
Abstract
Backgrounds:
In the renal intrarenal stone surgery (RIRS) procedure, ureteral access sheath (UAS) is still used in the majority of surgeries to both protect the flexible ureteroscope (FURS) and reduce intrarenal pressure. ClearPETRA is a new UAS that has an integrated aspiration port. We aimed to evaluate the clinical outcomes and effectiveness of Aspiration-Assisted UAS (ClearPETRA) in the RIRS procedure.
Methods:
One thousand six hundred twenty patients who underwent RIRS between January 2021 and January 2024 were evaluated retrospectively and 512 patients were included in the study. According to stone size, patients with stones less than 2 cm and those with stones between 2 and 3 cm were analyzed separately. Patient's demographic data, stone size, body mass index, Extracoporeal Shockwave Lithotripsy (ESWL) history, stone side, stone density (Hounsfield Unit), operation time, stone-free rate (SFR), and the number of patients with sepsis were recorded. SFR was evaluated with kidney urinary bladder 3 months after surgery for opaque calculi. Nonopaque calculi patients were evaluated with noncontrast computed tomography 3 months after surgery. In the postoperative evaluation, patients with stones less than 4 mm were evaluated as SFR. P value of <0.01 was considered statistically significant.
Results:
Patient's demographic data, stone characteristics, and history of ESWL were similar in the ClearPETRA and UAS groups (P > .05). A total of 328 patients who underwent RIRS for stones less than 2 cm were included (80 ClearPETRA, 248 UAS). Length of hospital stay, operation time, SFR, secondary intervention, or postoperative sepsis (P ≥ .01) were similar in both groups. The incidence of postoperative fever was statistically significantly lower in the ClearPETRA group (P = .006). A total of 184 patients who underwent RIRS for stones between 2 and 3 cm were included (42 ClearPETRA, 142 UAS). In the ClearPETRA group, operation time was statistically significantly shorter (P = .002), SFR was statistically significantly higher (P = .003), and the number of fever and sepsis were statistically significantly less (P = .003 and 0.002, respectively).
Conclusion:
We found that ClearPETRA reduces the likelihood of postoperative fever after RIRS surgeries. Moreover, we can say that the use of ClearPETRA in RIRS, especially for stones larger than 2 cm, reduces the operation time, increases the SFR, and also reduces sepsis rates.
Introduction
Kidney stones are a common health problem that occurs worldwide. According to the World Health Organization, ∼10–15% of the world's population will experience kidney stone formation at least once in their lifetime. 1
The incidence of kidney stone formation can vary depending on geographic region, climate, dietary habits, and genetic factors. In general, people who live in hot climates and consume low amounts of fluids are at an increased risk of kidney stone formation. 2
Renal intrarenal stone surgery (RIRS) is a minimally invasive procedure that is increasingly used to treat renal calculi. The procedure involves the insertion of an ureteral access sheath (UAS) into the ureter to create a working channel for the endoscope and other instruments. Although RIRS can be performed without UAS in recent years, it is still used in a large portion of surgeries for both the protection of flexible ureteroscope (FURS) and the reduction of intrarenal pressure. We also use it in almost all of our RIRS surgeries. 3
Traditional UASs are made of silicone or latex and are not designed to remove blood and debris from the ureter. This can lead to ureteral edema, inflammation, and stricture formation. 4
ClearPETRA is a new UAS that has an integrated aspiration port. The aspiration port allows for the removal of blood and debris from the ureter, which can help to reduce the risk of ureteral complications. 5
The purpose of this study was to evaluate the efficacy of ClearPETRA in RIRS.
Materials and Methods
This study was carried out with the Prof. Dr. Cemil Tascioglu City Hospital Ethics Committee's approval dated 05.02.2024 and numbered 08.
A total 512 of 1620 patients who underwent RIRS between January 2021 and January 2024 were included in the study. The patients were retrospectively evaluated. For standardization, patients with kidney or proximal ureter stone of 3 cm or less were included in the study. ClearPETRA 11/13F was used in 122 of the patients in RIRS surgery, while 10/12 UAS (Plastimed 10/12) was used in 390. The patients were given complete blood count, routine biochemistry tests, electrocardiogram, chest X-ray, and urine culture tests before surgery. Patients with positive urine culture were treated with antibiotics and operated on after the urine culture became negative. Patient's demographic data, stone size, Body Mass Index, Extracorporeal Shockwave Lithotripsy (ESWL) history, stone side, Stone density (Hounsfield Unit [HU]), operation time, stone-free rate (SFR), and the number of patients with sepsis were recorded. Patients with stones less than 2 cm and between 2 and 3 cm were evaluated separately. Patients who had previous surgery for kidney and ureter stones, patients with multiple calyceal stones, patients who did not use UAS during surgery, patients with renal anomalies, and patients who had pyelonephritis due to stone and had nephrostomy were not included in the study. The study flow diagram is shown in Figure 1.
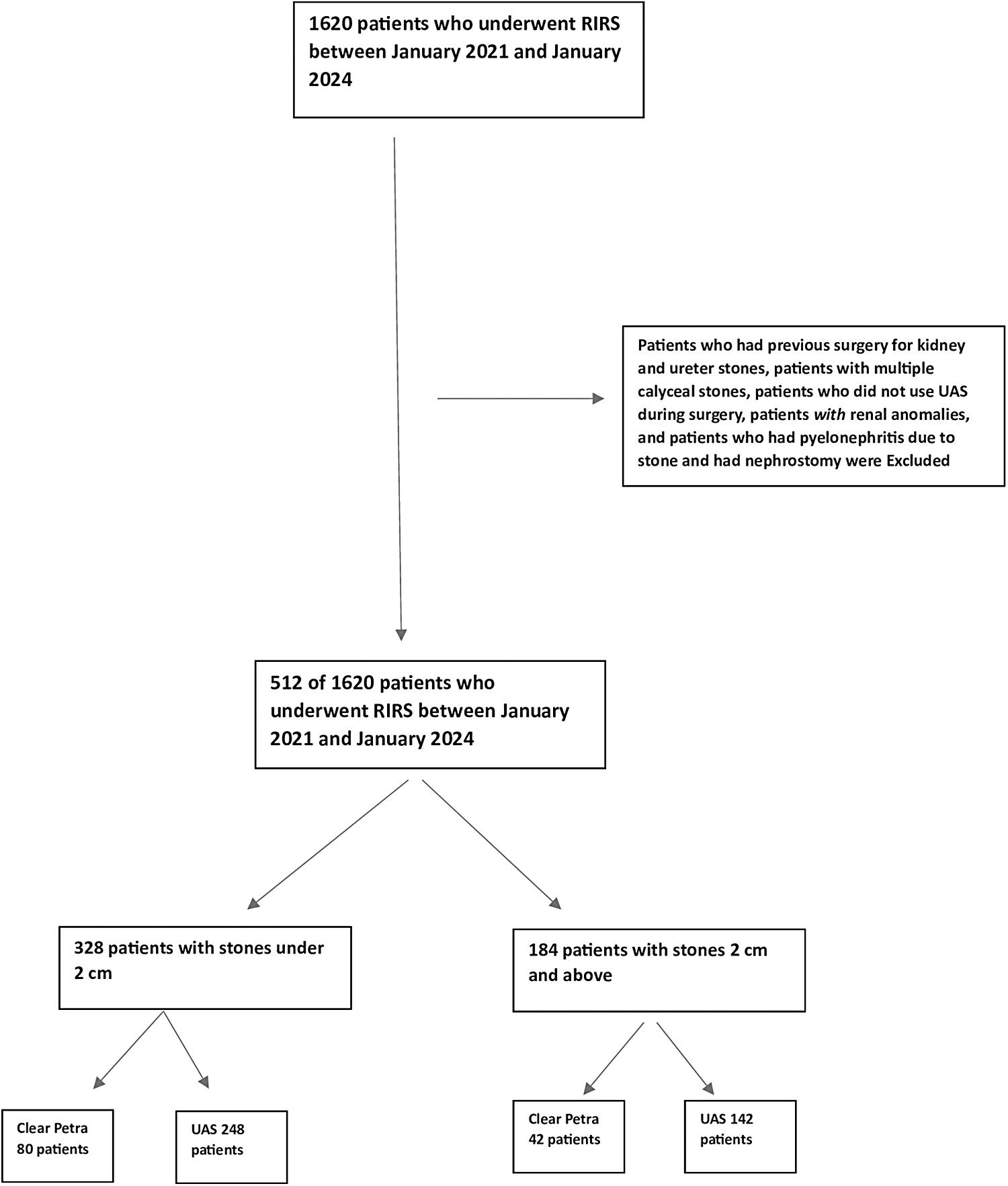
Study flowchart.
Patients who underwent RIRS with Double-J stent insertion due to inability to place UAS through ureter and patients who underwent second surgery 3 weeks later were included in the study. All patients underwent noncontrast computed tomography (CT) before surgery. SFR was evaluated with kidney urinary bladder 3 months after surgery for opaque calculi. Nonopaque calculi patients were evaluated with noncontrast CT 3 months after surgery. In the postoperative evaluation, patients with stones less than 4 mm were evaluated as SFR. All patients underwent Double-J stent placement during surgery, and Double-J stent was removed 14–21 days later.
Retrograde intrarenal surgery
First, a Comeg 8/9.8F semirigid ureteroscope was inserted into the side of the operation and a guidewire was placed. UAS or ClearPETRA was placed over the guidewire. Afterward, Hugemed (HU30S 7.5F) FURS was inserted. Stones were fragmented using a Ho-YAG (Quanta 30 W) device and a 273-lm laser fiber. The laser parameters were adjusted according to the stone hardness, with energy ranging from 1 to 2 joules, frequency from 5 to 10, and power from 5 to 20 W.
Statistical analysis
A chi-square test was used for the comparison of the two study groups. The Student's t-test was used for testing continuous variables conforming to a normal distribution. The Wilcoxon test was used to test continuous variables that did not conform to a normal distribution. A P value of <0.01 was considered statistically significant. The SPSS 20.0 software was used for statistical analyses.
Results
Patient's demographic data, stone characteristics, and history of ESWL are summarized in Table 1. No statistically significant difference was found in the demographic data, stone characteristic of the patients, and history of ESWL (P ≥ .01).
Demographic Data and Stone Characteristics
Patients who underwent RIRS were categorized by stone size: under 2 cm and 2 cm≤ both groups were then classified into two groups ClearPETRA and UAS. The ClearPETRA and UAS groups were compared with each other.
There were 328 patients with stones under 2 cm. ClearPETRA was used in 80 of the patients, and UAS was used in 248 of the patients. When the ClearPETRA and UAS groups were compared, there was no statistically significant difference in terms of hospital stay, operation time, SFR, secondary intervention, or postoperative sepsis (P ≥ .01). Only the ClearPETRA group had a significantly lower incidence of postoperative fever (P ≤ .01). The detailed table of patients with under 2 cm parameters is presented in Table 2. Patients who underwent RIRS after Double-J were statistically significantly higher in the ClearPETRA group.
Operative Data for Patients with Stones Under 2 cm
RIRS, renal intrarenal stone surgery.
There were 184 patients with stones 2 cm≤. ClearPETRA was used in 42 of the patients, and UAS was used in 142 of the patients. When the ClearPETRA and UAS groups were compared, there had statistically significant difference in terms of operation time, SFR, secondary intervention, postoperative fever, and postoperative sepsis (P ≤ .01). The ClearPETRA group had significantly better outcomes than the UAS group for all of these parameters. The only no statistically significant difference between the ClearPETRA and UAS groups was in the length of hospital stay. Patients who underwent RIRS after Double-J were statistically significantly higher in the ClearPETRA group. The detailed table of patients with stones 2 cm≤ parameters is presented in Table 3.
Operative Data for Patients with Stones 2 cm and Above 2 cm
RIRS, renal intrarenal stone surgery.
Discussions
The development of flexible ureteroscopy (URS) and laser technologies has led to a shift in the paradigm of renal stone management. Retrograde intrarenal surgery (RIRS) has become the preferred approach for the management of kidney and proximal ureteral stones in most cases. RIRS is a safe and effective procedure that can be used to treat a wide range of kidney and ureteral stones in all age groups, with a variety of stone sizes, and in almost all kidney locations. It is also well suited for patients with bleeding and coagulation disorders and for patients with kidney anomalies.6–8
Although there have been recent Ex Vivo publications on the use of UAS-free RIRS with low irrigation rates for small stones with thin flexible URS, UAS is still used in many patients undergoing RIRS. 9 The UAS provides a stable platform for the flexible URS device and helps to protect the device from damage. The UAS also helps to reduce intrarenal pressure, which can help to prevent complications such as bleeding and infection. 10
The most important goal of RIRS is to achieve maximum SFR with minimal complications. The SFR and complications of patients vary depending on the stone size, location, and duration of the procedure. The most feared complication of RIRS surgery is sepsis.10,11 V-UAS (Vacuum-assisted UAS-ClearPETRA) is used to reduce intrarenal pressure and improve image quality during the operation due to its aspiration feature.11,12
In a systematic review by Giulioni et al., aspiration methods were evaluated in the retrograde intrarenal surgery (RIRS) procedure. The authors reported that aspiration devices in RIRS surgery increased SFR, reduced postoperative infectious complications, and decreased intrarenal pressure, resulting in improved image quality by reducing dusts. 12 In another study by Gauhar et al., a high SFR was observed with the use of aspiration—Flexible and Navigable Suction UASs. No infectious complications were observed. 13 In an ex-vivo porcine study by Wang et al., Vacuum-Assisted Ureteral Access Sheath (VUAS) was found to significantly reduce intrarenal pressure. This suggests that VUAS could be effective in reducing infectious complications, particularly. 14
There are also studies showing that ClearPETRA is effective in mini-percutaneus nephrolithotomy (PNL) surgery, especially in children. In the studies conducted by Quiroz et al. and Collura et al., it was revealed that the use of ClearPETRA in mini-PNL surgery is advantageous in terms of both SFR and sepsis.15,16
Our study is valuable in that it has a larger number of patients than other studies, and it is one of the few studies that evaluate stones less than 2 cm and stones greater than 2 cm separately in patients who received ClearPETRA.
Our study has several limitations. First, it is possible to consider which patients were treated with ClearPETRA and which patients were treated with UAS. ClearPETRA was started to be used in our clinic after January 2023. ClearPETRA was used in patients after this date, and only 3 patients without ClearPETRA were treated with 10–12F UAS. The inability to include the fluoroscopy time in the study due to the fact that it was not recorded in all patients, and the fact that the study was not prospective are the other limitations of the study. The statistically significant higher proportion of patients who underwent RIRS after Double-J in the ClearPETRA group may be attributed to the thickness of ClearPETRA compared to the UAS group.
Conclusion
We found that ClearPETRA reduces the likelihood of postoperative fever after RIRS surgeries. Moreover, we can say that the use of ClearPETRA in RIRS, especially for stones larger than 2 cm, reduces the operation time, increases the SFR and also reduces sepsis rates. We think that these data should be supported by prospective studies.
Footnotes
Authors' Contributions
M.E.: Conceptualization (lead); writing—original draft (lead); formal analysis (lead); writing—review and editing (equal). M.B.: Methodology (lead); writing—review and editing (equal). M.A.S.: Methodology (lead); writing—review and editing (equal); L.O.: Conceptualization (supporting); writing—original draft (supporting); writing—review and editing (equal); O.C.: Conceptualization (supporting); writing—original draft (supporting); E.D.: Methodology (lead); writing—review and editing (equal). E.C.P.: Supervision; validation; visualization. A.O.: Supervision; validation; visualization.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.