
Abstract
Background and Objectives:
Endoscopic resection of gastrointestinal (GI) tract lesions, originating from Japan, is becoming more frequently used in European countries. Endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) ensure minimally invasive removal of benign, premalignant, and early neoplastic tumors of esophagus, stomach, and intestine in selected group of patients. Aim of this study was to determine the outcomes, radical resection rate (R0), and complication rate of ESD procedures performed in our department.
Methods:
The data from 100 ESD procedures of esophageal, gastric, duodenal, and colorectal lesions performed in out unit between 02.01.2020 and 30.06.2023 were collected and analyzed retrospectively.
Results:
A total of 42 male and 58 female patients in the median age of 64 years (range, 31–89 years) underwent ESD. Mean duration of the procedure was 66 minutes (ranging 25–185 minutes). Tumors were located in the esophagus in 8 cases (8%), stomach in 25 cases (25%), duodenum in 1 case (1%), and colon in 66 cases (66%). Radical resection was achieved in 98 cases (98%); 2 patients were qualified for surgical treatment. Average size of dissection lesions was 26 × 19 mm. The biggest one was 60 × 60 mm (sigmoid adenoma), and the smallest one was 5 × 5 mm (gastrointestinal neuroectodermal tumors). Complication occurred in 10 patients (10%)—9 perforations of the wall of intestine (9%) and 1 hemorrhage, which required endoscopic intervention (1%).
Conclusions:
Implementation of ESD to clinical practice gives the opportunity for minimally invasive, radical treatment of benign, premalignant, and early neoplastic lesions of gastrointestinal tract in selected group of patients. Experienced endoscopists, following current guidelines and standardized process of qualification, are crucial to minimize the risk of severe complications.
Introduction
Endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) are being widely used for minimally invasive removal of benign, premalignant, and early neoplastic lesions of gastrointestinal (GI) tract 1 (Fig. 1). Elevation of the lesion is achieved with submucosal injection (in EMR most commonly with normal saline, in ESD with mannitol, dextran, hyaluronic acid, and other thick fluids) in static or dynamic technique. EMR is a well-known technique developed almost 30 years ago. It is performed by capturing the lesion with snare device and removing it using electrocautery. 2 This method is limited to lesions smaller than 20 mm, has no use in nonlifting tumors, and do not ensure proper histological findings in malignant tumors. ESD was developed around 10 years later to face these limitations but it is also technically more difficult and associated with higher rate of complications. This technique is based on a gradual methodical cutting of the lesion with an electrosurgical knife in the submucosa just above the muscular layer after cutting surrounding mucosa.3,4 ESD was introduced in 1995 in Japan in face of high prevalence of gastric cancer. There was a need for minimally invasive tool allowing radical resection of early neoplastic lesions larger than 20 mm and allowing proper histopathological examination. Due to satisfying outcomes in upper GI tract, it quickly found its place in colorectal lesions reaching gaining popularity among endoscopists. At the beginning ESD was associated with a high risk of complications (perforation in around 10% of cases), but these numbers decreased in time with rising experience of the operators. Currently, perforation rate and hemorrhage rate are being estimated for 1.5%–5.2% and 1.1%, respectively. 5 In comparison to EMR, ESD gives an opportunity to increase the rate of en bloc resections of flat lesions larger than 20 mm with R0 resection rate accounting for 84.5% for esophageal, 82%–92% for gastric, and 53%–91% for colorectal lesions.4,6 Both techniques are being widely used and continuously developed in esophageal,7–12 gastric,13–16 duodenal,17–20 and colorectal lesions21–24 (Fig. 2). Except for benign lesions European Society of Gastrointestinal Endoscopy (ESGE) Guideline for Endoscopic Submucosal Dissection from 2015 recommends ESD for superficial esophageal squamous cell cancers without submucosal involvement, Barrett’s esophagus neoplasia, gastric superficial neoplastic lesions with very low risk of lymph node metastasis, and colorectal lesions that cannot be radically resected by snare-base procedures. 25

Submucosal lesion-leiomyoma of the esophagus (before excision).
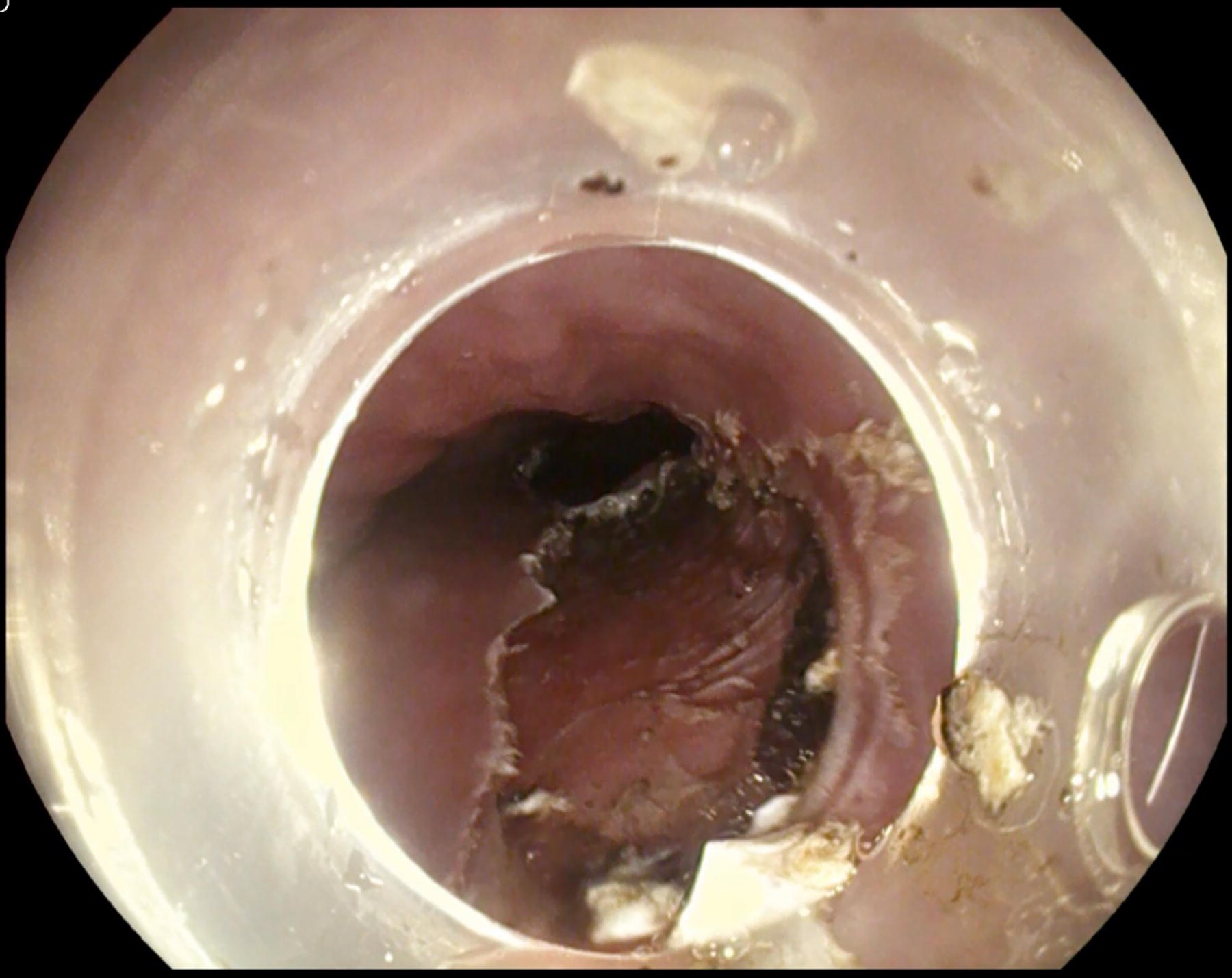
Submucosal lesion-leiomyoma of the esophagus (excision completed).
The data published each year from single-center and multicenter experience and case series from all around the world are a valuable source of information for improvement of outcomes in this group of patients. In this publication we present our experience and outcomes of ESD procedures performed in 100 patients.
Methods
The data of 100 patients who underwent ESD procedure between January 2, 2020, and June 30, 2023, at the Department of General and Transplant Surgery, Medical University of Lodz, Poland, due to esophageal, gastric, duodenal, and colorectal laterally spreading tumors (LST) of mucosa larger than 20 mm, gastrointestinal neuroectodermal tumors (GNETs) smaller than 20 mm, and slightly depressed lesions smaller than 20 with a risk of submucosal invasion <200 μm (SM1) (Paris 0-IIc) were collected retrospectively and analyzed. Selected cases of patients with submucosal esophageal and gastric lesions were also included in this group.
The endoscopist performing ESD in this group of patients has undergone initial ESD training on ex vivo and in vivo models and then completed an internship on ESD training in a reference center. Moreover, he had vast previous experience in EMR in the GI tract having performed over 300 EMR procedures prior to.
ESD was performed in an intravenous sedation using 5 mg of midazolam, 100 µg of fentanyl, and continuous intravenous infusion of deksmedetomidynum. Patients heart rate, blood pressure, and saturation were monitored continuously during the procedure. Patients were placed on their back or left side, although during some procedures the position was changed to the right side of the patient to obtain better approach to the lesion (mainly in cases of lesions located in the colon).
PENTAX Medical EG-2990i gastroscope and PENTAX Medical EC38-i10F2 colonoscope with carbon dioxide (CO2) insufflation were used during ESD procedures. Narrow-band imaging (NBI) of the lesions was performed with PENTAX Medical i-scan optical enhancement (OE) in every case just before the dissection to re-evaluate the indication for ESD. Submucosal injection of 15% mannitol or 10% Dextran solution stained with indigo carmine was always used for the elevation of the lesion. Nonlifting sign (meaning failure to achieve lesion elevation with a submucosal injection) was the reason for abandoning the pursuit for performing the ESD procedure.
Dissection was performed with a blade electrosurgical endoscopic knife with a blade length of 1.5 mm (PENTAX Medical, Splash M-Knife). The endoscope was equipped with a distal, straight, transparent silicone cap to facilitate dissection (Olympus, distal attachment cap) using coagulation forceps (Olympus, electrosurgical hemostatic forceps FD-411UR) and hemostatic clips (JIUHONG, Disposable Endoscopic Hemoclip 16 mm JHY-CD16-25–230).
Dissection of esophageal, gastric, and duodenal lesions was performed by circular incision (mucotomy) of the mucosa around the lesion and then gradual dissection in the submucosa. In these cases, the lesions were marked before excision with coagulation (ERBE VIO 300D, Forced Coagulation 20 Watt) with an appropriate margin of unaltered mucosa. In colorectal lesions the tunneling technique was used with the primary dissection of the entire lesion from the muscularis through a small mucotomy and then cutting it off from the surrounding mucosa.
Medical history, institutional endoscopic database, and histopathological reports were analyzed and included in this study. All patients underwent diagnostic gastroscopy or colonoscopy before the procedure showing no signs of invasive cancer. Collected data were analyzed due to age and gender of the patients, location and size of the lesion, classification (Paris, LST), duration of a procedure, additional procedures, complications, resection margin, histopathological findings, and early and late complications.
This retrospective study is not a medical experiment or a clinical trial performed on a patient; therefore, it did not require an Ethics Committee approval.
Results
A total of 42 male and 58 female patients in the median age of 64 years (range, 31–89 years) underwent ESD procedure between January 2020 and June 2023 in our department.
Every lesion was dissected using the ESD technique. Mean duration of the procedure was 66 minutes (range, 25–185 minutes). Tumors were located in esophagus in 8 cases (8%), stomach in 25 cases (25%), duodenum in 1 case (1%), and colon in 66 cases (66%). In colon lesions were located in: cecum (6), ascending colon (9), hepatic flexure (2), transverse colon (9), splenic flexure (3), descending colon (5), sigmoid (15), and rectum (12). Radical resection was achieved in 98 cases (98%). Of the patients, 2 were qualified for surgical resection due to muscular layer infiltration (2 sigmoid lesions). All lesions were measured in 2 dimensions in postprocedural course. Average size of dissection lesions was 26 × 19 mm. The biggest one was 60 × 60 mm (sigmoid adenoma), and smallest one was 5 × 5 mm (GNET) (Table 1).
Localization, Size and Type of Dissected Lesions, and Radical Resection Rate
In 59 patients (59%) the resection bed was closed with clips; in 7 cases (7%), coagulation was used to achieve proper hemostasis. In the rest of procedure, endo-loop (2), hot-biopsy (2), and stitching (1) were used for proper ensuring of mucosal defect (Table 2).
Devices and Procedures Used for Hemostasis after Dissected Lesion
Perforation of the wall occurred in 9 cases (2 cecum, 2 sigmoid colon, 2 splenic flexure, 1 stomach, 1 ascending colon, 1 transverse colon) and in 7 cases was successfully managed with clipping (microperforation). In 2 cases sigmoidectomy was necessary (Table 3). One patient required endoscopic clipping of bleeding vessel in the bed after dissection of sigmoid tumor due to hemorrhage in postprocedural course (day 1).
Perforation Rate and Therapeutic Procedure
Histopathological examination revealed adenoma in 88 cases, GNET in 6 cases, carcinoma in situ in 5 cases, and leiomyoma in 1 case (Table 4).
Histopathological Findings of Dissected Lesions
Discussion
ESGE Guideline published in 2015 recommended ESD for en bloc resection of superficial squamous cell carcinoma (SCC) of esophagus (especially larger than 10 mm) and Barrett’s esophagus cancer in lesions larger than 15 mm (as well as poorly lifting tumors and tumors at risk for submucosal invasion). 25 Update of ESGE Guidelines from 2022 extends these recommendations for most superficial SCC of esophagus and Barrett’s cancer lesions >20 mm, in suspicion of submucosal invasion (Paris type 0-Is, 0-IIc) and for lesions in fibrotic areas. 26 Following these guidelines we performed 8 ESD of esophageal lesions, which were adenomas in 5 cases, Barrett’s cancer in 2 cases, and leiomyoma in 1 case. The outcome of these procedures was satisfactory. In two patients, coagulation was used for proper hemostasis. No clipping or other procedures were used to avoid postprocedural stenosis. The risk of esophageal stricture is also increased if a complete round resection of the esophageal mucosa is performed. We achieved 100% of R0 resection rate with lack of early and late complications, and these results inspire optimism for further research. Radical resection margin and en bloc resection rate are being estimated in literature for 90% and 70%–88% in large groups of patients, respectively.7–12
In case of gastric lesions ESGE recommends ESD for intramucosal carcinoma or dysplastic lesions of any size. Exception is made for lesions with ulceration, which should not be dissected endoscopically if larger than 30 mm. Adenocarcinomas should be individually considered for ESD depending on size, depth, and differentiation—≤30 mm for superficial, submucosal SM1, well-differentiated and ≤20 mm for intramucosal and poorly differentiated. In our group there were 25 patients with gastric lesions—19 of them revealed as adenomas and 6 as GNETs. Every tumor was resected with radical margins (R0). Clipping, coagulation, endo-loop, and hot-biopsy were used to ensure the bed after dissection and achieve proper hemostasis. No early or late complication occurred in this group of patients. Our results are corresponding with current scientific reports—radical resection margin and en bloc resection are being estimated for 75%–80% and >90%, respectively.13–16
ESD of lesions located in duodenum or small intestine is not recommended by ESGE due to high risk of perforation accounting for 10%–37.5%. This risk is especially increased for lesions localized distal to ampulla of Vater. Radical resection rate varies significantly depending on the experience of an endoscopic center—it is estimated at 19.4%–93.9%.27,28 Patient with duodenal lesions should be qualified for ESD very carefully by endoscopists experienced in this kind of procedures taking into account the balance of potential losses and benefits. 26 Our patients had the lesion localized in the duodenal bulb, proximal to the ampulla of Vater with the diameter of 20 mm and Paris type 0-IIa+IIc. ESD of this lesion was successful, with radical resection margin and no early or late complication. Proper ensure of the bed after the dissection was achieved with endo-loop device supported by clipping.
Most of our patients underwent ESD for colorectal lesions (66%)—especially in left colon and rectum. Endoscopic dissection in these parts of GI tract is associated with higher complication rate (perforation) due to thinner wall in comparison with esophagus or stomach. 26 Due to current knowledge perforation rate is estimated for 5.2% and bleeding rate for 2.7% in this kind of procedures. Radical resection rate and en bloc resection rate for colorectal lesions are estimated to be 82.9% and 91%, respectively. 29 We achieved R0 resection rate in 97% of cases—2 patients with incomplete excision of sigmoid tumors were qualified for laparotomy. Complications occurred in 8 patients—perforation in 7 and postprocedural bleeding in 1, which account for 12.1% and 1.5%, respectively.
Our experience shows that ESD of lesions localized in sigmoid is associated with lower R0 resection rate (86.7%) and higher risk of perforation requiring surgical treatment (laparotomy) compared with lesions in different locations. This should be considered by endoscopists during learning process, and lesions with lower risk of complications should be qualified for ESD procedure at the beginning of the learning curve.
Conclusion
Implementation of ESD to clinical practice gives the opportunity for minimally invasive, radical treatment of benign, premalignant, and early neoplastic lesions of GI tract in selected group of patients. Experienced endoscopists, following current guidelines and standardized process of qualification, are crucial to minimize the risk of severe complications.
Footnotes
Authors’ Contributions
W.C.: Study Design, Data Collection, Statistical Analysis, Data Interpretation, Article Preparation, and Literature Search. T.K.: Study Design, Data Collection, Statistical Analysis, Data Interpretation, and Article Preparation. A.D.: Data Interpretation and Literature Search. P.H.: Data Collection and Literature Search. J.S.: Study Design, Statistical Analysis, and Literature Search.
Institutional Review Board Ethics Approval
This retrospective study is not a medical experiment or a clinical trial performed on a patient; therefore, it did not require an Ethics Committee approval.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.