
Abstract
Background:
Laparoscopic totally extraperitoneal (TEP) inguinal hernia repair (IHR) reduces risk of injury to intraperitoneal structures. Balloon dissection is more costly and has theoretical risk of injury to the surrounding structures compared with telescopic dissection (TD). This study aims to evaluate the learning curve (LC) for TEP IHR with TD of a single surgeon.
Methods:
This is a 3-year retrospective cohort study from January 2020 to December 2022 on patients who underwent elective laparoscopic TEP unilateral IHR with TD. Exclusion criteria were recurrent inguinal hernia. Cumulative sum (CUSUM) analysis was performed to evaluate the number of cases required to surmount the LC, that is, NLC for operating time (OT) and open conversion. One way analysis of variance was used to perform groupwise comparison.
Results:
There were 69 patients who underwent laparoscopic TEP unilateral IHR with TD. The median age was 58.0 years (range 24.0–80.0) and body mass index was 23.0 (range 18.6–30.0). Majority of the hernia was indirect (n = 48, 69.6%). The median OT was 70 minutes (range 35–210). Three cases (4.3%) had open conversion. One-year recurrence was 4.2% (n = 1/24). CUSUM analysis showed improvement in OT after the eighth case. However, this was followed by multiple inflection points with no apparent stabilization in OT. Pairwise comparison showed a decrease in OT between cases 18–36 and cases 37–54. There was no incidence of open conversion until the 56th case.
Conclusion:
Laparoscopic TEP IHR using TD is safe in the absence of a practor. A minimum of 36 cases is required to surmount the initial LC.
Introduction
Laparoscopic totally extraperitoneal (TEP) inguinal hernia repair (IHR) requires safe creation of a preperitoneal working space. This can be performed either through balloon dissection (BD) or telescopic dissection (TD).1,2 BD is commonly used for beginner surgeons performing TEP IHR during the learning curve (LC) due to its ease of use. 3 However, this approach is associated with complications such as bleeding, peritoneal laceration, and even bladder rupture as one is unable to fully control the manner with which the balloon dissects tissues during expansion. 4 TD, on the contrary, creates the preperitoneal space under direct visualization, and hence, dissection can be performed safely while avoiding the aforementioned complications with BD. 5
Performing TEP IHR with the TD technique requires detailed knowledge of the extraperitoneal inguinal anatomy and is more difficult to master compared with BD during the LC. 5 However, there is still a paucity of studies analyzing the nature of the LC, the exact learning model, and the number of repetitions needed to become sufficiently skilled at this technique. The primary aim of this study was to investigate the LC of a single surgeon at the beginning of the LC performing the laparoscopic TEP IHR with TD without any supervision through the use of cumulative sum (CUSUM) control chart analysis.
Materials and Methods
This is a retrospective cohort study on patients who underwent elective TEP IHR using TD between January 2020 and December 2022 by a single consultant surgeon at a university-affiliated tertiary hospital in Singapore. The study was performed from a prospectively held database. Written consent was taken from each patient for both laparoscopic repair and open Lichtenstein hernia repair in the event open conversion was necessary.
Inclusion criteria were patients with unilateral inguinal hernia. Exclusion criteria were patients who underwent TEP IHR with BD, transabdominal preperitoneal (TAPP) repair, previous IHR with recurrence, bilateral IHR, emergency admission for complicated inguinal hernia, and age <18 years. For all patients who presented with inguinal hernia, both open and laparoscopic surgeries were offered. For patients who had a history of abdominal surgery, open and laparoscopic TEP IHR was offered. For elderly patients with multiple comorbidities, or had large and/or incarcerated hernia, open repair was offered. Decision for TEP IHR with TD or BD, or TAPP IHR was based on surgeon's preference in view of comparable postoperative outcomes. 6
All surgeries were performed by a single surgeon (M.W.O.) who had adequate experience with laparoscopic appendicectomy and cholecystectomy, and at least 10 cases of TEP IHR with BD before the start of the study. The conduct of this study is in accordance with the STrengthening the Reporting of OBservational Studies in Epidemiology (STROBE) statement for observational studies. 7 This study was approved by our local institutional review board (NHG DSRB Ref. No: 2023/00080).
Study variables and outcomes
Study variables collected include age, sex, body mass index, type of inguinal hernia, operating time (OT), intraoperative complications (injury to spermatic or inferior epigastric vessels, injury to spermatic cord structures, entry into peritoneum, open conversion), immediate postoperative complications (pain score on postoperative day (POD) 1 and acute retention of urine, seroma or hematoma formation, wound infection, and early recurrence within 30 days), and long-term outcomes at 1-year follow-up (chronic pain, seroma, hematoma, and recurrence). Any swelling in the inguinal region was verified by clinical examination and ultrasound imaging to ascertain the presence of seroma, hematoma, or recurrence. The operation time was defined as the time from skin incision to skin closure. The presence of chronic pain during follow-up was defined as a pain score of more than 0 on the visual analogue scale.
Most patients were discharged from hospital on the same day as the surgery, however, if they stayed overnight in the hospital, then the length of stay was calculated as the number of days in the hospital after surgery. All patients were reviewed 1 month after operation and subsequently 1 year later. Patients who failed to turn up for clinic review were contacted by telephone, if they were still unable to be reached then the last recorded follow-up data were used for analysis. Our primary outcome was the number of cases required to overcome the learning curve (defined as NLC) for OT. Our secondary outcomes were the NLC for open conversion, as well as intra- and postoperative complication rates.
Operative technique
All surgeries were performed under general anesthesia with patients having emptied their bladders prior. A paraumbilical skin incision was made on the contralateral side of the inguinal hernia and the anterior rectus sheath was incised. The rectus muscle was retracted laterally and a 10 mm blunt trocar was inserted above the posterior rectus sheath aiming toward the pubic symphysis. A preperitoneal space tunnel was created in between the rectus abdominis muscle and peritoneum (Fig. 1A). This preperitoneal space was then insufflated with carbon dioxide to a pressure of 12 mmHg. Two additional 5-mm working ports were inserted in the midline, one 3 cm above the pubic symphysis and the other midway between the umbilicus and previously placed working port. Careful dissection in the space of Retzius was first performed with endoscissors to expand the retropubic extraperitoneal space (Fig. 1B).

Intraoperative photographs showing
Cauterization of small capillary vessels was performed to ensure meticulous hemostasis and keeping the field clear of blood. Dissection was then carried laterally toward the space of Bogros. The inferior epigastric vessels were identified and ensured that they were kept firmly against the posterior surface of rectus muscle and not displaced inferiorly toward the peritoneal surface. Once both spaces were fully dissected, attention was then focused on dissection of the peritoneal sac away from cord structures in cases of indirect inguinal hernia or complete reduction from the abdominal wall defect in cases of direct inguinal hernia (Fig. 1C). During dissection, any rents encountered in the peritoneum were secured with endoclips or suturing.
After complete peritonealization of the hernia sac, a 15 × 10-cm-sized macroporous polypropylene mesh (Ultrapro, Ethicon, LCC) was inserted and with sufficient coverage of all myopectineal orifices (Fig. 1D). Fixation of the mesh was performed using various fixation techniques; tacker (AbsorbaTack™ Covidien, Mansfield, MA, USA) was used in the majority of cases—2 tacks were placed along the inferior edge of the mesh to the pubic bone/pectineal ligament and another 2 tacks were placed laterally in the upper-outer quadrant of the mesh at least 3–4 cm above the ilio-pubic tract to avoid any injury to the nerves. The mesh was held in place as the space was deflated.
Statistical analyses
All categorical variables were described as n (%) and all continuous variables were described as median (range) unless otherwise specified. While only patients with unilateral inguinal hernia were included for the analysis of LC, baseline demographics of all patients were included in our results as well. CUSUM analysis was used for analysis of the LC for this study. CUSUM analysis allows for visual detection of chronological and consistent changes in data, done by the calculation of sequential differences between the individual data (i.e., outcome variable of the particular case number) and the average value. For this study, OT was used for CUSUM analysis and was defined as
For open conversion (binary variable), CUSUM was defined as
Results
Baseline demographics and clinical profile
There were a total of 117 patients who underwent laparoscopic IHR during this study period. There were 27 patients (23.1%) with bilateral inguinal hernia. The majority of patients underwent TEP IHR (n = 106, 90.6%). For patients who underwent TEP IHR, BD was used for 32 patients. Median OT was 70 minutes (range 35–210 minutes) for unilateral IHR, and 90 minutes (range 60–180 minutes) for bilateral IHR. Sixty-nine patients who received laparoscopic TEP, unilateral IHR with TD was included in the final analysis for evaluation of the LC. The overall patient demographics are summarized in Table 1 for both the overall cohort and those included in the final analysis only.
Clinical Demographics of All Patients Who Underwent Laparoscopic Inguinal Hernia Repair and Laparoscopic Totally Extraperitoneal Repair with Telescopic Dissection
ASA, American Society of Anesthesiologists; IHR, inguinal hernia repair; TAPP, transabdominal preperitoneal; TD, telescopic dissection; TEP, totally extraperitoneal.
Clinical outcomes
The overall cohort had four cases (3.4%) with open conversion, while the final included cohort had three cases (4.3%) with open conversion: the first case had a sliding hernia and the sac contents were unable to be fully reduced into the abdomen; the second case had a large indirect sac, which was densely adherent to surrounding tissues and had several tears within the sac; and the third case had a large indirect hernia sac and there was inadvertent injury to the inferior epigastric artery during dissection of the sac.
The overall cohort and final included cohort had 89 patients (76.1%) and 55 patients (79.7%), respectively, who completed follow-up at the 1-year interval. There was one patient who had recurrence at 1-year follow-up in both the overall cohort and final included cohort. Intraoperative characteristics and postoperative outcomes of both the overall cohort that underwent laparoscopic IHR, and the final included cohort that underwent laparoscopic TEP unilateral IHR with TD are summarized in Table 2. In the TEP unilateral IHR with TD cohort, we obtained good postoperative outcomes with no incidence of seroma, hematoma, and scrotal swelling at 1-year follow-up. There were 4 patients (7.3%) who reported chronic pain at the 1-year follow-up.
Intraoperative and Postoperative Outcomes of All Patients Who Underwent Laparoscopic Inguinal Hernia Repair and Laparoscopic Totally Extraperitoneal Repair with Telescopic Dissection
IHR, inguinal hernia repair; POD1, postoperative day 1; TD, telescopic dissection; TEP, totally extraperitoneal.
LC analysis
CUSUM analysis was performed on consecutive laparoscopic TEP unilateral IHR with TD (n = 69) to assess the LC. Figure 2 shows the CUSUMOT for all included cases. There was a steady increase in CUSUMOT until case 8, where there was a subsequent downtrend from the case 9 to case 17. There were five inflection points in total—case 8 (uptrend to downtrend), case 17 (downtrend to uptrend), case 36 (uptrend to downtrend), case 54 (downtrend to uptrend), and case 60 (uptrend to downtrend). There was a significant difference in OT when comparing across six groups based on the inflection points noted on the CUSUM graph.

CUSUM curve evaluating changes in OT with each case. CUSUM, cumulative sum; OT, operating time.
Pairwise comparison between those groups showed a significant difference in OT between cases 9–17 versus 18–36 (increase in OT; adjusted P = .026), 9–17 versus 55–60 (increase in OT; adjusted P = .021), and 18–36 versus 37–54 (decrease in OT; adjusted P = .005). Further analysis was made to compare the mean OT across the new groups made based on the arbitrary regrouping of cases in view of the unstable LC (Table 3).
Comparison of Mean Operating Time Between Phases of Learning Curve Identified Using Cumulative Sum Analysis and Between Phases of Learning Curve Regrouped Using the Initial Cumulative Sum Analysis
Bold number indicates that P value was significant as it was <0.05.
P-value was obtained using independent sample t-test in the presence of two groups, and one-way ANOVA in the presence of more than two groups.
ANOVA, analysis of variance; OT, operating time.
Open conversion occurred for cases 56, 60, and 65. While CUSUM analysis (Fig. 3) showed a steady decrease in NLC until case 56, which may be a possible inflection point, the number of cases of open conversion is too low to make any definitive conclusion on the NLC for open conversion. Hence, based on our results, we did not establish an LC for open conversion in laparoscopic TEP unilateral IHR with TD.
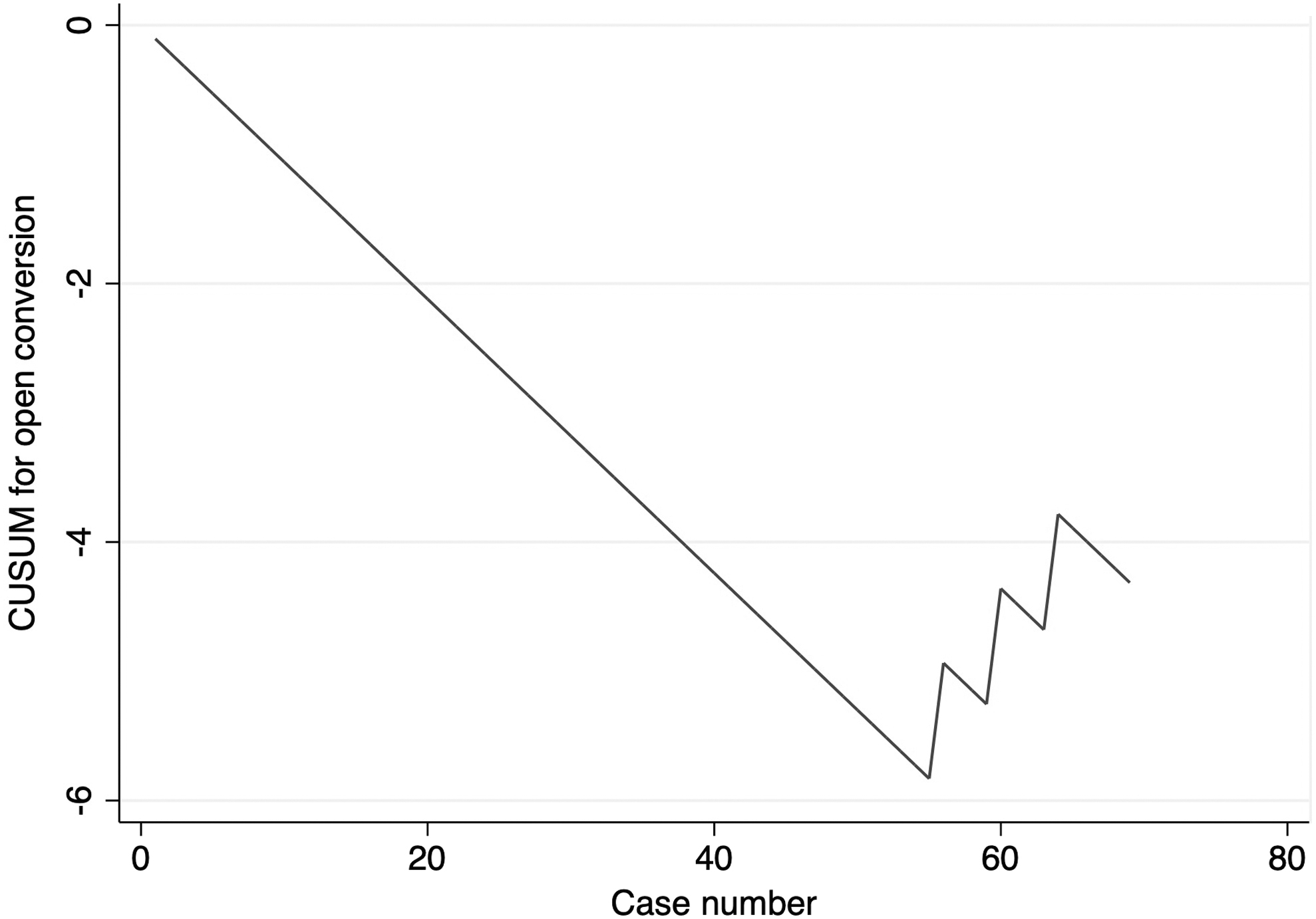
CUSUM curve evaluating changes in incidence of open conversion with each case. CUSUM, cumulative sum.
Discussion
LC has been defined as the minimum number of operations required for gaining sufficient knowledge of technical factors and understanding of operative pitfalls, which leads to improvement and eventual stabilization of operation times and complication rates.9,10 However, existing literature reporting on the NLC for laparoscopic TEP IHR is highly variable, ranging from 20 to 400.11–16 To add on, there are even fewer articles reporting on the LC for TD,12,14 as BD has been associated with reduced OT and open conversion rates (and hence possibly a more popular approach). 2 Hence, our study is important to fill in the lacuna in literature on the NLC for laparoscopic TEP IHR with TD; we demonstrated that a minimum of 36 cases were required to overcome the initial LC.
Laparoscopic IHR has now largely replaced open repair for most inguinal hernia with reduced postoperative pain and time to return to work, yet with similar long-term recurrence and chronic pain incidence. 17 Unlike TAPP IHR, TEP IHR has reduced risk of injury to the intra-abdominal organs and risk of forming adhesions, but requires a longer OT due to the smaller working space. 18 The extraperitoneal space in TEP IHR may be created using BD or TD; BD allows the creation of an extraperitoneal space through the use of insufflation without direct vision and has been shown to reduce OT. 2
However, BD is more costly compared with TD, and has an added theoretical risk of injury to the inferior epigastric vessels and bladder due to the lack of direct vision and controlled expansion of the balloon in the extraperitoneal space. 19 TD allows for careful and controlled dissection under direct vision and has been shown to be safe compared with BD. 20 This raises the need for studies to evaluate the LC for laparoscopic TEP IHR with TD.
Our study showed that there is an initial NLC of eight cases for laparoscopic TEP IHR with TD. However, the OT did not stabilize thereafter. CUSUM analysis on OT showed that eight cases were required to overcome the initial LC for TEP unilateral inguinal repair with TD (Fig. 2). The LC for surgical practice was described by Hopper et al. 21 ; it can be divided into the following five phases: (1) initial rapid improvement in performance with a gradual decrease in the extent of improvement, (2) continued improvement (although slower) with ability to perform the procedure independently and competently, (3) small improvements in performance, (4) plateau in performance, and (5) fall in performance due to advanced age or deterioration in surgeon dexterity, eyesight, or cognition.
The initial rapid improvement in OT up till the eighth case is likely due to the rapid acquisition of skills on the use of TD in TEP IHR as the surgeon had prior experience in TEP IHR with BD. Existing reviews on the LC in pancreaticoduodenectomy, esophagectomy, and total gastrectomy showed that prior experience in laparoscopic surgery reduces the NLC for new techniques, for example, robotic surgery.22–24
However, this rapid improvement in OT was followed by multiple inflection points with increasing and decreasing OT with no apparent stabilization. We believe the first increase in OT (inflection point at case 17) to be due to modifications in our surgical technique with more care taken during dissection. This was made after learning from the first few cases, where there was inadvertent entry into the peritoneum. Experience with careful dissection transited to improvement in OT (inflection point at case 36). With more experience in TEP IHR with TD, the surgeon expanded his selection criteria and included more challenging cases (e.g., patients with larger hernia defects and incarcerated hernias); this corresponds with the second increase in OT (inflection point at case 54) and our first case of open conversion.
This trend of improvement in outcome, followed by subsequent worsening of outcome, was similarly identified in studies exploring the LC in other minimally invasive surgeries. For instance, Zhu et al. studied the LC in video-assisted McKeown esophagectomy and demonstrated a decrease in recurrent laryngeal (RLN) palsy rates after the initial 72 cases, followed by a subsequent increase in RLN palsy after 151 cases. 25 The authors explained the downward trend (cases 73–151) in RLN palsy to be due to reduced lymph node dissection in view of high incidence of RLN palsy experienced prior. The subsequent upward trend in RLN palsy was due to increased lymph node dissection (although overall RLN palsy during that period remains low). In view of the multiple phases of LC reported in our study with no apparent stabilization, it is difficult to draw a definitive conclusion on the exact NLC required to surmount the LC.
Therefore, we combined the six phases into various groups and performed pairwise and/or intergroup comparisons to explore significant differences in OT (Table 3). There was a significant decrease in OT between cases 18–36 and cases 37–54, with a subsequent increase in OT between cases 37–54 and cases 55–60. As described in our results, the subsequent increase is likely due to the inclusion of more challenging cases, as evident by our first incidence of open conversion at case 56. While there was subsequently a decrease in OT between cases 55–60 and cases 61–69, this was not statistically significant (adjusted P = .110), which may be due to the small sample size. Based on the above analysis, a minimum of 36 cases is required to surmount the LC.
Patient selection is important for any surgical procedure and is of even greater emphasis during the initial phase of learning. It is impractical and unethical to include difficult cases during the early phase of learning as patients may be subjected to increased morbidity. It is recommended that a beginner surgeon starting out on TEP IHR should select patients who are relatively younger, less than 60 years old, of thin build, with unilateral, nonscrotal primary inguinal hernia. 26 Other studies evaluating the LC of other surgeries similarly raised concerns that case selection is a confounding factor that unfortunately cannot be adjusted for. 27
Proctorship and apprenticeship are key aspects of surgical training; surgery has traditionally been taught using “see one, do one, teach one.” 28 In the process of teaching, it is also important for the proctor to pass down technique modifications, which he or she has used to ease the steep LC of surgical training. For instance, a study by van der Sluis et al. evaluating the NLC in minimally invasive esophagectomy showed that the NLC for improvement in operating was 70 cases for the proctor, but only 24 cases for the trainee. 29
In our study, we analyzed the LC of a single surgeon with prior experience in laparoscopic surgery, and at least 10 cases of TEP IHR with BD. The NLC obtained from our study may be longer compared with other studies in the presence of a proctor. In addition, with the increase in accessibility to the internet, surgeons may refer to user-uploaded videos for reference to provide a mental imagery, which may also ease the steep LC. 30
Our series showed a 1-year recurrence of 1.8% (n = 1/55), which is comparable with internationally reported standards of 0–3.5%.18,31–34 This demonstrates the safety and feasibility of TEP IHR with TD even during the initial LC without a proctor. We believe that the cause of recurrence was due to the inadequate coverage of the mesh of the direct hernia; it is recommended to have at least 4–5 cm medial coverage of the direct defects from the direct edge to reduce risk of recurrence.35,36 However, readers should also note that not all the patients completed their follow-up at the 1-year interval. Further data should be reported. Lamb et al. who similarly studied on the LC of laparoscopic TEP IHR showed that recurrence occurred in 10% of a surgeon's first 20 cases, 4% of the next 60 cases, and falling to below 2% thereafter. 37
Low recurrence and conversion rates should prioritize over OT for any inexperienced surgeon beginning the LC for TEP IHR with TD. Implementation of a safe training algorithm in the presence of a proctor should be considered; Hannan et al. demonstrated safe training for surgical trainees starting on laparoscopic TEP IHR with the use of a structured training algorithm with similar postoperative outcomes, including recurrence, except for OT (longer for trainees compared with consultants). 38
Our study has its limitations. First, this is a retrospective cohort study with inherent selection bias. However, this was reduced with the use of clearly defined exclusion criteria to limit heterogeneity of our study (single-surgeon study with inclusion of only unilateral, nonrecurrent inguinal hernia). In addition, data on comorbidities and history of abdominal surgery were not collected. In the case of IHR, other outcome long-term outcome variables such as 5-year recurrence are also important. A longer follow-up period is required for this, for which data are being collected and will be published for subsequent studies.
Conclusion
Laparoscopic TEP IHR using TD is safe and feasible in the absence of a proctor for an inexperienced surgeon. Our results demonstrated that a minimum of 36 cases is required to surmount the LC. However, with the inclusion of more technically challenging cases in our LC, this resulted in an increase in OT in the later cases. Further studies with a larger sample size are required to further evaluate the LC. In addition, long-term outcomes such as recurrence and chronic pain are important outcomes of IHR and should be evaluated in future studies.
Footnotes
Authors' Contributions
K.S.C.: Conceptualization, methodology, software, validation, formal analysis, investigation, and writing—original draft. J.L.: Validation, investigation, resources, data curation, visualization, and supervision. M.W.O.: Conceptualization, methodology, investigation, resources, data curation, writing—review and editing, visualization, supervision, and project administration.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.