
Abstract
Introduction:
Urologic complications are thought to be the most common surgical complication of renal transplantation. Ureteral pathology, including stenosis, urine leak, and vesicoureteral reflux, predominates. Although endourologic and interventional radiological management may be utilized, failure rates remain relatively high and surgical reconstruction remains the definitive management. Robotic ureteral reconstruction has been demonstrated to provide patient benefit in nontransplant populations, but the literature on transplant reconstruction is very limited. This study reports an additional series of patients with a focus on surgical technique, as well as reviews the available evidence for robotic reconstruction for post-transplant ureteral complications.
Methods:
All institutional patients undergoing robotic-assisted reconstruction for post-transplant ureteral complications for the years 2019–2022 were included. Intra- and postoperative variables, patient demographics, and follow-up data were obtained retrospectively from parsing of patient records. Statistics were tabulated descriptively.
Results:
Eleven patients underwent ureteral reconstruction. Of the 11, 9 (81%) were male with a mean age of 51.9 years (16–70) and BMI of 33.8 (24.3–49.1). The most common (10/11) indication for reconstruction was stricture; the most common (10/11) technique used was Lich-Gregoir reimplantation. Mean operative time was 288 minutes (143–500). There were no intra- or immediate postoperative complications. Median length of stay was 2 days (1–22). There were two incidences of mortality at 2 and 5 months postoperatively unrelated to surgery. There were four readmissions within 30 days, three for urinary tract infection (UTI) and one for a pelvic abscess which required washout. The remainder of the cohort has been followed for a mean of 14.6 months (6–41) without any incidences of graft loss or recurrence of ureteral pathology.
Conclusions:
Robotic-assisted ureteral reconstruction is a technically challenging but highly feasible technique that may provide the benefits of minimally invasive surgery while still allowing definitive reconstruction. Centers with extensive robotic capabilities should consider the technique.
Introduction
Background
Urologic complications following kidney transplantation are a challenging clinical scenario with overall estimates of incidence ranging from 2.5% to 14%.1,2 Urologic complications are thought to be the most common surgical complication of renal transplantation, of which ureteral stenosis, urine leak, and vesicoureteral reflux (VUR) predominate. 3 Of these, ureteral stricture is the most common; estimates of stricture incidence vary, with the largest systematic review suggesting a rate between 1.9% and 3.7%, dependent on technique. 4 Furthermore, renal transplantation is estimated to be responsible for between 3% and 8% of all ureteral strictures. 5 Risk factors for post-transplant ureteral stenosis are believed to act through ischemia and inflammation of the graft tissue. Surgical errors (i.e., stripping the ureter), as well as extended cold ischemia, acute rejection, and general postoperative complications are all known to increase the risk of stenosis. 6 Urine leak, which is most often an early complication, has an estimated incidence of 1.5% to 6.0% in later series which has been noted to decrease over time and with increasing experience. 3 Transplant VUR is in the majority of cases asymptomatic, and if necessitating repair occurs as a late complication. The reported incidence of VUR varies widely (0.5% to 86%), largely owing to inconsistent reporting criteria; treatment is largely indicated by reflux nephropathy and recurrent UTI in the setting of demonstrated high-grade VUR. 7
Optimal management of post-transplant urologic complications is not currently defined. 8 Before the advent of advanced endourologic and interventional radiological techniques, treatment for ureteral stricture was limited to open surgery, including reimplantation, diversion, and interposition. 9 Technological advances in subsequent decades have enabled a variety of minimally invasive management approaches. Currently, endourological management is considered a reasonable first step for the majority of patients with both ureteral stenosis and urine leak, as well as patients with clinically significant VUR. 10 However, despite the availability of endourological and interventional radiological management, these strategies have success rates that lag significantly behind definitive surgical repair: specifically, 64.3% versus 85.4% for stricture when compared as a primary treatment. 8 Given that robotic ureteral reconstruction is a well-established technique in the nontransplant literature with demonstrated benefits over open surgery, there is strong impetus for extending the technique to the management of renal transplant complications.11–13
Literature review
There are limited clinical data available on robotic ureteral reconstruction in the transplant population, currently with <30 cases available for review in the literature.
The first report of robotic-assisted management of transplant ureteral pathology was published by Abdul-Muhsin et al. in 2017. 14 This series of five patients described the management of transplant ureteral stricture which had previously failed other minimally invasive management. Three patients underwent distal ureterectomy with Lich-Gregoir reimplantation; two patients underwent pyelovesicostomy. There were no conversions to open or intraoperative complications; one patient required ICU admission for postoperative sepsis but recovered with supportive care.
In addition, in 2017, Benamran et al. published a series and comparative study of 10 patients undergoing robotic-assisted ureteral reconstruction and 7 undergoing open repair. 15 Four patients in the robotic group required conversion to open leaving a final cohort of 6 patients managed with robotic repair. Four patients underwent ureteroureterostomy, and two underwent ureteropyelic anastomosis. One patient in the robotic group had a complication of an anastomotic stricture which was managed endoscopically. Comparison with the open group demonstrated shorter length of stay (LOS) (5 versus 9 days; p = 0.003), faster return to normal PO intake (1 versus 3 days; p = 0.012), and less utilization of opiate analgesia (1 day versus 5 days; p = 0.0035). At follow-up no patients in the robotic group had recurrence of VUR-causing pyelonephritis or recurrent stricture.
The next series was published by Yang et al. in 2019 and described robotic reconstruction in a series of patients with both post-transplant stricture and VUR. 16 Two patients underwent repair for VUR causing graft pyelonephritis; four underwent repair for ureteral stricture resulting in deterioration of renal function. One patient underwent robotic transplant to native ureteroureterostomy; the remaining five underwent robotic transplant to native pyeloureterostomy with one case requiring conversion to open. The series also included a single traditional laparoscopic transplant to native ureteroureterostomy. At extended follow-up no patient had either recurrent pyelonephritis or recurrence of stricture.
Subsequently, Kim et al. in 2020 reported a series of five patients who also underwent robotic repair for post-transplant stricture. 17 All patients had confirmed stricture after presenting with renal deterioration and were previously treated with nephrostomy tubes. Three patients underwent pyelovesicostomy, two with Boari flap, one without; two underwent neoureterocystostomy. All repairs were reported as successful with intra- or postoperative complications nor readmissions; all grafts were preserved.
Finally, Malinzak et al. in 2021 reported a series of three patients undergoing robotic repair for ureteral stricture after robotic-assisted kidney transplant. 18 All patients presented with renal deterioration and were managed with nephrostomy tube placement in addition to ureteral stent placement, the failure of which prompted surgical management. Two patients underwent Lich-Gregoir reimplantation; one underwent transplant to native pyeloureterostomy. There were two Clavien–Dindo grade II complications of a port-site hematoma and a UTI. There were no intraoperative complications nor conversions to open; all patients retained good graft function at follow-up. A summary of prior studies is presented in Table 1.
Summary of Prior Studies
Methods
Patient selection and data collection
All patients undergoing robotic-assisted transplant ureteral reimplantation (RATUR) at the author’s institution in the years 2019 and 2022 were included; no exclusion criteria were applied. The data collection method was retrospective through parsing of patient charts/records. Complications were graded using the Clavien–Dindo classification. Institutional IRB study approval was sought, and it was determined that this research was exempt. Informed consent was obtained from all participants.
Operative technique
All operations were performed by a urologist with extensive (>20 years) experience in advanced robotic urological procedures. All operations were performed using the da Vinci Xi Surgical System (Intuitive Surgical, Sunnydale, CA, USA). In all cases, Foley catheters were placed and patients were secured to the operating table with beanbags and tape before prepping and draping in the usual sterile manner. A 12 mm laparoscopic port was placed in the left upper quadrant (LUQ) through the rectus muscle utilizing direct visualization. A measure of 15 mmHg of pneumoperitoneum was applied. The abdomen was inspected for adhesions; any encountered were taken down with laparoscopic scissors. Four additional 8 mm robotic ports were then placed under direct visualization, symmetrically spaced approximately 10 cm apart across the right upper quadrant (RUQ) and LUQ completing a “fan” distribution. The graft was identified, and any adherent bowel carefully taken down. In all cases, dissection was complicated by dense fibrosis encountered around the transplant fossae and ureteral anastomoses. Dissections began along the anterior abdominal wall into the preperitoneal space to expose the graft and dome of the bladder. In all cases, the suspected location of the ureteral anastomosis was surrounded by an area of dense fibrosis. Meticulous dissection commenced primarily utilizing fenestrated bipolar forceps and monopolar curved scissors. Fibrous tissue was dissected until the graft ureter could be identified and inspected for the area of calcification/stricture. The graft ureter and surrounding fibrous tissue were then divided sharply and the pathological section excised from the bladder. One patient was found to have the graft ureter obliterated along its entire length by fibrous tissue. In this case, the obliterated ureter and surrounding fibrous tissue were excised en bloc. The bladder was then mobilized on the ipsilateral side until it could reach the transplant pelvis without tension. Matching incisions in the renal pelvis and bladder dome were made; anastomosis was accomplished in two layers using a 4-0 knotless barbed suture system in a running manner. The anastomosis was made over a 6 Fr Double J ureteral stent.
For the remainder of the cases, the bladder lumen was identified and inspected through the cystostomy after the distal ureterectomy. The proximal ureter was dissected free of surrounding tissue and spatulated to a length of approximately 1 cm. A 6 Fr Double J stent was placed between the bladder lumen and proximal ureter. Reimplantation using a modified Lich-Gregoir technique commenced. Mucosal anastomosis was completed in two segments utilizing running 4-0 Monocryl suture. The adventitial layer was oversewn utilizing a 4-0 knotless barbed suture system in a running manner. In all cases a 19 Fr pelvic drain was left in place. The robot was undocked, and all port sites were closed in the standard manner. Key operative steps are illustrated in Figure 2.

Intraoperative images from robotic laparoscope.
Results
Patient demographics and preoperative variables
Eleven patients underwent RATUR. There were nine male and two female patients. Mean age was 52.0 years (16–70); mean BMI was 33.8 (24.3–49.1) (Table 2). Stricture was the indication for reimplantation in 10/11 (90.9%) patients (Figure 1). One patient (#6) required reimplantation for a urinary leak after undergoing washout for an infected perinephric collection. All patients had preoperative management with nephrostomy tube placement and subsequently failed capping.
Patient Demographics and Preoperative Variables
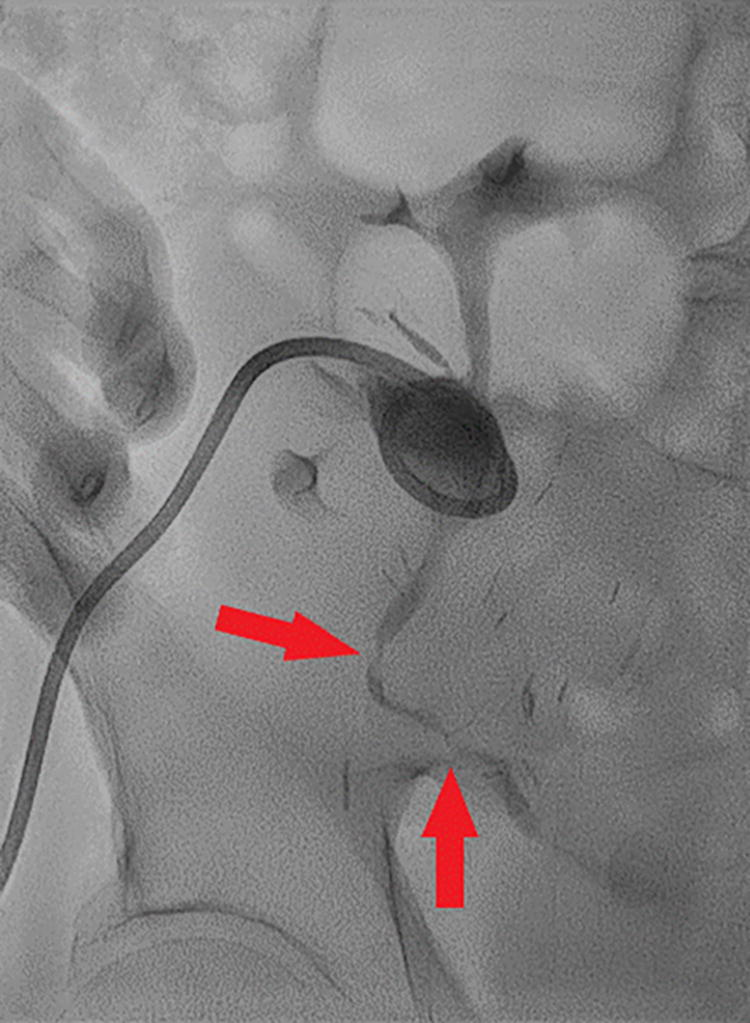
Nephrostogram obtained during interventional radiology (IR) nephrostomy tube exchange of patient #4 demonstrating stenosis and luminal irregularity of the distal graft ureter, indicated by arrows.
Intra- and postoperative results
Mean operative time was 288.6 minutes (143–500). Mean estimated blood loss (EBL) was 45 mL (5–200) with no patients requiring transfusion. There were no intraoperative or immediate postoperative complications. Median length of stay was 2 days (1–22) (Table 3). All patients were discharged home with a Foley catheter, which was maintained for 2 weeks; all ureteral stents were maintained for 6 weeks and were removed with outpatient cystoscopy.
Intra- and Postoperative Variables
Follow-up results
There were two incidences of mortality in the cohort. The first (patient #3) re-presented 2 months postoperative with worsening shortness of breath and lethargy in the setting of COVID-19 infection. His respiratory status worsened, requiring intubation and paralysis. He remained intubated/paralyzed for 10 days with some transient episodes of hemodynamic stability. However, after 10 days he developed acute septic shock with progressively worsening hemodynamic status despite maximal vasopressor support. Unfortunately, after 3 days of maximal medical therapy, the patient suffered cardiac arrest and could not be revived. The second (patient #7) was found deceased at home 5 months postoperatively. Postmortem examination was consistent with myocardial infarction (MI) in the setting of long-standing hypertension. Both patient #3 and patient #7 had urologic and nephrology follow-up at 1 and 4 months postoperatively, respectively, before their passing. Both had stable graft function and were voiding well; neither had urologic concerns or extended complications from reimplantation.
One patient (#10) had an extended LOS at 22 days, as well as a readmission within 30 days, for a Clavien–Dindo Grade IIIb complication of a pelvic abscess requiring washout and stent placement. The patient had had a previously complicated course, including a pelvic abscess before referral for ureteral reconstruction; the patient in addition suffered from neutropenia secondary to difficult titration of immunosuppression. The patient underwent washout 2 months after reconstruction and was hospitalized for an additional 10 days for antibiosis and rehabilitation. She was discharged to home and subsequently has not suffered any urologic disease and has had stable graft function.
Two patients (#6, 11) developed grade II complications of UTI which required readmission for intravenous (IV) antibiotics. One patient (#8) similarly developed a grade II complication of orchitis requiring admission for IV antibiotics.
The remainder of the cohort has been followed up for an average duration of 14.6 months; all have had stable graft function, and none has had extended complications from reimplantation (Figure 3).

Serum creatinine versus timepoint for each included patient.
Discussion
To our knowledge, this is the largest series to date reporting the use of robotic surgery for the management of post-transplant ureteral complications.
Several factors complicate the interpretation of the limited literature surrounding the robotic repair of post-transplant ureteral complications. The heterogeneity in indications (e.g., stenosis versus leak), severity (e.g., extent of stenosis), and the technique of repair reduce the validity of cross-case comparison. However, it should be noted that in 100% of the cases reported thus far graft function was preserved and the reconstruction definitively resolved the ureteral pathology. Although study heterogeneity thus far precludes statistical comparison, qualitatively the complication rate is within an acceptable range.
This small series adds to the limited clinical literature on robotic-assisted ureteral reimplantation for post-transplant ureteral complications. All of the reported cases were technically challenging, owing primarily to dense fibrosis in the transplant fossae, necessitating extensive and meticulous dissection. Despite these difficulties, no cases required conversion to open, and there were no intraoperative or immediate-postoperative complications, nor hemorrhage requiring transfusion. The successes along these lines provide evidence that the robotic approach enables definitive reconstruction despite hostile operative fields. Two patients did require readmission within 30 days for infectious complications; however, it should be noted that both of these patients had already developed infected perinephric collection/pelvic abscess before requiring reimplantation. The other two readmissions, both for urologic infections (UTI/orchitis), serve to highlight the ever-present risks of extensive instrumentation/surgical manipulation of the urinary tract.
There were two incidences of mortality in the cohort; however, neither was likely related to surgery. The first, occurring 1 month postoperatively, was from COVID ARDS. Given the timing (several weeks removed from surgery) it is unlikely that undergoing RATUR was a causal factor in the contraction of COVID-19 nor the subsequent deterioration. The second, 5 months remote from surgery was confirmed postmortem to be from MI in the setting of long-standing hypertension. Given this, the reimplantation was unlikely to be a causal factor.
Of the remaining cohort, all had complete symptom resolution and preserved graft function without further need for surgical intervention. Given the low complication rate and short average length of stay, this cohort further argues for RATUR as an excellent minimally invasive management option for definitive repair of post-transplant ureteral complications.
Limitations and future directions
Limitations of this study include its small size, retrospective nature, and lack of comparison or control group. Future studies should use larger cohorts and compare robotic reimplantation with other minimally invasive management methods. Future studies should also consider developing standardized treatment protocols for post-transplant ureteral complications based on the type, location, and extent of ureteral pathology.
Conclusion
Robotic-assisted transplant ureteral reconstruction is a technically challenging but highly feasible technique that may provide the benefits of a definitive open surgical approach, however in the most minimally invasive manner. More centers with high robotic capabilities should consider the technique for the management of post-transplant ureteral complications and consider the development of standardized protocols incorporating for reconstruction after the failure of interventional management. Larger series should be undertaken to allow formal comparison with both open and endourological management.
Footnotes
Authors’ Contributions
M.M.: Data curation, investigation (lead), writing—original draft (lead), and writing—review & editing. A.S.: Resources, conceptualization, writing—review & editing, validation, and visualization. R.K.: Resources (lead), writing—review & editing (lead), visualization (lead), and conceptualization. K.P.S.: Conceptualization, writing—review & editing, and validation. A.N.: Project administration, conceptualization, and writing—review & editing. J.J.: Resources, writing—review & editing, conceptualization, and validation. G.W.: Resources, supervision (lead), conceptualization, writing—review & editing, methodology, and validation. The authors declare that all listed individuals contributed substantively to the work and take public responsibility for its content.
Disclosure Statement
The authors declare they have no financial interests related to this work.
Funding Information
The authors declare that no funding or other material or financial support, internal or external, was received in the preparation and completion of this work.