
Abstract
Objective:
To investigate the impact of metabolic syndrome (MetS) on short-term complications of laparoscopic pancreaticoduodenectomy (LPD).
Materials and Methods:
We retrospectively analyzed perioperative data of patients who underwent LPD in our department from January 2020 to January 2022. The patients were divided into the MetS group and non-MetS group based on whether they had MetS. The incidence of postoperative complications and mortality rate was compared between the two groups.
Results:
The study involved 279 patients, with 30 having MetS and 249 without. However, the MetS and non-MetS groups differed significantly in terms of postoperative pancreatic fistula rate (26.6% versus 8.4%), abdominal infection rate (33.3% versus 10.0%), pulmonary complications rate (16.7% versus 6.42%), Clavien–Dindo ≥3 rate (20% versus 8.0%), multiple complications rate (23.3% versus 9.6%), percutaneous drainage rate (33.3% versus 10.0%), 90-day mortality rate (6.7% versus 1.2%), and length of postoperative hospital stay (15.00 ± 12.78 versus 10.63 ± 5.23 days). However, the two groups differed no significantly with respect to age, gender, American Society of Anesthesiologists score, preoperative CA125/CA199 levels, surgery time, specimen removal time, and intraoperative blood loss.
Conclusion:
MetS increases the incidence of postoperative complications and perioperative mortality rate in LPD.
Introduction
Pancreatoduodenectomy (PD), often considered as the crown of general surgery, is a complex procedure involving multiple organs. Its intricate surgical steps and the involvement of various anatomical structures contribute to a significant risk of postoperative complications. In the past decade, significant advancements in perioperative management and the growing expertise of surgeons have resulted in the widespread adoption of laparoscopic pancreaticoduodenectomy (LPD) as a novel procedure in major pancreatic surgery centers both domestically and internationally. The perioperative mortality rate has significantly decreased, but the incidence of complications remains high, including pancreatic fistula, bleeding, and delayed gastric emptying (DGE). 1 According to clinical oncology research reports, the incidence of pancreatic cancer has been on the rise due to increased social life stress and changes in dietary habits. 2 As the social standard of living improves, an increasing number of individuals are affected by underlying conditions such as hypertension, diabetes, hyperlipidemia, and obesity, collectively known as metabolic syndrome (MetS). Therefore, there is a growing population with MetS undergoing PD.
MetS is characterized by the presence of three or more of the following criteria: increased waist circumference or overweight/obesity, arterial hypertension, decreased serum high-density lipoprotein (HDL) cholesterol, increased serum triglycerides, and diabetes mellitus (DM) or increased fasting glucose levels. 3 Although there is no universally accepted set of diagnostic criteria for MetS, it is generally acknowledged that the diagnosis is confirmed when three or more of the aforementioned criteria are present. MetS not only increases the risk of cardiovascular diseases and nonalcoholic fatty liver disease but also leads to immune imbalance and dysbiosis of gut microbiota, thereby increasing the incidence of perioperative complications.4,5
Previous studies have reported that patients with MetS undergoing liver resection have a several-fold higher incidence of perioperative complications and mortality compared to the general population.6–8 Therefore, in this study, we conducted a retrospective review of perioperative data from patients who underwent LPD between January 2020 and January 2022 at a single center, aiming to investigate the impact of MetS on short-term complications of LPD.
Materials and Methods
Study population
A retrospective analysis was conducted from January 2020 to January 2022. In light of the retrospective nature of our study, we were granted an exemption from the requirement of obtaining ethical committee approval. Inclusion criteria were as follows: (1) patients have no contraindications for surgery and able to tolerate anesthesia; (2) preoperative imaging examination indicates that the tumor is resectable; (3) complete perioperative clinical data. The exclusion criteria were as follows: (1) intraoperative exploration revealing tumors that were deemed unresectable and requiring palliative treatment; (2) intraoperative conversion due to various reasons; (3) missing case data.
From January 2020 to January 2022, a total of 314 patients underwent LPD. Of those, we excluded patients with missing data (n = 21), patients who received palliative surgical interventions (n = 8), patients who underwent surgical conversion due to various reasons (n = 6). Lastly, in total, there are 279 patients included in this study (Fig. 1).
Flow chart of cohort creation.
Based on preoperative clinical data, the patients were divided into two groups: the “metabolic syndrome” group (30 cases) and the “nonmetabolic syndrome” group (249 cases). The definition and diagnosis of MetS followed the criteria of meeting three out of the following five items: (1) abdominal obesity (body mass index [BMI] >28.8 kg/m2); (2) fasting triglycerides >150 mg/dL; (3) fasting HDL <1.04 mmol/L; (4) type 2 diabetes (fasting blood glucose >6.1 mmol/L); (5) hypertension (blood pressure >130/85 mmHg). 9
Surgical procedure and perioperative management
All patients underwent LPD for tumor resection. Simultaneously, a lymph node dissection was performed in the corresponding tumor region, and the digestive tract reconstruction was performed using the Child method. Pancreaticojejunostomy was performed using the “modified double purse-string suture” technique. After completing the digestive tract reconstruction, abdominal drainage tubes were placed in the anterior and posterior aspects of the pancreaticojejunostomy and near bilioenteric anastomosis site. Postoperatively, all patients received acid suppression, enzyme inhibition, gastrointestinal decompression, anti-inflammatory drugs, and fluid therapy. On the first postoperative day, abdominal ultrasonography was performed, followed by abdominal CT on the second postoperative day. If no fluid accumulation was observed on the imaging studies, early removal of the drainage tubes was performed.
Study variables
The data collected for analysis encompassed a comprehensive set of preoperative, intraoperative, and postoperative variables. Patient demographics, including age, gender, BMI, American Society of Anesthesiologists (ASA) classification, CA125, CA199, and diabetes, were meticulously recorded. Intraoperative and postoperative data comprised crucial information such as surgical resection time, estimated blood loss, transfusion requirements, incidence of postoperative pancreatic fistula (POPF), bile leakage, DGE, postoperative hemorrhage, 30-day mortality, 90-day mortality, re-operation rates, Clavien–Dindo classification ≥grade III, and duration of postoperative hospital stay.
The grading and definitions for POPF, hemorrhage, and DGE were based on the corresponding guidelines.10–12 Perioperative mortality was defined as death within 30 days after the surgery. The diagnosis of intra-abdominal infection was based on the consensus of experts on the diagnosis, treatment, and prevention of common postoperative complications in pancreatic surgery, while the diagnosis of pneumonia was based on clinical manifestations and imaging examination results. 13 Preoperative non-alcoholic fatty liver disease (NAFLD) was determined by CT or MRI scans, whereas new, postoperative NAFLD was determined by color Doppler ultrasound examination
Statistical analysis
Data analysis was performed using SPSS 22.0 statistical software. The data were categorized into two types: continuous variables and categorical variables. For continuous variables that followed a normal distribution, descriptive statistics such as mean (x) ± standard deviation (s), and t-test were used. For continuous variables that did not follow a normal distribution, median and interquartile ranges were used, and nonparametric tests such as the Mann–Whitney U test were employed.
Categorical variable data were analyzed using the chi-square test. Univariate and multivariate logistic regression was used to evaluate the association between MetS and primary outcomes.
Results
Patients' characteristics
Among them, 171 (61.29%) were male, with a median age of 60 years. Among these patients, 30 cases (10.75%) were diagnosed with MetS and were classified as the MetS group.
Two groups of patients showed no significant differences in age, gender, ASA classification, and preoperative indicators such as CA125 and CA199 (all P > .05). However, there were significant differences between the two groups in terms of preoperative BMI, triglyceride levels, and the presence of DM (Table 1).
Demographic Characteristics of Those People Who Underwent Laparoscopic Pancreaticoduodenectomy
ASA Classification, American Society of Anesthesiologists classification; BMI, body mass index.
Surgical outcomes
There were no statistically significant differences between the two groups in terms of surgical time, specimen resection time, intraoperative blood loss, and DGE (P > .05); however, the incidence of nonalcoholic fatty liver disease combined with MetS is significantly higher than that of the non-MetS group, and the difference between the two is statistically significant (Table 2). Furthermore, statistically significant differences were found between the two groups in terms of postoperative POPF, intra-abdominal infection, pulmonary complications, Clavien-Dindo ≥3, multiple complications, 90-day perioperative mortality, and failure to rescue, lower extremity vein thrombosis (all P < .05) (Table 3 and Fig. 2).
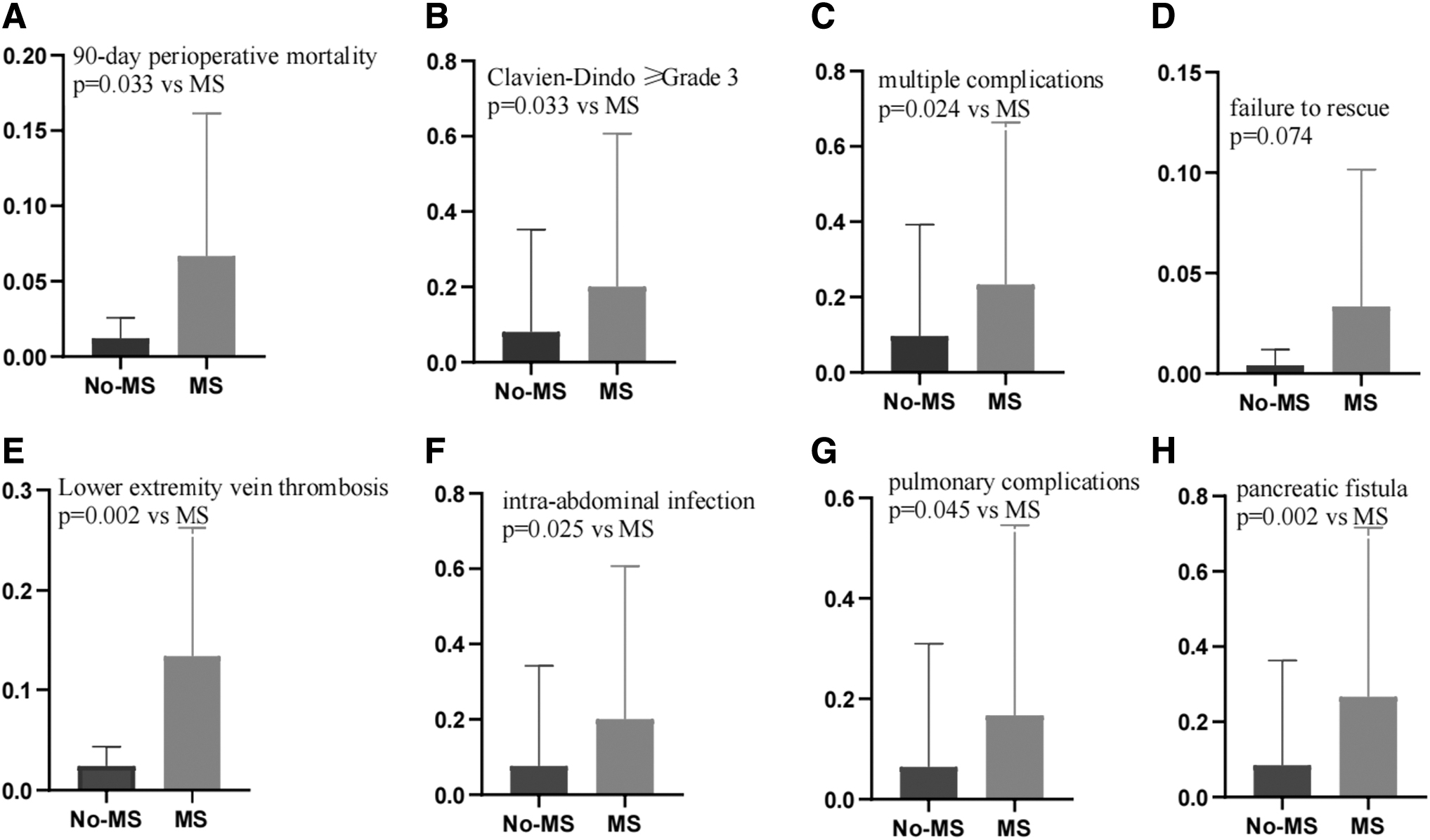
Representative percentages of significant outcomes of patients with and without MS.
Comparison of Various Data Between the Two Groups
Comparison of Postoperative Various Data Between the Two Groups
The relationship between MetS and postoperative complications
We performed additional analysis using logistic regression to identify the risk factors associated with postoperative POPF after LPD. Univariate analysis revealed several significant risk factors for the occurrence of POPF following LPD, including the presence of multiple complications, Clavien–Dindo ≥3, pancreatic duct diameter, re-operation, and the presence of MetS. In the multivariate analysis, it was determined that re-operation did not pose as an independent risk factor. However, multiple complications, Clavien–Dindo ≥3, pancreatic duct diameter, and MetS were identified as independent risk factors (all P < .05) (Table 4).
multivariate Regression Analysis of Pancreatic Fistula
On multivariate analysis, MetS was associated with increased multiple complications (≥2), nonalcoholic fatty liver, and intra-abdominal infection, and lower extremity vein thrombosis and pancreatic fistula (Table 5). The association of MetS and 90-day perioperative mortality, pulmonary complications approached statistical significance (P = .059and P = .054). The associations of MetS with Clavien–Dindo ≥3, re-operation, perioperative bleeding, DGE, 30-day perioperative mortality, and failure to rescue were not significant on multivariate analysis.
Multivariable Analysis of Metabolic Syndrome Contributing to Primary Outcomes
Discussion
MetS, which includes insulin resistance, obesity, dyslipidemia, hypertension, and impaired glucose tolerance, poses a significant problem for public health. Not only does it jeopardize individuals' well-being, but it also results in increased health care expenses for society. As living standards improve, this condition is becoming more prevalent in the general population, with an incidence rate of ∼20%. Among individuals with obesity, the proportion can be as high as 60%. 14
With the increasing incidence of MetS and periampullary tumors, an increasing number of patients are undergoing PD with MetS. Multiple studies have provided evidence that MetS contributes to a higher occurrence of postoperative complications and perioperative mortality across various surgical procedures.15,16 Bhayani et al. found that patients with MetS undergoing liver partial resection faced a 1.4-fold increase in the risk of perioperative complications and a 2.7-fold increase in the risk of mortality. 17 Furthermore, Zavlin et al. reported a significantly heightened risk of perioperative mortality among patients with MetS undergoing plastic surgery. 18
Obesity is one of the main manifestations of MetS. Multiple studies have indicated that patients with concomitant obesity undergoing LPD often experience increased intraoperative blood loss and a higher probability of postoperative complications such as POPF, intra-abdominal infection, pneumonia, and wound infection. Additionally, their hospital stay tends to be longer.19,20 Moreover, conditions such as hyperglycemia, hypertension, and hyperlipidemia not only disrupt the function of vascular endothelial cells and lead to secondary vascular diseases but also increase the risk of postoperative bleeding. Patients with MetS often lack physical activity and exhibit lipid abnormalities, resulting in overweight or obesity and long-term hyperglycemia, which can lead to impaired immune function, decreased neutrophil count, and disturbances in the internal environment, making them more susceptible to postoperative infections. Schumann et al. found a significant correlation between MetS and postoperative pulmonary complications, particularly respiratory failure and acute respiratory distress syndrome.
Compared to patients without MetS, those with MetS had significantly higher mortality rates at 30 and 90 days postoperatively. 21 In this study, we have further substantiated that MetS not only prolongs hospitalization after surgery but also elevates the risks of POPF, postoperative intra-abdominal infection, nonalcoholic fatty liver disease, pulmonary complications, Clavien–Dindo ≥3, multiple complications (≥2), and 90-day mortality. These findings are consistent with reports from the majority of researchers.22,23
Similarly, MetS is also linked to thrombotic events. It remains uncertain whether the elevated risk of thrombotic events is primarily attributed to MetS or other reasons. Our study revealed a higher incidence of lower extremity intermuscular vein thrombosis in the MetS group compared to the non-MetS group. Therefore, for patients with MetS, surgeons should implement precise stratified and individualized management, based on perioperative indicators, to determine whether prophylactic anticoagulant treatment is necessary.
Compared to other centers, 22 both groups in our study had a similar perioperative mortality rate of around 3%. However, our center had a slightly higher incidence of pancreatic fistula (26.6% versus 12.8%) and percutaneous drainage (31.25% versus 13.3%), but a slightly lower rate of unsuccessful rescues (3.3% versus 10.4%) and reoperation (3.3% versus 5.0%). Our center's lower perioperative mortality and reoperation rates can be attributed to our regular use of abdominal imaging during the early postoperative period (within the first 3 days) to detect pancreatic fistula and abdominal fluid accumulation for timely intervention. This may also explain why our incidence of percutaneous ultrasound-guided drainage is higher. Furthermore, the higher incidence of pancreatic fistula in our center could be due to the smaller number of patients with MetS included in our study.
In summary, patients with MetS experience significantly higher rates of perioperative complications and mortality compared to those without MetS, and these differences are statistically significant. The occurrence of postoperative complications not only poses a risk to patients' safety but also leads to increased health care expenses for society. Therefore, it is essential to accurately regulate and manage various risk factors based on patient conditions before surgery. Additionally, implementing stratified and refined management approaches after surgery is crucial to reduce the incidence of perioperative complications.
Footnotes
Acknowledgment
We thank Y.F. who came up with the idea.
Authors' Contributions
Conception and design: Y.F., S.W. Data analysis and interpretation: Xu. W. Manuscript writing: All authors. Final approval of manuscript: All authors.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.