
Abstract
Background:
The treatment of choledocholithiasis with nondilated common bile duct (CBD) is a challenge for surgeons who often choose endoscopic retrograde cholangiopancreatography with laparoscopic cholecystectomy (LC) staging surgery instead of simultaneous laparoscopic CBD exploration with LC because of the small CBD diameter. This study aims to introduce and assess the clinical applicability of a technique we developed to identify and extract CBD stones using laparoscopic ultrasound (LUS).
Methods:
We retrospectively reviewed surgical procedures and clinical data of 13 patients who underwent LC and CBD exploration using LUS between May 2022 and August 2023. The cystic duct was used for CBD stone removal.
Results:
Ten patients were successfully treated; 2 patients with residual stones were treated with ursodeoxycholic acid, whereas 1 patient required a microincision near the CBD and choledochoscopy because of stone incarceration in the duodenal papilla. The CBD diameter was 6 mm (5–9 mm). There were less than three CBD stones, with diameters of 2–6 mm; the median operative time was 105 minutes (range, 52–155 minutes). One patient developed postoperative cholangitis. The median postoperative hospital stay was 6 days (3–8 days). The stone clearance rate was 76.9%, and the CBD stone detection rate was 100%. No intraoperative complications, postoperative bile leakage, and mortality occurred.
Conclusions:
CBD exploration and transcystic stone extraction under LUS guidance are safe and effective approaches for patients with choledocholithiasis; strict control over surgical indications is necessary. This study could provide new strategies for effectively treating choledocholithiasis.
Introduction
Cholelithiasis is a prevalent digestive tract disease, and 10%–20% of patients with gallstone are complicated with choledocholithiasis.1–3 Various treatments are available for common bile duct (CBD) stones, including endoscopic retrograde cholangiopancreatography (ERCP) and laparoscopic cholecystectomy (LC) after stone extraction (the “two-stage” approach) and simultaneous laparoscopic CBD exploration and LC (the “single-stage” approach), each with specific indications. However, in clinical practice, most patients with small-diameter CBD stones have less obvious CBD dilatation, challenging traditional laparoscopic CBD exploration (LCBDE), and increasing surgical difficulty. Nondilation of the CBD makes indwelling of the T-tube difficult and increases the incidence of postoperative biliary stricture and bile leakage.4–5 Surgeons often opt for ERCP and LC to alleviate this burden at the cost of increasing the physical and economic pressure on patients.6–8 Although laparoscopic transcystic CBD exploration (LTCBDE) can solve some of these problems, 9 the lack of small-diameter choledochoscopes in many hospitals limits its application.
To address this issue, we aimed to examine a novel method that combines laparoscopic ultrasound (LUS) examination with a wire basket through the cystic duct to enable simultaneous detection and stone removal. By emphasizing the experience and precautions for this surgical method, this study could help develop new strategies for improving CBD stone treatment.
Materials and Methods
Patients
This study retrospectively analyzed the clinical data of 13 patients who underwent CBD exploration and CBD stone removal using the cystic duct approach combined with LUS at the Minimally Invasive Treatment Center of Hepatobiliary and Pancreatic Surgery in Wuhan Central Hospital between April 2022 and August 2023. All patients underwent simultaneous LC. This study was approved by the Ethics Committee of Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology (Approval no.: WHZXKYL2023-142). All patients provided informed consent before surgery.
Surgical method
A four-hole surgical method was used. Trocar position is as shown in Figure 1. The patient was placed in the supine position. After anesthesia, a Veress needle puncture was performed to establish a CO2 pneumoperitoneum with a gas pressure of 12 mmHg. A 10-mm trocar was placed through an arc incision under the umbilicus. Then, a 12-mm trocar was placed under the xiphoid in the upper abdomen, a 5-mm trocar was placed in the midclavicular line 1–2 cm below the costal margin, and another 10-mm trocar was placed in the right abdomen 5 cm below the costal margin.

Trocar position.
The patients were placed in the reverse Trendelenburg position and tilted to the left. A wide local dissection of Calot’s triangle was performed, and the cystic duct and cystic artery were completely free and exposed to the CBD junction as far as possible. The cystic artery was then occluded and excised. The distal cystic duct was ligated using a silk thread to adjust its direction. Next, a transverse incision was made on the lateral wall of the cystic duct. The proximal cystic duct was longitudinally incised along this incision until it joined the CBD. A laparoscopic separation forceps was used to insert into the cystic duct and open the tip of the forceps to expand the cystic duct. For cases with a thin cystic duct and a high operation difficulty, we used a dilatation balloon guide wire to stretch into the cystic duct, inflated the balloon, and used the balloon to dilate the cystic duct until the bile flowed smoothly.
A LUS probe was used to conduct transverse and longitudinal exploration through the 12-mm trocar under the xiphoid and the 10-mm trocar on the right side of the abdomen to clarify the location of the stones, and then a wire basket was used to enter the CBD through the cystic duct. Subsequently, it was opened and pulled back until the stones were captured, and the stones were removed under ultrasound guidance. After stone removal, an 8 Fr infusion tube was inserted into the CBD to flush out the residue. Finally, the cystic duct stump was clamped directly. In the case of microincision technique (a small incision of the cystic duct at the confluence with the CBD with extension of only 3–5 mm), the incision was sutured intermittently, and then the cystic duct stump was clamped 2–3 mm away from the suture area. In cases where microincision technique was used and intraoperatively we found gallbladder edema or inflammatory exudates, an abdominal drainage tube was placed. Intraoperative key view during surgery is shown in Figure 2. Intraoperative ultrasound image is shown in Figure 3.
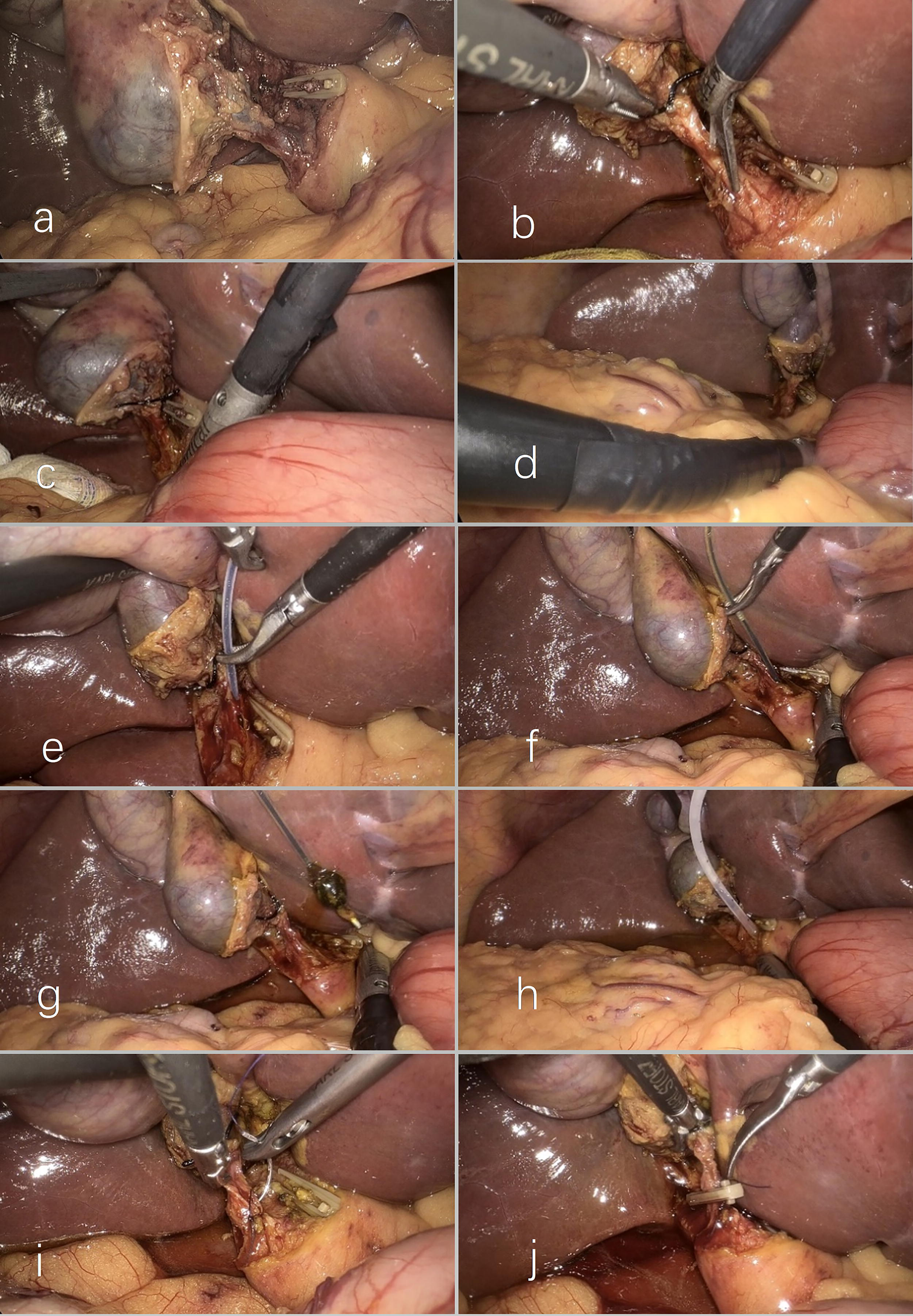
Intraoperative key view during surgery.

Intraoperative ultrasound image.
Follow-up management
We followed up with the patients after discharge. Follow-up visits were conducted at 1 month, 3 months, 6 months, and then annual follow-up; patients would come to our hospital outpatient clinic. Follow-up examinations included abdominal ultrasound, computed tomography, magnetic resonance cholangiopancreatography, and blood biochemical examinations. The purpose of the follow-up was to detect postoperative complications early and evaluate postoperative biliary function.
Results
From May 2022 to August 2023, 13 patients underwent LC and CBD exploration with LUS at our center, and CBD stones were successfully removed through the cystic duct. The patients’ characteristics are described in Table 1.
Patient Characteristics
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CBD, common bile duct; F, female; γ-GT, γ-glutamyl transpeptidase; M, male; N, none.
The median age of these patients was 59 years (23–84 years), the median preoperative total bilirubin was 15.6 µmol/L (5–79.8 µmol/L), the median preoperative aspartate aminotransferase was 42.3 U/L (7.2–621.2 U/L), and the median preoperative alanine aminotransferase was 35 U/L (18.7–605.9 U/L). The median preoperative γ-glutamyl transpeptidase was 47 U/L (6.3–453.1 U/L). Two patients (NO. 8 and NO. 12) exhibited elevated preoperative transaminase levels. No patients had preoperative pancreatitis or cholangitis. The median diameter of CBDs was 6 mm (5–9 mm), the median number of observed CBD stones was 1 (1–3), and the median diameter of the cystic duct was 5 mm (4–6mm). These data were obtained using preoperative imaging (abdominal ultrasonography, computed tomography, and magnetic resonance cholangiopancreatography), and the median maximum diameter of CBDs was 3 mm (2–6 mm). No patients had preoperative pancreatitis or cholangitis. The median operative time was 105 minutes (52–155 minutes), and the median intraoperative blood loss was 20 mL (10–50 mL).
Operative outcomes are described in Table 2. Among these patients, 11 had an abdominal drainage tube and 2 did not. The tube was removed within 3–7 days after the operation (median, 4 days). The median postoperative hospital stay was 6 days (3–8 days). Postoperative imaging examination revealed that stone removal was successful in 10 cases, residual stones were found in 2 cases (NO. 3 and NO. 7), and in 1 (NO. 10) we failed to extract the stone owing to the stone being incarcerated in the duodenum, for which we made an incision of the cystic duct at the confluence with the CBD and choledochoscope was used. The closure was sutured after the bile duct stent was indwelled. In all these cases, LUS showed clear visualization of the stones (Fig. 3), with a positive rate of 100%. The number of stones detected by intraoperative ultrasound is consistent with the findings of preoperative imaging observations. The success rate of stone removal was approximately 76.9%.
Operative Outcome
N, none; POS, postoperative hospital stay.
None of the patients had secondary injuries during the operation, and 1 patient (No. 8) developed cholangitis after the operation, which improved after symptomatic treatment with anti-infection agents, spasmolysis, and cholagogue. No complications were observed in the other patients. Two patients with residual stones had 1–2 small stones with a diameter of approximately 2 mm without clinical symptoms. The patients were treated with oral ursodeoxycholic acid and underwent regular outpatient reviews. Hepatic function assessment before discharge did not reveal any aberrations. All patients recovered smoothly and were discharged from the hospital.
We followed up with these patients for up to 4 months to 18 months after surgery and did not find any patients with complications such as biliary stricture, residual stones, cholangitis, or pancreatitis, and their quality of life was good.
Discussion
The management of concomitant cholelithiasis and choledocholithiasis is based on single- or two-stage procedures. The prevailing view is that the intraoperative extraction of CBD stones is superior to the two-stage procedure; 10 however, for patients with a small diameter and a small number of CBD stones, their CBDs are generally not dilated and without jaundice and cholangitis. In these cases, owing to the difficulty of choledochoscopic exploration, high risk of postoperative bile leakage, and biliary stricture, or the belief that intraoperative exploration of the CBD is traumatic, surgeons are forced to choose a two-stage procedure. To solve these problems, we find a new way to replace the visualization function in choledochoscopy and establish an operation channel for stone removal.
Can intraoperative ultrasound replace choledochoscopy for CBD and calculi exploration?
The laparoscopic CBD lithotomy necessitates the utilization of a choledochoscope visualization to identify the course of the biliary tract and precisely ascertain the number and location of CBD stones, facilitating their extraction under direct visual guidance to prevent biliary tract injury and ensure complete stone clearance. LUS combined with a wire basket through the cystic duct can be a viable alternative for these functions.11–17
In 1979, Professor Makuuchi from Japan first applied intraoperative ultrasonography in liver surgeries. Since then, intraoperative ultrasound has been widely used in hepatobiliary, pancreatic, and other surgical fields. According to the literature, 11 CBD LUS exploration can achieve a positive stone detection rate similar to that of cholangiography. For CBD stone detection, LUS demonstrated a positive predictive value of 100%, a negative predictive value of 99.3%, a sensitivity of 98.4%, and a specificity of 100%. Therefore, LUS can be considered as the primary imaging modality for evaluating CBD stones in laparoscopic surgery, and it has been shown to be a safe, quick, and effective method for evaluating biliary anatomy.12–14 The metal head of the stone removal basket was clearly visualized using ultrasonography (Fig. 3b), allowing precise guidance during the stone removal procedure.
How to establish a passage from the cystic duct to the CBD
The Heister’s valve on the cystic duct prevents the wire basket from entering the CBD. CBD stones are secondary in the vast majority of cases, originating from the gallbladder through the cystic duct, which damages Heister’s valve and widens the diameter of the cystic duct.18,19 This pathological process enables the removal of CBD stones through the cystic duct. The key to opening the cystic duct into the CBD is to destroy the valve. We made a longitudinal incision through the cystic duct by endoscopic scissors and used a dilatation balloon guide wire to stretch into the cystic duct and inflated the balloon to dilate the cystic duct until the bile flowed smoothly.
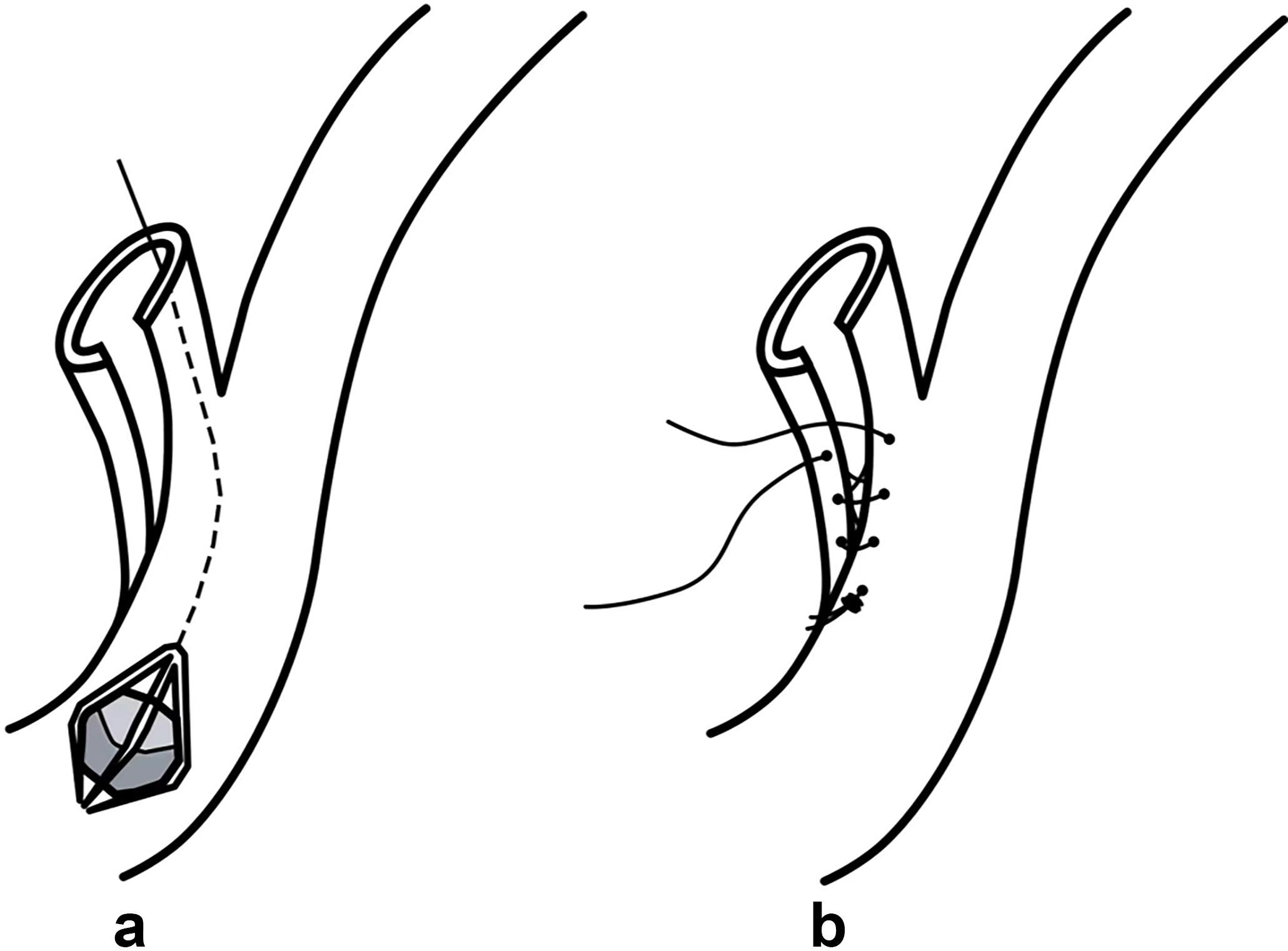
In more complex cases, a small incision can be made at the junction of the cystic duct and the CBD with an extension of only 3 mm at the lateral margin of the CBD to ensure that the wire basket can be inserted into the CBD (Fig. 4).20,21 During stone removal, the CBD and cystic duct should be kept as parallel as possible.
Attention to the application of LUS in CBD exploration
LUS can effectively avoid interference from abdominal wall fat and organs. 14 In our experience, when performing ultrasound exploration under laparoscopic guidance, the ultrasound probe should be bent downward from the back to hook the CBD and close to the wall of the CBD for exploration from top to bottom. After reaching the lower end, the probe was rotated to scan the ampullary and inner segments of the duodenal wall. If the probe does not closely fit the CBD, the scanning effect can be improved by injecting sterile saline. Examination of the duodenal segment of the CBD may be disturbed by intestinal gas; therefore, the intestinal gas can be removed to improve accuracy. Transverse scanning was performed at the operative hole below the xiphoid, whereas longitudinal scanning was performed at the right abdominal operative hole. For small sediments or stones at the end of the CBD, false-negative results may occur due to the difficulty in ultrasound imaging; therefore, the surgeon needs to have relevant professional knowledge of ultrasound or receive assistance from an ultrasound specialist.
How to deal with a large-diameter stone
For large stones that are challenging to extract, a microincision (Fig. 4) can be performed. In cases where successful stone removal is not achieved, it is advisable to avoid forceful pulling and instead opt for postoperative ERCP for stone extraction. Therefore, a comprehensive evaluation of the diameters of the bile duct stone and cystic duct is essential before surgery.
The management of the stump of cystic duct
In order to avoid bile leakage, the cystic duct stump should be treated more carefully. For patients without microincision of the cystic duct–CBD junction, the cystic duct stump can be treated with absorbable clipping. For patients with a microincision of the cystic duct at the confluence with the CBD, an absorbable clip can be used after the incision is interrupted and sutured with absorbable thread (Fig. 2i, j),22–24 and attention should be paid to avoid excessive suturing causing biliary stricture. The clipping position should be as far away from the CBD as possible to prevent iatrogenic injury. In this study, no postoperative bile leakage occurred.
The method of removing common bile duct stones through the cystic duct avoids incision of the common bile duct, so there was no need to worry about postoperative biliary stricture. For several difficult cases, we used a microincision technique (Fig. 4) to avoid direct longitudinal incision of the anterior wall of the common bile duct. We also changed the incision from the traditional straight line to a similar arc, thus reducing the damage to the wall of the common bile duct and reducing the risk of biliary stricture caused by postoperative scar tension and scar contracture.
Can biliary stent be performed?
Theoretically, ultrasonography can detect the stent and determine whether it passes through the duodenal papilla. Using the microincision technique, we can place a biliary stent in the CBD through an opening at the junction. We did not attempt it because there was no apparent suppurative cholangitis in the above cases. This application can be further pursued once the technology reaches maturity.
Based on our experience in surgery, we summarized the indications and contraindications of the LUS-guided transcystic surgical method. This method is ideal for cases with thin CBDs and where small gallbladder stones have migrated into the CBD, resulting in secondary CBD stones. 25 Among these cases, 10 patients who underwent successful stone removal had cholesterol stones that were firm in texture and not easily fragmented; these stones were visible on ultrasound imaging, leading to a higher success rate of stone removal. However, 2 cases with residual biliary pigment stones may have fragmented during the stone-removal process, resulting in some small fragments remaining. The number of common bile duct stones is <3; cholesterol stones are an indication for surgery. And the diameter of a CBD stone should be less than or equal to that of the cystic duct.26,27 The diameter of the cystic duct should be >0.4 cm.
In addition, patients without serious inflammatory adhesions in Calot’s triangle or an obtuse angle between the cystic duct and the distal CBD are more suitable candidates for stone removal procedures.
Preoperative imaging (such as abdominal ultrasonography, computed tomography, and magnetic resonance cholangiopancreatography) can accurately evaluate the diameters and directions of the CBD and cystic duct, as well as the size, quantity, and nature of the stones, to judge the indications and improve the success rate of surgery.
LUS observation is less accurate than choledochoscopic observation in assessing Oddi’s sphincter contraction function. Because this procedure does not require indwelling T-tubes, cases of calculi incarceration, large or multiple stones, and suppurative cholangitis should be considered as contraindications. 28 When stones are taken through the cystic duct, the small fragile cystic ducts, as well as anatomic variations, distortion, and obstruction of the cystic duct, are contraindications. And bile duct stones located in the hilar region is also a contraindication for surgery.
This technique can be performed concurrently with LC without the need for CBD opening or T-tube retention, avoids potential damage to the Oddi’s sphincter that may occur with ERCP, and requires a short hospitalization time and quick recovery after surgery. Overall, the intraoperative and postoperative results were satisfactory for the patients who underwent this novel surgical method for CBD stones. This method offers a cost-effective solution for patients with choledocholithiasis, especially those without a dilated CBD. Even negative exploration results or incomplete stone removal can be acceptable because this approach does not cause additional trauma to the patients. In cases where complete stone removal was difficult, postoperative ERCP may be necessary. High-level surgical centers can consider implementing this technique.
There are some limitations to this study, including a small number of cases and lack of a control group. Our center has conducted preliminary trials using this approach. We hope that more centers will try this method and further summarize the standardized process.
Conclusions
For patients with choledocholithiasis, especially those with a nondilated CBD and small-diameter stones, CBD exploration and transcystic stone extraction under LUS guidance are safe and cost-effective methods; however, strict control over surgical indications is necessary. This study could help develop approaches for improving choledocholithiasis treatment.
Footnotes
Acknowledgments
The authors thank the operating room nurses and anesthesiologists who participated in the operation.
Authors’ Contributions
F.W.: Writing—original draft, Data curation, Investigation, Conceptualization, and Formal analysis; R.Z.: Writing—review & editing, Investigation, Conceptualization, and Formal analysis; X.W.: Investigation, Conceptualization, Data curation, and Visualization; L.Z.: Writing—review & editing, Project administration, Conceptualization, and Supervision.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.