their overall time of 77.5 minutes and Andre Luiz et al. had a console time of 58 minutes. When we compared the data, overall time of R-TEP is faster compared with R-TAPP15–17 (Table 3).
Robotic Totally Extraperitoneal Versus Robotic Transabdominal Preperitoneal
Pain
In laparoscopy, the fulcrum effect places the leverage on the abdominal wall causing the stretching of the skin and the tissues beneath it. This damage causes the tissues to release the inflammatory mediators resulting in pain. 18 With a robotic platform, the fulcrum is set at a point so the portion of the instrument in contact with the skin does not move from side to side. 18 No extra external force is applied to the surgical wound regardless of the direction in which the arm moves. 19 Most of the movements occur at the wrist of the working instruments, further reducing the movements at the trocar entry point. Additionally, trocars must be aligned along their axes to minimize the tension and to avoid causing stretching of the tissues, which contributes to increased pain. 20 Our study demonstrated that R-TEP had significantly lesser pain compared with R-TEP vs L-TEP (Table 1).
Nondominant hand
Physiologic tremors of the surgeon are readily transmitted through the length of rigid instruments. These limitations make more delicate dissections difficult if not impossible. 21 Robot filters out the unwanted motion. Advantages could increase the manipulative abilities of the surgeon irrespective of the dominant or nondominant hand. 22 This study's surgeon was well versed in using the left hand (nondominant) and could complete the right lateral dissection and right parietalization of peritoneum without much difficulty.
Conclusion
With our study we have shown that R-TEP performed using the principle laparoscopic triangulation technique with CMR Versius is feasible and reproducible. There is no need for supraumbilical extraperitoneal dissection (such as eTEP inguinal hernia surgery) for placement of camera port. Operating with a self-controlled 3D vision makes dissection in the anatomical planes much easier and with better ergonomics. When compared with L-TEP, time taken for R-TEP is significantly more. The time taken is mostly due to initial docking. Exclusive console time shows that R-TEP is at par with L-TEP. As we avoid entering peritoneal cavity, bowel and solid organ injury is less likely. As peritoneal suturing is avoided, the operative time over R-TAPP is less. Thus R-TEP can be a better alternative over R-TAPP and L-TEP for inguinal hernias. A systematic RCT would provide more evidence since we now know R-TEP is feasible.
Footnotes
Authors' Contributions
H.B.K.: Conceptualization, Methodology, Formal Analysis, Investigation, Data Curation, Writing—original draft, Writing—review and editing, Visualization, Supervision, and Project Administration. S.G.: Methodology, Investigation, Software, Validation, Formal Analysis, Data Curation, and Writing—review and editing. P.J.C.: Investigation, Data Curation, Writing—review and editing. J.P.: Investigation, and Data Curation. R.M.: Formal Analysis, and Investigation. R.S.: Writing—review and editing, and Supervision. S.R.: Supervision. P.C.: Resources, Writing—review and editing, Supervision, and Project Administration.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.