
Abstract
Background:
Peritoneal dialysis (PD) is a common method for treating end-stage renal disease (ESRD). Occurrence of inguinal hernia before and during PD is considered to be the main cause of treatment discontinuation, failure, and conversion to hemodialysis. In this study, we present a single-center experience about laparoscopic inguinal hernia repair and synchronous PD catheter placement and evaluated the feasibility and outcomes.
Methods:
During May 2018 to May 2022, a total of 216 consecutive patients with ESRD underwent laparoscopic PD catheter placement. Among them, 41 patients (27.7%) with coexistent inguinal hernia were included in this study. Individual information, complications, recurrent and new-onset hernias, and catheter survival were retrospectively analyzed.
Results:
Forty-one patients underwent laparoscopic inguinal hernia repair and synchronous PD catheter placement, 9 patients had bilateral inguinal hernia, and another 32 patients had unilateral inguinal hernia. The mean age was 46.49 years (range, 28–72 years), including 39 males and 2 females. There was no recurrent hernia and only 1 patient (2.4%) developed incisional hernia (trocar site hernia) which required hernia repair and discontinuation of PD. No postoperative complications were observed, such as bleeding, infection, and dialysate leakage. After a median follow-up of 37 months (20–58 months), there were no deaths and 97.6% (40/41) catheters were still working.
Conclusions:
Laparoscopic hernia repair and synchronous PD catheter placement is an effective and safe treatment for ESRD patients with coexisting inguinal hernia in virtue of low postoperative complications and high catheter survival.
Introduction
Peritoneal dialysis (PD) has the advantages of easy to use and relatively low cost compared with hemodialysis, and it is currently one of the main renal function replacement therapies for patients with end-stage renal disease (ESRD). 1 The presence of inguinal hernia in ESRD patients before treatment is an important reason for the cessation of PD or the conversion to hemodialysis. However, periodic injection of dialysate unavoidably increases intra-abdominal pressure, which may lead to hernia formation, especially in patients with abdominal weakness or defects.2,3 Although several previous studies have demonstrated the feasibility of synchronous tension-free hernia repair and PD catheter placement in a limited number of patients.4,5 There is no consensus or gold standard for the treatment of patients with inguinal hernias during PD.
In the epoch of minimal invasive surgery, laparoscopic technology has been widely used in hernia repair and PD catheter placement.6,7 Herein we present a single-center experience of laparoscopic inguinal hernia repair and synchronous PD catheter placement to evaluate the safety and effectiveness of this approach in ESRD patients.
Materials and Methods
Study population
Patients who underwent laparoscopic hernia repair and synchronous PD catheter placement from May 2018 to May 2022 were evaluated. Data collection included age, sex, cause of renal failure, type of hernia, length of operation, comorbidities, postoperative complications, assessment of recurrent hernia and new-onset hernia by telephone or outpatient follow-up, and catheter survival. Patients with serious risks for general anesthesia or/and history of lower abdominal surgery were excluded. Informed consent was obtained from all participants. The study was approved by the Ethics Committee of the People's Hospital of Huangshan and was performed following the Declaration of Helsinki.
Surgical strategy
Hernia repair
The laparoscopic surgery was performed under general anesthesia by the same team of surgeons after intravenous antibiotic prophylaxis with Cefuroxime 1.5 g. Patients were placed in the Trendelemburg position. The CO2 pneumoperitoneum was induced up to 12 mm Hg pressure by a Veress needle. A 10 mm trocar was placed using supra-umbilical incision for the 30° videocamera, followed by placement of two 5 mm trocar in the left and right lateral abdomen.
Laparoscopic exploration was performed to determine the type of hernia and detect occult hernia. The peritoneum around the myopectineal orifice should be exposed clearly. Then an arcuated incision was made in the peritoneum from the anterior superior iliac spine to the median umbilical ligament about 2 cm above the hernia ring. The medial and lateral compartments were dissected using blunt dissection in the avascular area after identification of the epigastric vessels. The peritoneum was separated from the male spermatic cord or the female round ligament. When the area around the myopectineal orifice was dissected completely, a self-gripping mesh (Progrip™, Covidien, Dublin, Ireland) in different sizes was placed to cover all possible hernia openings by at least 3 cm. The peritoneum was closed by continuous suture with the barb line.
PD catheter placement
Catheter placement was carried out after hernia repair. The surgical technique of catheter placement is consistent with that described in the previous study. 8 The deep cuff of PD catheter was located in the Douglas root, then the catheter can be fixed into the anterior abdominal wall. The superficial cuff was placed in the subcutaneous tunnel created between the subumbilical incision and the right 5 mm trocar site. Catheter inflow and outflow patency was tested intraoperatively.
Postoperative care
Catheter location was assessed by abdominal X-ray on postoperative day 1. Peritoneum washing with 300 mL of dialysis solution per day was started on postoperative day 3, and the volume of dialysis solution gradually increased to 2000 mL during the following 2 weeks. From week 3, the protocol of PD would be decided by a nephrologist based on patient's renal function.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation. Categorical variables are expressed as numbers (percent). The SPSS 22.0 software (IBM Corp., Armonk, NY) was used in data analysis.
Results
A total of 216 patients were given placement of PD catheter during the study period. Among these patients, 41 patients all had inguinal hernias, 32 of which were diagnosed preoperatively and 9 of which were found intraoperatively. All 41 patients underwent laparoscopic inguinal hernia repair and synchronous PD catheter placement, inguinal hernia was bilateral in 10 patients and unilateral in 31 patients (Fig. 1). Clinical characteristics of patients with inguinal hernia are shown in Table 1.
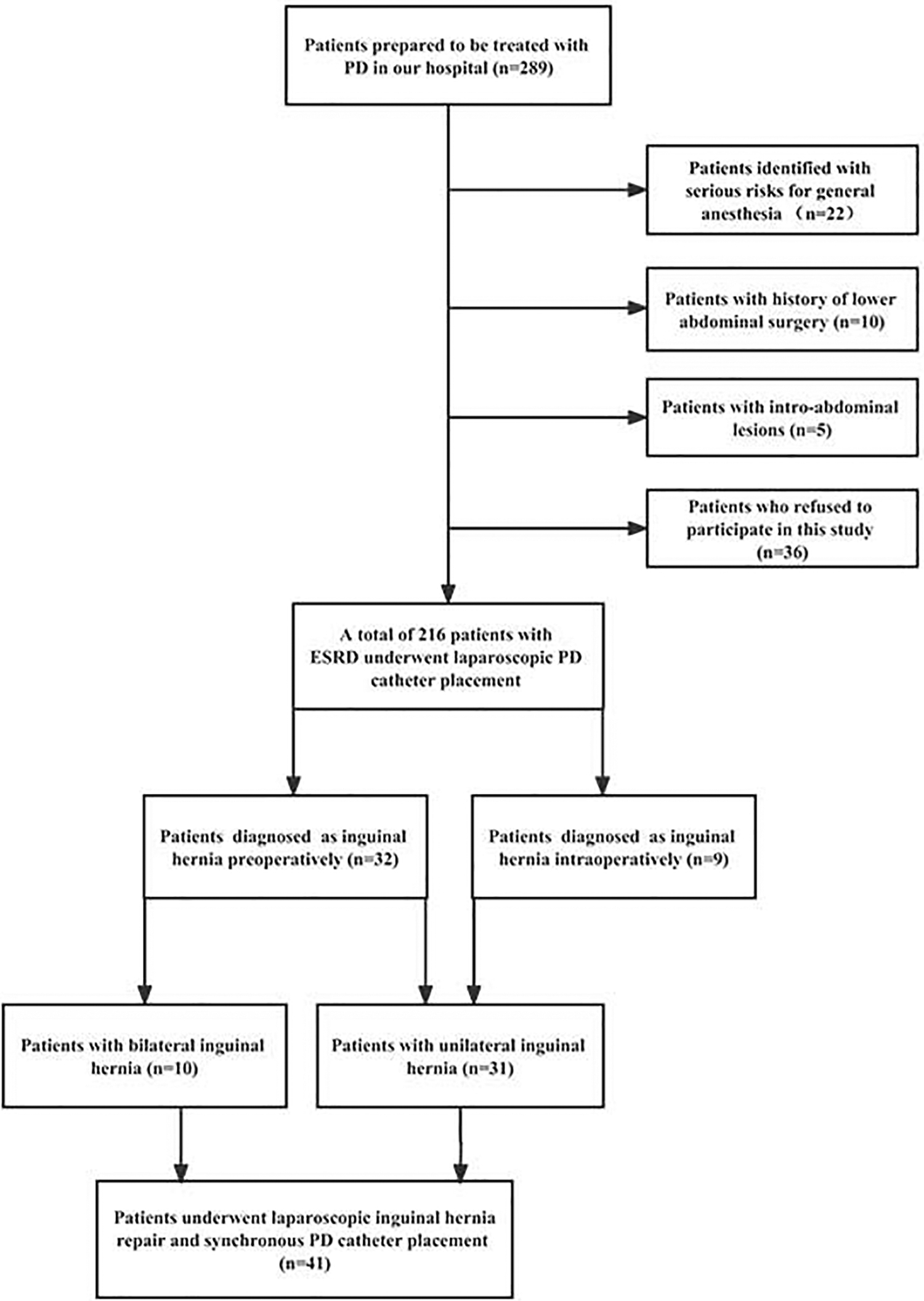
Flow chart for included patients. ESRD, end-stage renal disease; PD, peritoneal dialysis.
Patient Characteristics
SD, standard deviation.
The mean age was 46.49 years (range, 28–72 years), including 39 males and 2 females. The mean body mass index was 23.82 kg/m2 (range: 19.00–28.40). The causes of renal failure were chronic glomerulonephritis (n = 15), diabetes nephropathy (n = 14), hypertensive nephropathy (n = 5), lupus nephropathy (n = 4), obstructive nephropathy (n = 2), and unknown (n = 1). In addition, 22 patients suffered from hypertension and 19 patients suffered from diabetes.
Table 2 presents perioperative data of patients with inguinal hernia. All operations were performed successfully, with a mean length of operation of 73.03 minutes for unilateral inguinal hernia and 128.7 minutes for bilateral inguinal hernia. There were no recurrent hernias and only 1 patient (2.4%) developed incisional hernia located in the umbilicus region (trocar site hernia) at 17 months after surgery, which required hernia repair and termination of PD. No postoperative complications occurred, such as bleeding, infections, and dialysate leakage. After a median follow-up of 37 months (20–58 months), there were no deaths and 97.6% (40) of the catheters were still working. PD catheter was replaced in 1 patient owing to omental wrapping on 26 months postoperatively.
Perioperative Data
SD, standard deviation.
Discussion
The occurrence of inguinal hernia during PD period is a primary cause of termination of PD. Weakened connective tissue and increased abdominal pressure due to the infusion of PD fluid are the main reasons for the high incidence of inguinal hernia in patients with chronic renal failure. 9 The prevalence of symptomatic inguinal hernia in patients undergoing PD ranges from 11% to 33%10–12 and the incidence (14.8%) in our study is within this range. A thorough examination of groin region before PD is necessary. However, occult inguinal hernias are commonly asymptomatic before PD treatment and are difficult to detect by preoperative imaging assessment. The advantage of laparoscopic PD catheter placement is evident especially for patients with occult hernias. Because laparoscopic approach can simultaneously solve the problem of hernia repair to avoid secondary surgery, which is most important for patients with highly impaired renal function.
Kou et al. 13 demonstrated that synchronous hernia repair during PD catheter placement reduces the risk of symptomatic inguinal hernias development after initiation of PD therapy. No recurrent hernias were found in our study during follow-up, perhaps due to the timely intraoperative detection of occult hernias and the delicate and complete repair of the area around myopectineal orifice. However, one patient developed trocar site hernia located in the umbilicus region after 17 months postoperatively. This suggests that we should completely close the trocar incisions at a minimum of 10 mm located mostly in the umbilicus region after the laparoscopic surgery.
Compared to conventional open approach, patients can benefit from laparoscopic PD catheter placement with smaller scars and quicker recovery. 14 Also, it can ensure optimal placement of the catheter under visual guidance and reduce the postoperative complications, including catheter dysfunction and dialysate leakage. 15 No complications relating to catheter displacement occurred during the follow-up in this study, and the catheters worked for a long time; only 1 patient suffered from catheter blockage and catheter replacement at 26 months after surgery. Although techniques such as omentectomy, fixation of catheter, and omentum have been studied to reduce catheter occlusion and improve functional outcome,16–18 these operations may cause an increased risk of infection, bleeding, intra-abdominal hernia, and difficulty in extubation. We are neutral about these surgical procedures and fixation of catheter and omentum is not our operative practice. But we may take these measures to prevent catheter blockage in the future.
Dialysate leakage is a common complication associated with PD catheter implantation which can lead to catheter replacement, peritonitis, or temporary suspension of PD. 19 To avoid the occurrence of the dialysate leakage, Dombros et al. 20 recommend low volume exchange for 2 weeks after PD catheter implantation. In addition, Yang et al. 21 showed that there were no differences between early (<14 days) and late (>14 days) PD in term of dialysate leakage. Several studies have noted that the healing time of the peritoneum ranges from 7 to 14 days.22,23 Therefore, the principle of starting with low volume and gradually increasing the volume was implemented in our study, which made possible obtaining of good results without postoperative complications such as dialysate leakage. Similar results are also reported by some previous research.24,25 Another significant reason for this satisfactory result is that the subcutaneous tunnel can minimize the risk of dialysate leakage around the catheter.
To the best of our knowledge, our study is the largest investigation which included 41 ESRD patients who underwent laparoscopic hernia repair and synchronous PD catheter placement and analyzed the outcomes, postoperative complications, and catheter survival. However, this study is inevitably associated with certain shortcomings, namely, the lack of a control group and relatively limited number of patients. In addition, our study is a single-center experience with a rather short follow-up period. A prospective study with longer follow-up and larger sample size is needed in the future.
Conclusions
In the epoch of minimal invasive surgery, laparoscopic approach is feasible and safe for hernia repair and synchronous PD catheter placement in ESRD patients without hernia recurrence and postoperative complications during the follow-up time.
Footnotes
Authors' Contributions
T.C. designed the research and approved the submitted manuscript. Y.H. and C.H. drafted the manuscript. Y.H. and J.L. collected the data. C.H. and J.L. analyzed the data. All authors read and approved the final manuscript.
Consent for Publication
Informed consents were obtained from all patients included in the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.