
Abstract
Background:
Today, laparoscopy is frequently used in abdominal emergencies such as acute appendicitis. There are several techniques used to close the appendiceal stump during laparoscopic appendectomy. We aimed to compare the use of handmade loop and Hem-o-lok used to close the appendiceal stump in public hospitals where resources are limited, in terms of surgical outcomes and cost.
Methods:
Between January 2020 and December 2022, patients for whom handmade loops and Hem-o-loks were used to close the appendiceal stump during laparoscopic appendectomy in our clinic were included in the study. There were a total of 638 patients (mean age: 33 ± 13.5 years, 325 females and 313 males) in the patient cohort. Demographic and clinical data, duration of surgery, complications, hospital stay, pathology reports, mortality, and cost of supplies were compared between the two groups.
Results:
There were 308 patients in the handmade loop group (160 females, 148 males, mean age: 33.7 years, range: 18–85 years) and 330 patients in the Hem-o-lok group (166 females, 164 males, mean age: 32.5 years, range: 18–89 years). There was no significant difference between the two groups for American Society of Anesthesiologists score, duration of symptom, hospital stay, intensive care unit stay, preoperative laboratory values, histopathological results, mortality, and morbidity (P > .05). The mean operation time was 48.76 ± 16.16 minutes in the handmade loop group and 40.53 ± 11.63 minutes in the Hem-o-lok group (p = 0.001). In terms of cost, the cost per case of Hem-o-lok group was about 25.8 times as much as the group that used sutures ($31 versus $1.2).
Conclusions:
Both methods can be used safely in laparoscopic appendectomy. The use of Hem-o-lok has no advantage other than shortening the operation time. However, it is costlier. Especially in peripheral hospitals where resources are limited, closing the appendiceal stump using a handmade loop is an easy, safe, and cost-effective method.
Introduction
Acute appendicitis is one of the most common surgical emergencies. Since it was first described by Semm et al. in 1983, laparoscopic appendectomy (LA) has been a popular and important alternative method in the treatment of acute appendicitis. 1 The advantages of LA over traditional open appendectomy include less postoperative pain, faster recovery, earlier initiation of dieting, shorter hospital stay, good cosmetic outcomes, early return to normal daily activities, and a reduced risk of developing surgical site infections. In addition, it has the advantage of better visualization of the abdominal cavity for pathologies. 2 However, there are also negative aspects such as high cost, long operation time, and high rate of intra-abdominal abscess.3,4
Closure of the appendiceal stump during laparoscopic appendectomy due to acute appendicitis is perhaps the most critical point of the surgery. 5 Many different methods have been described for closing the appendiceal stump. These methods include endoloop, titanium endoclips, nonabsorbable polymer clips (Hem-o-lok clips), stapler, knot pusher, extracorporeal or intracorporeal tying, and use of LigaSure®.6–8 In the literature, it is not clear which method is superior to the others. The available literature indicates the relative advantages and disadvantages of such methods in securing the appendiceal stump. The method used must be safe, easily accessible, and cost-effective.
In this study, we evaluated the fixation of the appendix base with an extracorporeal handmade loop with Hem-o-lok clips in terms of surgical outcomes, safety, and cost.
Materials and Methods
Patients who had undergone surgery with the LA method for acute appendicitis between January 2020 and December 2022 in the General Surgery Clinic of Tokat Gaziosmanpaşa University Faculty of Medicine were retrospectively examined and added to the data record. Due to the retrospective design of the study, ethical approval and informed consent have not been taken. However, the study was conducted in accordance with the Ethical Principles of Helsinki. Patients who had been operated with the diagnosis of acute appendicitis were screened at hospital database with International Classification of Disease (ICD) codes (K35, K35.31, K 35.3), and a patient cohort was formed. The patients whose appendiceal stump had been closed with an extracorporeal handmade loop and with Hem-o-lok method were divided into two groups. Group 1 had the patients who underwent Hem-o-lok, whereas Group 2 included the patients for whom extracorporeal handmade loops were made. The method of closure of the appendiceal stump, the choice of Hem-o-lok clip or handmade loop, depended on the surgeon’s wishes. However, in edematous and thick appendicitis cases, the handmade loop was preferred due to concerns about clip safety.
Patients under 18 years of age, patients who had perforated appendicitis with diffuse peritonitis, appendiceal mass or abscess diagnosed preoperatively, severe sepsis with laparotomy indications, and pregnant patients were excluded from the study.
During the study period, a total of 660 patients underwent laparoscopic appendectomy. Five patients under the age of 18, 6 patients with pregnant appendicitis, 3 patients with perforation and severe peritonitis, and 8 patients whose stump appendicitis was closed with methods other than the two used in the study were excluded from the study. Our alternative stump closure method was laparoscopic stapler and endoloop. Consequently, a total of 638 patients formed the study cohort. There were 330 patients in Group 1 and 308 patients in Group 2. The most important outcome was the stump leakage and cost. Other outcomes were duration of operation, hospital and intensive care unit stays, reoperation, and postoperative complications (intra-abdominal abscess, wound infection, ileus, bleeding, and so on).
In addition, physical examination findings, laboratory values such as white blood cell (WBC) and C-reactive protein (CRP) when they were admitted to the emergency service, demographic data, symptom duration, American Society of Anesthesiologists (ASA) score, intraoperative findings, and pathology report were recorded for comparison. Purulent fluid collection in the abdomen was defined as intra-abdominal abscess. Purulent discharge from the incision or erythema at the incision site was defined as surgical wound infection.
Cost comparison was made between a cartridge Hem-o-lok clip (consisting of six clips) and a single pack of Vicryl sutures to create a handmade loop to be used per case. (Current prices were obtained from our hospital’s medical equipment purchasing office.)
Surgical procedure
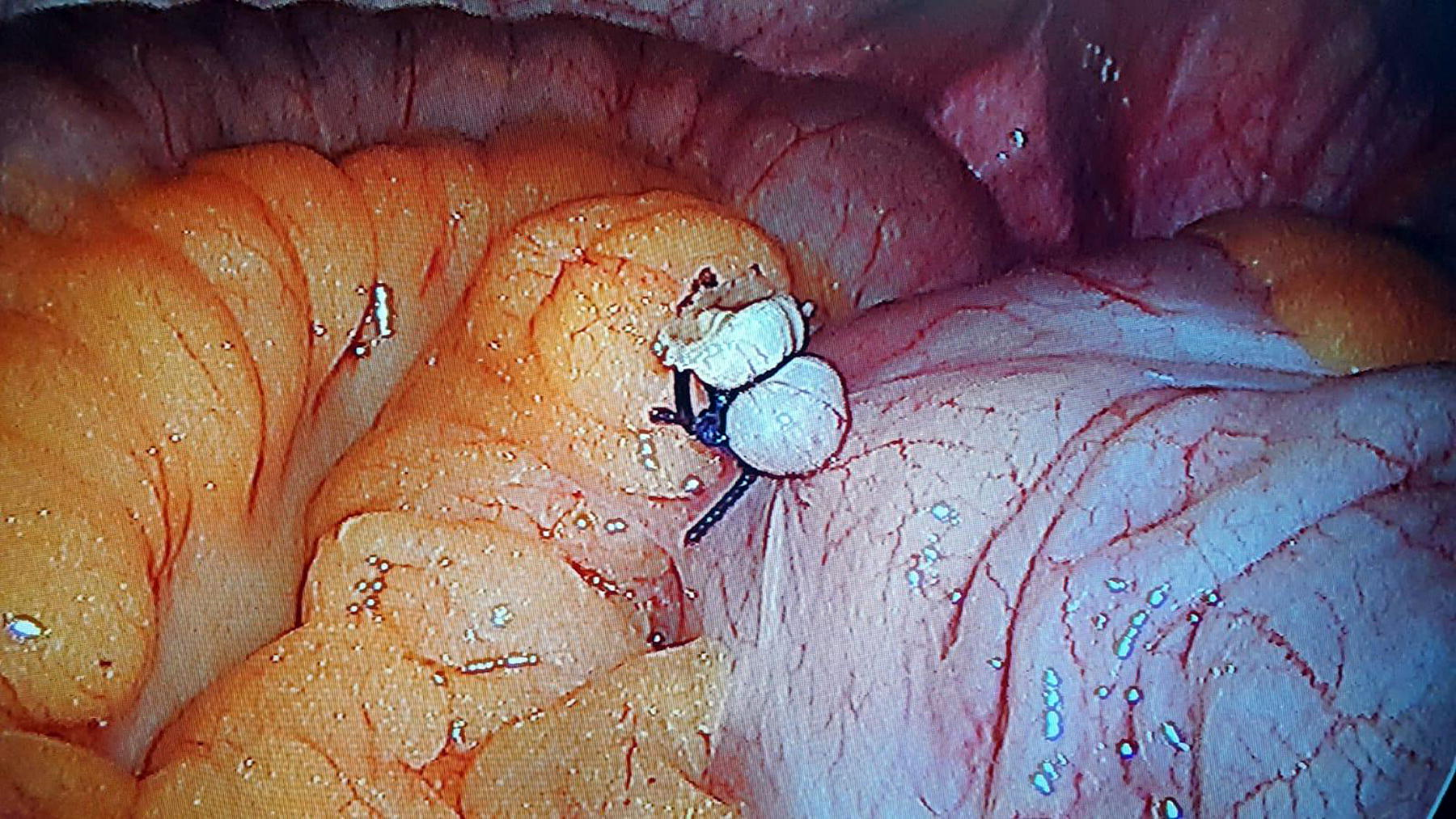
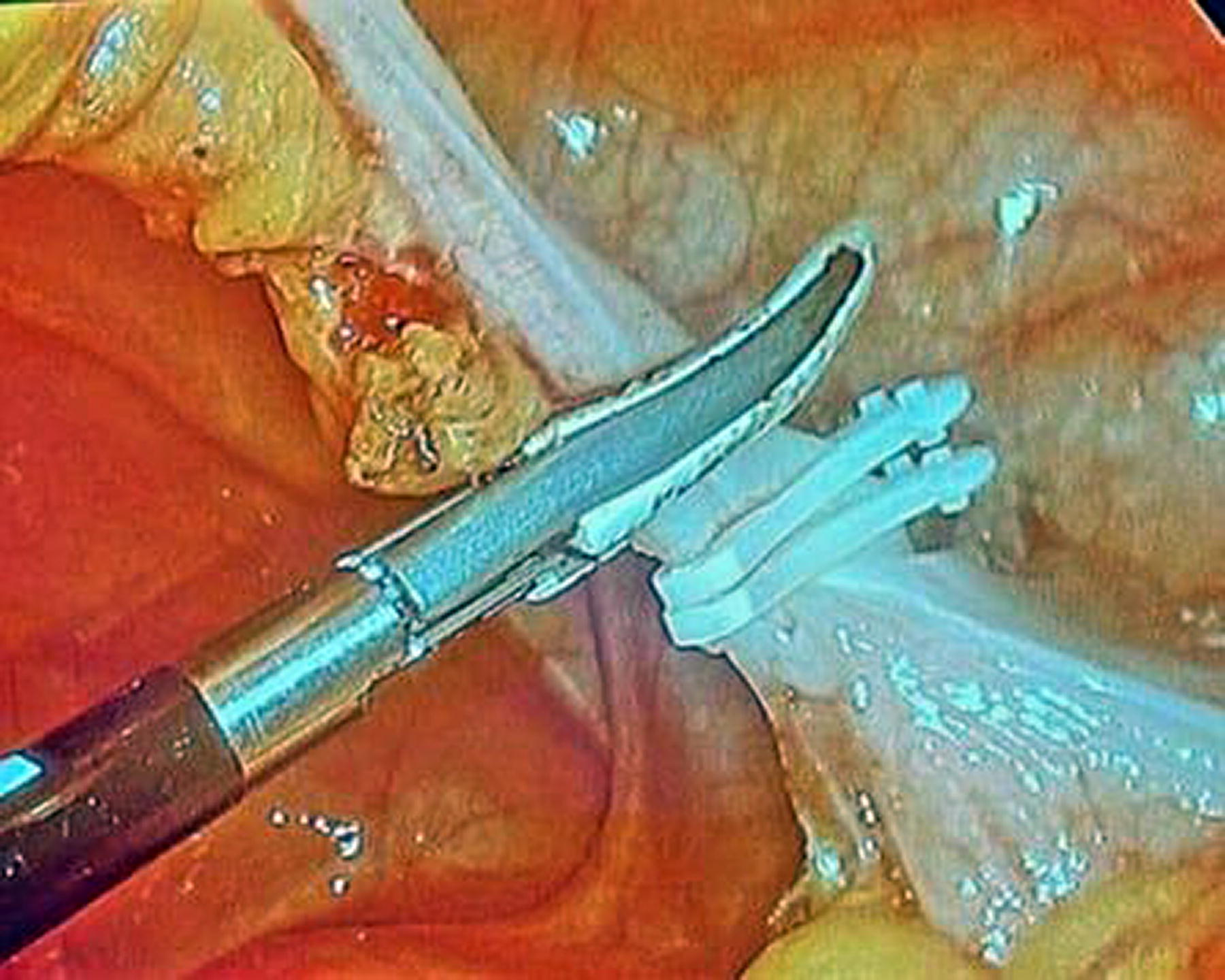
All surgeries were performed by the same surgical team. All patients were administered preoperative antibiotic prophylaxis (1 g of cefazolin). All operations were performed using the classical three-port technique with three conventional laparoscopic trocars. Pneumoperitoneum was created by closed or open technique through supraumbilical incision. One 10 mm trocar was inserted (30°) through an underbelly incision for the camera, the second 5 mm trocar was placed through a suprapubic incision, and the third 5/10 mm trocar was inserted through a right lower quadrant middle clavicular incision. After pneumoperitoneum and standard exploration were secured, the patient was placed in 20° Trendelenburg position and 15° left tilt. Appendix meso was dissected with cautery and/or vessel sealing devices. Then, the loop was prepared using 2/0 Vicryl for the patients in the extracorporeal handmade loop group. The formula “1:3:1” was used. First, a loop was made around a post and then a simple knot was made. The short working end was then rotated three times around the two wires of the loop. The node was completed by making a single turn around the perpendicular part of the working tip inside the stitch and making a half-hanger. Finally, the loop was tightened and checked whether there was a slippage (Fig. 1, Supplementary Material Video S1). The loop prepared outside the abdominal cavity was advanced into the abdomen through the suprapubic 5 mm trocar hole and placed at the root of the appendix. The short end that stayed inside was held with a laparoscopic grasper. The long end that stayed outside was pulled simultaneously by the assistant, and the knot was placed at the appendix root. The stump in this group was closed with two knots (Fig. 2). Nonabsorbable L or XL polymeric clip (Weck® Hem-o-lok polymer ligation system, Teleflex Medical, NC, USA) was used for the patients in the Hem-o-lok® group. One of the clips was placed on the appendiceal stump with the clip applicator. Another clip was placed 2–3 mm distal (Fig. 3). The appendix was cut a few millimeters distal into double Hem-o-lok clips or double handmade loop ligatures. After both techniques, the specimen was taken out with the help of a bag made with sterile gloves. When necessary, a silicone drain was left in the abdomen.

Handmade loop preparation technique.
Handmade extracorporeal knotting on appendiceal stump.
Hem-o-lok clips on appendiceal stump.
Statistical analyses
IBM SPSS Statistics for Windows (Version 21, IBM Corp., Armonk, NY, USA) was used for all analyses. The two groups were compared using the independent samples t-test for normally distributed continuous variables and the Mann–Whitney U-test for non-normally distributed continuous variables. Continuous variables with normal distribution were expressed as mean ± SD, while those without normal distribution were expressed as median values. The χ2 test was used for comparison of categorical variables. A P value <.05 was considered statistically significant.
Results
The study group consisted of a total of 638 patients, and 325 patients were female and 313 were male. The mean age of the patients was 33 ± 13.5 years. The handmade loop group consisted of 308 patients (160 females and 148 males, mean age: 33.7 years, range: 18–85 years), and 330 patients (166 females and 164 males, mean age: 32.5 years, range: 18–89 years) were in the Hem-o-lok group.
There was no significant difference between the two groups for average age, gender distribution, ASA score, duration of symptoms, hospital stay, intensive care unit stay, appendicitis diameters, and preoperative laboratory values of WBC and CRP (P > .05). The patients’ demographics, clinical data, and surgical outcomes are shown in Table 1.
Demographic Data, ASA Score, Laboratory Values, Hospital and Intensive Care Unit Stays, and Cost Comparisons of the Study Groups
CRP, C-reactive protein; WBC, white blood cell.
In 3 patients in Hem-o-lok group, the handmade loop method was used due to the large appendix diameter of 10 mm and intense inflammation.
Histopathologically, acute appendicitis was the majority in both groups. There was no significant difference (P = .47), but the number of patients with perforated appendicitis was higher in the handmade loop group (n = 32 versus 21). Malignancy was detected in 2 patients in the Hem-o-lok group and in 1 patient in the handmade loop group (Table 2).
Histopathological Parameters, Mean Operative Time, Mortality, and Morbidity Rates in the Study Groups
Significant.
The mean operation time was 48.76 ± 16.16 minutes in the handmade loop group and 40.53 ± 11.63 minutes in the Hem-o-lok group, and the difference was significant (P < .001) (Table 2, Fig. 4).

Operation time of the study groups.
Intraoperative bleeding occurred in a patient with perforated appendicitis in the handmade loop group, and the bleeding was stopped before switching to the open method. There were no intraoperative complications in the Hem-o-lok group, and the difference was not significant (P = .47).
Our total postoperative complication rate was 2.5% (n = 16). There was no significant difference in both groups (P = .58). The most common complication was superficial wound infection (n = 8), which was treated with daily wound dressing, debridement, and antibiotic therapy. Intra-abdominal abscess developed in 2 patients in the Hem-o-lok group and in 1 patient in the handmade loop group. Two patients were successfully treated for percutaneous abscess drainage. Percutaneous drainage was not successful in a patient (18 years of age, female) in the handmade loop group due to diffuse abscess. The patient who developed peritonitis symptoms and sepsis was operated. In the operation, the appendiceal stump was intact, and the pericecal abscess was drained. A total of 5 patients developed ileus in the postoperative period. These patients were treated nonoperatively with nasogastric decompression and intravenous fluid therapy (Table 2).
One patient (79 years old, male) with coronary artery disease and cirrhosis diagnoses in the handmade loop group died on the 9th postoperative day. The difference for mortality rate of the two groups was not significant in both groups (P = .59)
Discussion
Today, with the introduction of laparoscopic methods into surgery, the development of industrial instruments, and surgical experiences, many gastrointestinal surgical procedures can be performed laparoscopically. Laparoscopy has also been used in the treatment of acute appendicitis, and studies have been conducted on its advantages and disadvantages. 9 The important critical point in LA is how to close the appendiceal stump, because stump closure with an inadequate technique can produce very serious complications, which can result in stump leakage and subsequent intra-abdominal abscess, peritonitis, and death. 10
In open appendectomy, the stump can be easily fixed with a simple ligation or, in complicated cases, with purse string suture. That may not always be easy in LA. For this reason, many techniques such as endoloop, intra- or extracorporeal simple tie, metal or polymeric clips, and endostaplers have been described.
In fact, at present, endoloops and endostaplers seem to be the most common method used to close the appendiceal stump. Both methods have achieved good outcomes in many studies.11,12 While endoloops are recommended due to their cost efficiency, there are studies reporting that endostaplers should be used in a way to include a part of cecum in cases with perforation at the base of the cecum. 13
However, in developing countries such as ours, the cost of materials used in laparoscopic surgeries is quite high. Handmade loops have been described as an easy, safe, and inexpensive method that has been proven to be safe in previous studies.14,15 In addition, the cost is lower compared to other methods such as endoloop and stapler. It can be easily done with a single silk or Vicryl suture. In the conditions of our country, the cost is only $1.2, which is one of the most important reasons that makes this method preferable instead of endoloop, which costs $35, and endostapler, which costs $60. In our hospital, we have been using handmade extracorporeal loops in quite a large patient group for a long time.
In the last few years, Hem-o-lok has been used by some surgeons in our clinic due to reasons such as the easy learning curve and shortening the operation time. Hem-o-lok clips, which are polymer clips, are made of nonabsorbable material and their safety in the ligation of structures such as vascular structures, cystic canal, and ureter has been clearly demonstrated in many laparoscopic surgeries.16,17 Endoclips are easily applied laparoscopically and have been reported to reduce both operation time and equipment cost, increasing the efficiency of the procedure. 18 Recently, some studies have compared the polymeric clip with staple and endoloop and reported that the polymeric clip is safe, easy to use, and more cost-effective.19,20 However, we could not find many studies in the English literature comparing the polymer clips with handmade loops. In their retrospective study, Arer et al. compared these two methods and reported that there was no difference in terms of surgical outcomes, operative times, and complications, but when it comes to cost-effectiveness, the cost of Hem-o-lok clips was 31.7 times that of suture material per case. 21 Nevertheless, the potential for stump closure may differ depending on the anatomy of the appendix. In cases where the appendix is inflamed and has a diameter of more than 10 mm, it may not be sufficiently safe. Delibegovic et al. 22 noted cases in which the bulging and edematous appendix base was too large in size during the operation and even the XL clip was not suitable for inclusion in the Hem-o-lok sample because it could not safely surround the base. Rickert et al. 23 reported that they did not perform stump closure with endoclip when the base of the appendix exceeded the size of the endoclip or when the inflammation spread to the cecum due to safety concerns and applied alternative methods of stump closure. In the present study, a handmade loop was used in three cases where the appendix size was larger than 10 mm, and no complications developed. In addition, apart from these two methods, endostapler and endoloop were used for stump closure in 8 patients. The appendix of these patients was also large, edematous, and inflamed.
In this study, we compared the Hem-o-lok clip application, which we applied as a new technique in stump closure in our hospital, with the handmade loop. It was noteworthy that there was no significant difference between the two methods in terms of operation results. The fact that the developed complications were not related to the technique used to fix the appendix base and that there was no significant difference between the 2 patient groups for rehospitalization need confirmed the safety of both methods used in our study. In contrast to the previous study, 21 the duration of the operation was longer in the handmade loop group. We attributed this to the fact that the learning curve of the method is higher and that this method is preferred in edematous and inflamed cases. We are of the opinion that this time would be shorter as the experience of loop creation with sutures increases. In addition, it is known that the shorter surgery time reduces the cost. It was reported that surgical costs are between $30 and 100 per minute. 24 However, the data in this regard are insufficient in our country. In the present study, we did not focus on this issue. Nevertheless, we believe that the length of operative time could be ignored in emergency operations.
In our study, we found that the loop technique was more preferred in perforated appendicitis. In terms of cost efficiency, the handmade loop was found to be significantly better compared to the Hem-o-lok clip in our country. In the current study, the handmade loop achieved excellent results as a safe and low-cost method, and the use of endoloop, which is costlier, has been largely abandoned. The cost-effectiveness of our study is comparable to other studies.
The present study showed that Hem-o-lok clip is safe, very simple to apply, easy to learn, and does not require advanced laparoscopic skills. However, it is about 25 times costlier than the other method. In addition, in developing countries, it may not always be possible to find it in peripheral hospitals located in rural areas. For this reason, we think that it is useful for surgical assistants to gain experience in handmade loops and to graduate with experience with this method.
The retrospective design of our study has the inherent limitation of the design. Some patients may have been missed due to the coding error. In addition, the study utilized a single center data, which needs to be confirmed with multicentric prospective randomized controlled trials. Second, cost analysis was performed for Turkey’s health care system and cannot be generalized because the pricing of services and materials differs in international health systems. However, the method of securing the appendiceal stump is the most important step during LA, and there is still no uniform approach worldwide. We think that our study contributes to the literature which has only limited number of studies comparing these two methods.
Conclusions
Closure of the appendiceal stump using a handmade loop or polymer Hem-o-lok clip during LA is effective and safe with no significant difference in surgical outcomes or complication rate. Unlike the Hem-o-lok clip, the handmade loop requires more skill and can also take a longer time to apply to the base of the appendix. However, it is superior due to its cost efficiency. The only advantage compared to the handmade loop was shorter operative time. In addition, we consider it a good alternative as a cost-effective method in countries where the use of more expensive materials is a concern in cases for whom Hem-o-lok clips cannot be used.
Footnotes
Authors’ Contributions
M.Y. and M.F.T. planned the study; M.Y., A.I.S., and B.K. collected the data; and M.Y., B.K., and N.O. prepared the article and made revisions in the article.
Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
This research received no grant from any funding agency in the public, commercial, or not-for-profit organizations.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.