
Abstract
Objectives:
The primary objective of this study was to evaluate the safety and efficacy of the enhanced recovery after surgery (ERAS) protocol in cholecystectomy, comparing it with standard care.
Methods:
A comprehensive literature search was conducted in December 2023, using globally recognized databases such as PubMed, Embase, and the Cochrane Library. Various parameters were compared using Review Manager software. This study was duly registered with PROSPERO (CRD420223).
Results:
The meta-analysis included nine studies, encompassing a total of 1920 patients. The findings revealed that the ERAS group, in comparison to traditional care, experienced shorter hospitalization periods (weighted mean difference [WMD]: −1.23, 95% confidence interval [CI]: −1.98 to −0.47; P = .001), lower visual analog scale at 24 hours (WMD: −1.10, 95% CI: −1.30 to −0.90; P < .00001), faster time to first flatus (WMD: −4.48, 95% CI: −4.50 to −4.46; P < .00001), and reduced operative times (WMD: −9.94, 95% CI: −17.88 to −0.96; P = .03). In addition, there was a notable decrease in instances of postoperative nausea and vomiting (odds ratio [OR]: 0.46, 95% CI: 0.28 to 0.74; P = .002). No significant differences were observed in readmission rates, blood loss, postoperative complications, or bile leakage between the two care methods.
Conclusions:
This study substantiates that the ERAS protocol is an advantageous perioperative care strategy for patients undergoing cholecystectomy. It significantly outperforms traditional care in reducing the length of stay, decreasing the likelihood of postoperative nausea/vomiting, alleviating postoperative pain, and accelerating the time to the first flatus. These findings highlight the effectiveness of ERAS in enhancing patient outcomes in cholecystectomy.
Introduction
Since the introduction of laparoscopic cholecystectomy (LC) in 1985, it has become the preferred approach for benign gallbladder conditions, noted for its reduced postoperative discomfort, shorter hospital stays, and faster return to normal activities.1,2 However, LC has its complications, such as postoperative nausea and vomiting (PONV) and acute pain, which can exacerbate cardiovascular and respiratory issues in patients with pre-existing conditions, potentially extending hospitalization and delaying recovery. 3 Therefore, minimizing surgical trauma and enhancing postoperative rehabilitation are crucial objectives for health care professionals.
In 1997, Professor Kehlet 4 of the University of Copenhagen proposed the enhanced recovery after surgery (ERAS) concept, prioritizing a comprehensive, evidence-based, and patient-focused approach to perioperative care. This method encompasses preoperative steps (including counseling, carbohydrate loading, and necessary bowel preparation), intraoperative strategies (such as thrombosis prevention, antibiotic prophylaxis, temperature control, precise fluid replacement, and the selection of optimal surgical techniques and incisions), and postoperative care (emphasizing effective pain management, early removal of tubes and catheters, prompt physical activity, and the start of enteral nutrition). 5 ERAS aims to reduce surgical risks, decrease hospital stays, and enhance recovery outcomes.6,7
Recent studies suggest that ERAS protocols can significantly improve patient recovery and shorten length of stay by optimizing pain management, reducing stress, encouraging early feeding, and promoting mobility. However, the effectiveness of ERAS compared to traditional care in cholecystectomy patients remains underresearched. 8 This article aims to assess the safety and efficacy of the ERAS regimen in cholecystectomy versus traditional care.
Literature search
This research adhered to the guidelines outlined in PRISMA 9 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and was pre-registered in the PROSPERO database CRD42024499462). For the systematic review, two independent reviewers (Q.J. and G.L.Y.) scrutinized the included articles. The literature search, confined to English language publications, was conducted up to December 1, 2023, using databases such as PubMed, Embase, and the Cochrane Library. Search terms included Medical Subject Headings (MeSH) and keywords such as “Cholecystectomy,” “Enhanced Recovery After Surgery,” “traditional care,” and “Systematic Nursing.” In addition, a manual search of pertinent references was undertaken to ensure comprehensive coverage and prevent any oversight.
Inclusion and exclusion criteria
In this study, the PICOS framework was utilized to systematically address the clinical questions. Patient (P): The patient group comprised individuals undergoing cholecystectomy for gallbladder disease. Intervention (I): The intervention examined was the Enhanced Recovery After Surgery (ERAS) protocol. Comparison (C): This was compared with the Usual Care given to patients undergoing the same surgical procedure. Outcome (O): The primary outcomes measured were the length of hospital stay and the 24-hour pain score, assessed using the visual analogue scale. This scale is a 10-cm line representing pain intensity from 0 (no pain) to 10 (worst possible pain), where patients mark their level of pain. The time of the first gas after operation was also recorded. Secondary outcomes included operative time, instances of PONV, readmission rates, blood loss, postoperative complications, and postoperative bile leakage. Study (S): The types of studies included were cohort studies, case–control studies, and randomized controlled trials (RCTs). Exclusion criteria were set for non-English language articles, noncomparative studies, studies involving nonadult subjects, conference abstracts, case reports, letters, and any other unpublished literature.
Data extraction was conducted independently by two reviewers, focusing on general information like the first author, year of publication, country of origin, and population characteristics such as age, sex, and body mass index (BMI), along with details about primary and secondary outcomes.
Study screening and selection
All retrieved records were manually screened by two independent authors, Q.J. and G.L.Y. In instances where Q.J. and G.L.Y. did not agree, a third author, Z.P., was consulted to reach a consensus. The inclusion of studies was guided by the PICOS criteria, encompassing retrospective, prospective, nonrandomized, and randomized studies. However, reviews, conference abstracts, case reports, letters to editors, and editorials were excluded from consideration. Articles deemed potentially relevant to the study’s objectives were selected for further scrutiny through a full-text review.
Statistical analysis
In this study, statistical analysis was carried out using Review Manager V5.4.1 software, developed by the Cochrane Collaboration in Oxford, UK. The results were presented through 95% confidence intervals (CIs) and odds ratios (ORs) for dichotomous variables, and weighted mean differences (WMDs) for continuous variables. For studies that reported only medians, quartiles, or ranges of extreme values, their data were converted to means and standard deviations (SDs) using conversion tables provided by McGrath. 10 The meta-analysis was conducted using the Mantel-Haenszel method for dichotomous variables and the inverse variance method for continuous variables. Given the anticipated heterogeneity across trials, random-effect models were employed in all analyses. The I^2 statistic was used to assess heterogeneity among studies, with 0%–40% indicating mild heterogeneity, 40%–60% moderate, 60%–75% large, and 75%–100% high heterogeneity. 11 Statistical significance was set at P < .05.
Bias risk assessment
The Cochrane risk of bias tool was used to evaluate potential biases in the included RCTs. This tool examines five domains: Randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each domain was rated as low, unclear, or high risk. 12 For nonrandomized controlled studies, the Newcastle–Ottawa Scale (NOS) was used, employing a star system to assess study quality across three areas: Selection of study groups, comparability of groups, and ascertainment of exposure or outcome.
Sensitivity analysis
The “leave-one-out” method was used for sensitivity analysis, systematically excluding one study at a time from the pooled effect to observe the impact on overall results. This method identifies if any individual study disproportionately influences the pooled estimates, assessing the robustness of the findings. However, when fewer than four studies were involved, this analysis was limited due to the significant reduction in the data pool when a single study was removed.
Publication bias
Publication bias analysis was not conducted as the power of the test was insufficient when ten or fewer studies were included. This decision was based on the recognition that a smaller number of studies could lead to unreliable conclusions regarding publication bias.13,14
Result
Baseline characteristics
The initial search yielded 100 articles, from which five duplicates were removed, leaving 95 for screening. Upon title and abstract review, 78 were deemed irrelevant to the study objectives and excluded. The remaining 17 underwent full-text screening, leading to the exclusion of eight articles due to issues like lack of data specificity, nonadult subjects, missing data, or incorrect interventions. Consequently, nine studies15–23 were selected for inclusion in the meta-analysis. These studies originated from various countries, including Pakistan, France, Egypt, China, India, and Russia. Among them, five were retrospective, and four were RCTs. Notably, in Kamel’s study, the trials were categorized into four groups based on the type of cholecystectomy and care received. However, for this meta-analysis, only patients who underwent LC under either ERAS or traditional care were considered, in line with the majority of included studies focusing on laparoscopic procedures.
The meta-analysis encompassed data from 1920 patients, with 783 receiving ERAS care and 1137 under traditional care. The PRISMA flow diagram detailing the study selection process is illustrated in Figure 1. A summary of included studies’ characteristics and perioperative outcomes are presented in Tables 1 and 2, respectively. Table 3 indicates no significant statistical difference between the studies in terms of age (P = .66), BMI (P = .15), and male participant count (P = .86), suggesting that the characteristics and variables of the included studies were comparable. For studies such as Nechay’s, where continuous variables were reported as quartiles, data were converted to means and standard deviations using McGrath’s data conversion table to ensure consistency and comparability in the meta-analysis.
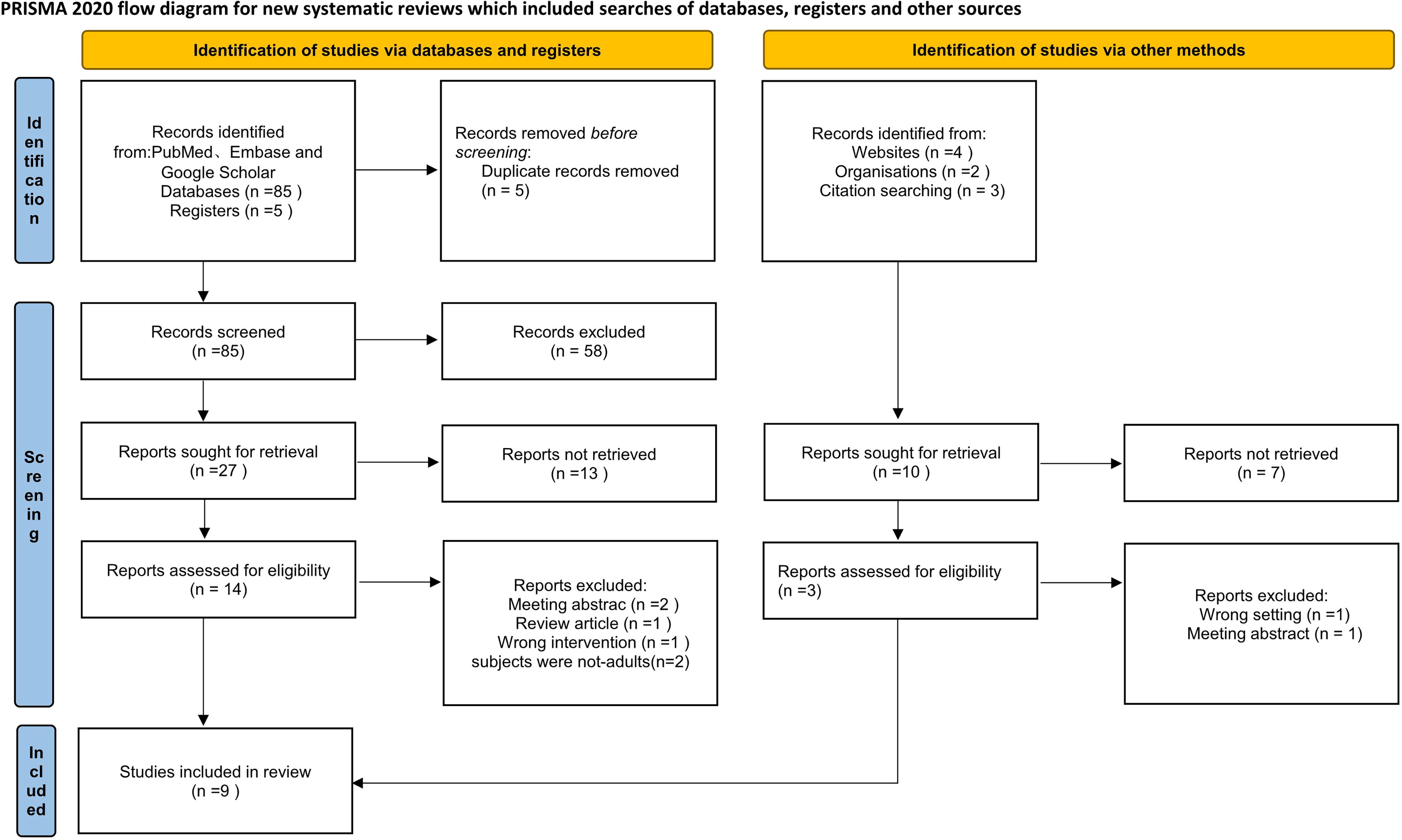
PRISMA flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Demographic Characteristics of the Included Studies
ERAS, enhanced recovery after surgery; SD, standard deviation; RCT, randomized controlled trial; BMi, body mass index.
The Demographics of the Studies
LOS, length of stay; PONV, postoperative nausea and vomiting; VAS, visual analog scale; POC, postoperative complication; ERAS, enhanced recovery after surgery; BS, recovery time of bowel sounds; FS, the time of first gas after operation; SD, standard deviation.
The Demographics of the Studies
WMD: weighted mean difference, OR odds ratio, Cl confidence interval; BMI, body mass index.
Assessment of quality
In this analysis, five retrospective studies were evaluated using the NOS for quality assessment. A score of 6 stars or higher on the NOS scale was designated as the benchmark for high-quality literature. All five of the retrospective studies met this criterion, achieving a score of ≥6 stars, indicating their high quality. The specifics of the quality assessment for these cohort studies are detailed in Table 4. In addition, four articles in this study were RCTs, assessed using the Cochrane risk of bias assessment tool. Of these, one article was determined to be of moderate quality, while the remaining three were classified as high quality. This indicates a general adherence to stringent study design and reporting standards among the majority of RCTs included. The quality assessment details for these RCT studies are visually represented in Figure 2.
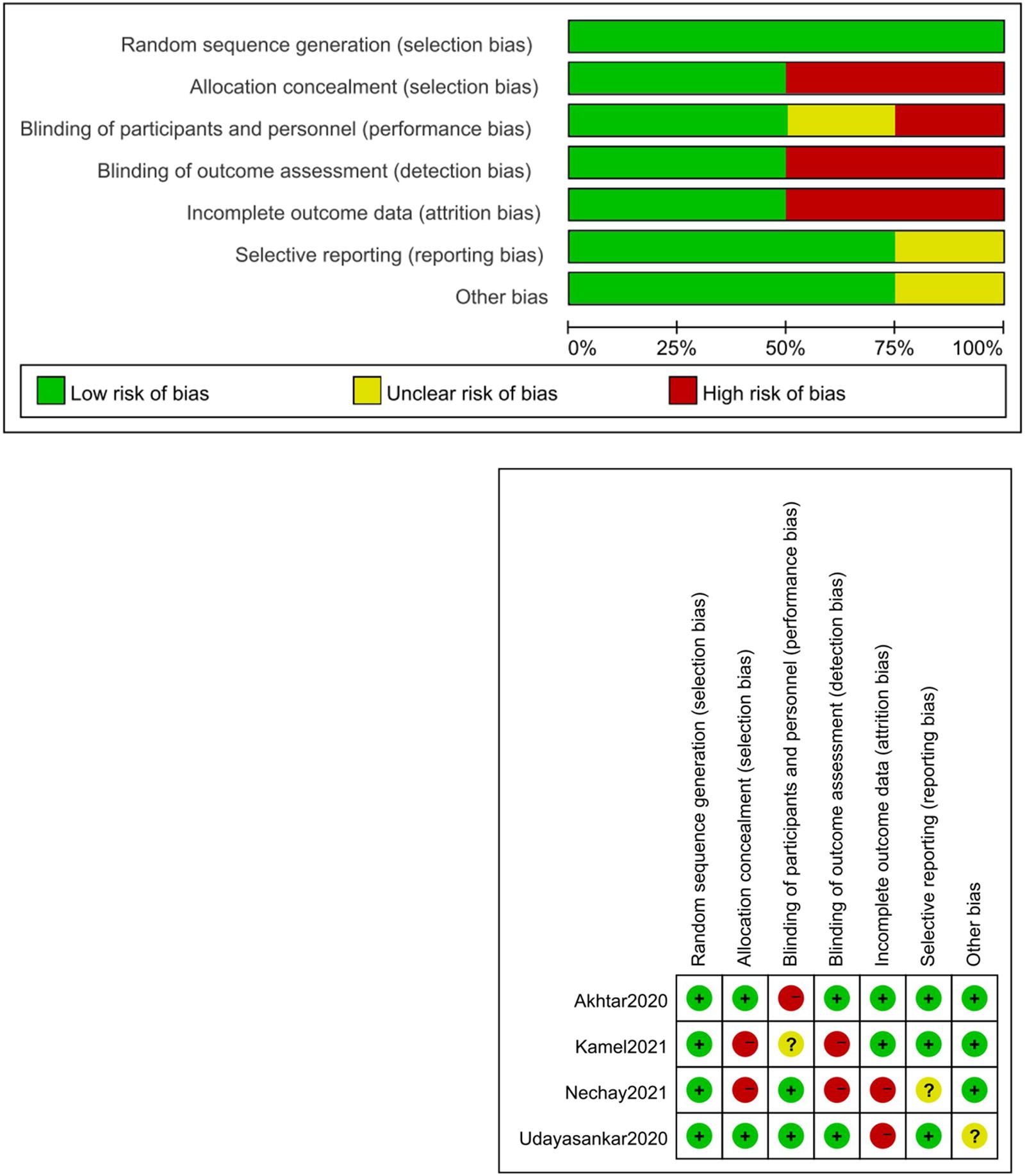
Quality assessment of randomized controlled studies.
Study Quality of Case–Control Studies Based on the Newcastle–Ottawa Scale (NOS)
1: Representativeness of the exposed cohort; 2: Selection of the nonexposed cohort; 3: Assessment of exposure; 4: Demonstration that outcome of interest was not present at the start of the study; 5: Comparability of cohorts based on the design or analysis; 6: Ascertainment of outcome; 7: Long enough follow-up for outcomes to occur; 8: Adequacy of follow-up of cohorts.
Primary outcome measures
Pooled analysis of the results of 5 studies showed that there were fewer days of length of stay in the ERAS group compared with the traditional care group (WMD: −1.23, 95% CI: −1.98, −0.47; P = .001) (Fig. 3A). Pooled analysis of the results of the three studies showed that the ERAS group had lower intraoperative 24-hour pain scores compared with the traditional care group (WMD: −1.10, 95% CI: −1.30, −0.90; P < .00001) (Fig. 3B). Pooled analysis of the results of the four studies showed that the time of the first gas after operation was shorter in the ERAS group compared with the traditional care group (WMD: −4.48, 95% CI: −4.50, −4.46; P < .00001) (Fig. 3C).

Secondary outcome measures
Pooled analysis of the results from six studies showed that the ERAS group had a shorter operative time compared to the traditional care group (WMD: −9.42, 95% CI: −17.88, −0.96; P = .03) (Fig. 4A). Pooled analysis of the results from five studies showed that there were fewer patients with PONV in the ERAS group compared with the traditional care group (OR: 0.46, 95% CI: 0.28, 0.74; P = .002) (Fig. 4B). However, there was no significant difference in the number of readmission (Fig. 4C), blood loss (Fig. 4D), postoperative complications (Fig. 4E), and postoperative bile leakage (Fig. 4F) between the two groups.

Sensibility analysis
In this meta-analysis, some results showed significant heterogeneity (I2 = 98% for length of hospital stay and I2 = 93% for operative time). We performed a sensitivity analysis of the target parameters to obtain stable conclusions. We used the leave-one-out approach to identify the source of heterogeneity from the pooled effect, and after each analysis was excluded one by one, we found no significant change in heterogeneity between the length of hospital stay and surgery in both analyses, and the results were stable. The number of patients with PONV and other statistically insignificant results showed no significant change in heterogeneity after performing sensitivity analysis, indicating that the results were robust.
Discussion
As people’s quality of life improves, there is a growing demand for high-quality health care. Patients and their families are increasingly concerned not just with the physical ailment but also with its psychological impact and overall quality of life. Studies have demonstrated that the ERAS protocol reduces postoperative complications and enhances recovery. For instance, a meta-analysis in colorectal surgery involving 16 randomized trials (2376 patients) revealed a 40% decrease in postoperative complications (RR = 0.6, 95% CI: 0.46–0.76). 24 Similarly, in pancreatic surgery, a meta-analysis of 14 nonrandomized studies indicated overall complication reduction (OR = 0.63, 95% CI: 0.54–0.74). 25 Ni et al. 26 found that ERAS in laparoscopic digestive system surgery leads to quicker recovery, shorter hospital stays, and fewer postoperative complications. Udayasankar 21 et al.’s randomized study of 50 elective LC patients demonstrated that the ERAS group experienced less anxiety, hunger, thirst, and fatigue, enhancing their overall perioperative comfort compared to traditional care. This study represents the first meta-analysis comparing perioperative outcomes between ERAS and conventional approaches in cholecystectomy.
Primary outcome measures
A comprehensive analysis of the results from the included studies demonstrates that the ERAS group exhibits certain advantages over the traditional care group in terms of hospital stay duration, 24-hour pain scores, and time to first flatus. Ahmad et al. 27 attributed the shortened length of stay to effective management of postoperative symptoms such as nausea, vomiting, reduced hematoma, and adequate pain control in their meta-analysis. In reality, several factors within the ERAS protocol contribute to patients’ recovery and reduce their time in the hospital.
In 2016, the ERAS Society issued its inaugural perioperative care guideline specifically for liver surgery, complementing the existing guidelines for other surgical specialties within the ERAS framework. This specific guideline comprises 23 key elements, including preoperative counseling, preoperative carbohydrate loading, perioperative nutrition, avoidance of bowel preparation, unconventional use of surgical drainage, thromboembolism prevention, antibiotic prophylaxis, minimally invasive techniques, intraoperative fluid restriction, multimodal analgesia, hypothermia prevention, early oral fluid intake, glycemic control, prevention of delayed gastric emptying, stimulation of defecation, early mobilization, prevention of PONV, fluid management, and systematic auditing. 28 Surgery can lead to the development of adverse psychological states, including anxiety or depression, which can negatively impact wound healing and physical function recovery. 29 Compared with the traditional care group, the ERAS group benefits from comprehensive preoperative education, enabling patients to have a fundamental understanding of their disease diagnosis, surgical procedures, perioperative management, prognosis, and more. This preoperative education alleviates preoperative tension, reduces psychological pressure, prepares patients for postoperative recovery, and promotes rehabilitation, while minimizing complications. This positive impact has also been confirmed by Zhao 30 et al.’s report and a randomized single-blind clinical trial conducted by José et al., 31 which included 74 patients and demonstrated a significant association between lower pain levels and the positive effects of preoperative education and comprehensive oral and written preoperative materials.
During surgery, maintaining optimal intraoperative temperature control and preventing hypothermia can reduce the incidence of postoperative infections, decrease intraoperative blood loss, and shorten postoperative anesthesia recovery time. In addition, monitoring central venous pressure and managing intraoperative fluid replacement effectively control circulating blood volume, reduce cardiac load, and prevent postoperative cardiac complications. 32 Measures such as using lower pressure pneumoperitoneum and unconventional placement of drainage tubes during surgery also promote faster postoperative recovery of gastrointestinal function and earlier patient ambulation. 33
The ERAS protocol employs multimodal analgesia for postoperative pain management, using a combination of opioids, nonsteroidal anti-inflammatory drugs, local incision infiltration anesthesia, intraspinal analgesia, and nerve blocks. This approach results in reduced postoperative pain and mitigates gastrointestinal depression, nausea, vomiting, and other adverse reactions commonly associated with strong opioids. 22 Roulin 34 et al.’s study highlights the benefits of early oral feeding, which preserves intestinal absorption, leading to higher collagen levels, positive nitrogen balance, accelerated wound healing, and reduced postoperative sepsis rates. In contrast to traditional nursing practices, ERAS advocates early postoperative eating, mechanical stimulation of the intestinal wall, promotion of defecation, shorter exhaust times, and reduced fluid replacement. Studies have shown that early resumption of a normal diet does not increase the incidence of vomiting and can reduce the occurrence of lung, abdominal, and incision infections, ultimately resulting in shorter hospital stays. Ensuring an adequate supply of glucose and amino acids is essential for normal protein synthesis, as the body requires sufficient protein to expedite wound repair and restore. 35
There is mounting evidence to suggest that implementing an ERAS clinical pathway can accelerate recovery and reduce hospital stays for patients undergoing surgery. This is achieved through multimodal strategies that encompass optimal pain relief, stress reduction, early nutrition, and early ambulation.
Secondary outcome measures
The analysis of data from the included studies shows that the ERAS group has certain advantages over traditional care in terms of operation time and the number of PONV incidents. Factors influencing operation time are varied, including patient age, gallbladder location, size, surgical complexity, and the surgeon’s experience and expertise. Although this summary suggests some benefits of ERAS in operation time, it is important to interpret these results cautiously, considering their multifactorial nature. Regarding PONV, other research indicates that ERAS protocols contribute to lower PONV rates due to better hydration and reduced opioid use, 36 findings that are consistent with our meta-analysis. In addition, ERAS patients tend to experience quicker gastrointestinal function recovery and faster post-surgery mobilization, attributed to improved preoperative education, intraoperative control, and postoperative management.
The combined results from the studies show no significant difference between ERAS and traditional care in terms of readmission rates, blood loss, postoperative complications, and bile leakage. In general, the ERAS protocol does not increase the incidence of complications or readmission. Pucher’s extensive meta-analysis, covering over half a million cholecystectomy patients, reported complication rates ranging from 1.6% to 5.3%, with severe cases such as bile duct injury accounting from 0.32% to 0.53%. 37 The mortality rate varied between 0.08% and 0.14%. 38 It is vital to consider a range of factors when evaluating complications and mortality rates, rather than attributing them solely to the type of care received.
In gynecological oncology, a meta-analysis of ERAS protocols showed similar outcomes, with no significant impact on readmission rates or complications, while reducing hospital stay length and cost. 37 However, a report from a single center involving over 900 consecutive patients indicated that the ERAS approach for colorectal cancer patients resulted in fewer complications and lower readmission rates. 39 Therefore, more comprehensive and high-quality clinical trials are necessary to further investigate which care model is more advantageous in outcome measures such as readmission rates and postoperative complications.
Limitations
First, this meta-analysis has some notable limitations. It included a limited number of prospective RCTs, had small overall sample sizes, and collected limited data. In Udayasankar et al.’s study, for example, only one outcome measure, namely PONV, was collected for analysis. This scarcity of data prevented further subgroup analysis, which could have helped identify the source of heterogeneity in the results. In addition, the parameters considered in this meta-analysis were insufficient. Crucial factors such as surgical costs and postoperative ambulation time were not subjected to further analysis, which represents a gap in the evaluation of the interventions. Finally, it is worth noting that surgical patient care pathways involve a multitude of medical professionals, including ambulatory physicians, surgical anesthesiologists, nurses, and postanesthesia care specialists. However, these diverse health care roles were not consistently reported or compared across multiple studies. This lack of uniformity in reporting may limit the generalizability of the findings.
Conclusion
After summarizing the findings, it was discovered that for patients with benign gallbladder conditions requiring cholecystectomy, enhanced postoperative recovery protocols have several advantages compared with traditional care. These advantages include a shorter hospital stay, reduced likelihood of PONV, alleviation of postoperative pain, and accelerated time to first flatus, among others. It is a worthwhile perioperative care strategy to implement in clinical practice. However, more high-quality clinical randomized trials are needed to further confirm its effectiveness.
Footnotes
Authors’ Contributions
All authors contributed to the conception and design of the study. Q.J. and G.L.Y. prepared the first draft and Z.W. and P.X. collected and analyzed the data. Z.P. critically revised important content. All authors commented on previous versions of the article. All authors read and approved the final article.
Data Availability Statement
The original contributions presented in the study are included in the article material, further inquiries can be directed to the corresponding author/s.
Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No funding was received for this article.