
Abstract
Background:
The Veterans affairs (VA) surgical quality improvement program was established to evaluate the quality of VA surgical care to over nine million United States Veterans. Patient demographics vary by region, with urban areas correlating with higher mortality rates. This study attempts to determine the factors associated with 30-day mortality at a single VA medical center in an urban setting.
Methods:
Patients included in the study were at least 18 years of age and underwent a surgical procedure between January 2013 and June 2023. Baseline demographics included preoperative comorbidities, American Society of Anesthesiology (ASA) class, and preoperative lab values. Clinical outcomes included postoperative mortality within 30 days of the procedure. Chi-square, t-test, ANOVA, and multivariate logistic regressions were used to determine relationships, using P < .05 to determine significance.
Results:
A total of 11,547 patients with complete data were included, of which 92 patients (0.8%) died within 30 days of surgery. A higher preoperative hematocrit was protective against 30-day mortality. A perioperative transfusion, bleeding disorder, chronic obstructive pulmonary disease (COPD), history of a myocardial infarction, higher ASA class, and an emergency procedure all increased the likelihood of perioperative mortality.
Conclusions:
Veterans who seek surgical care at Veterans Health Administration centers receive high quality care with a low mortality rate. Identifying risk factors for perioperative mortality provides the opportunity to stratify those veterans at highest risk.
Introduction
The Veterans Health Administration (VHA) is the nation’s largest integrated health care system and provides medical care to more than nine million veterans. 1 In 1991, the Veterans Affairs (VA) Surgical Quality Improvement Program (VASQIP) was established to evaluate the quality of VA surgical care. 2 Over the past 3 decades, the VASQIP database has provided a foundation for substantial improvements in the quality and safety of VA surgical care. Subsequently, the standards established by VASQIP for surgical quality improvement were utilized to formulate the American College of Surgeons National Surgical Quality Improvement Program. 3 Since initiating VASQIP, the 30-day mortality of major surgery in the VA decreased from 3.1% in 1991 to 2.3% in 2000. Presently, the 30-day mortality rate for major surgery in the VA system is 1.0%. Compared with the private sector, VA surgical care is associated with a lower risk of perioperative death. 4
Although the VA system shows a lower 30-day mortality rate over the past 3 decades, each respective VA medical center (VAMC) may exhibit varying levels of mortality based on acuity and case complexity. Typically, the demographics and comorbidities of VAMC located in urban regions correlate with higher mortality rates. 5 It is incumbent on each facility to determine their respective mortality rate and the factors associated with that rate. These perioperative factors may delineate a path to decrease mortality in the future. This study attempts to determine the factors associated with 30-day mortality at a single VAMC in an urban setting.
Methods
The investigational review board at the Washington, D.C. VAMC approved this study (#1621468-5). The requisite for informed consent was waived due to the retrospective nature of this study. This research was a retrospective review of the prospectively maintained VASQIP database at an urban medical center located in VISN 5. VASQIP utilizes unique identifying information to track patients who undergo surgical procedures within the VHA system.
Patients included in the study were at least 18 years of age and underwent a surgical procedure between January 2013 and June 2023. Patients were excluded if they had missing information, incomplete data, or underwent a cardiothoracic procedure. Patients who underwent both emergent and elective procedures were included in the study.
Baseline demographics included age, gender, race, preoperative body mass index (BMI), surgical specialty of procedure, tobacco, and alcohol use, as well as preoperative comorbidities, and American Society of Anesthesiology (ASA) class. Lab values, including preoperative creatinine, white blood cell (WBC) count, platelet count, and hematocrit were included. Perioperative transfusion requirement was collected and defined as a patient receiving at least one unit of packed red blood cells during or within 72 hours of the operation. Race and ethnicity were acquired by self-reporting, proxy reporting, or during registration. Patients could select between the following categories: American Indian or Alaska Native, Asian, Black, or African American, Native Hawaiian or Other Pacific Islander, White, or Unknown. For the purpose of analyses, these demographics were consolidated to: Black, White, Hispanic, and Unknown/”Other.”
Clinical outcome included postoperative mortality within 30 days of the procedure. Univariate and multivariate regressions were performed, and continuous data were analyzed with a Student’s t- test, denoting mean ± standard deviations. Categorical variables were reported as frequencies and percentages. The chi-squared or Fisher’s exact test were used to perform univariate comparisons. Binary logistic regression estimated the probability that a certain predisposing factor was predictive of peri-/postoperative mortality. Odds ratios (OR) and adjusted OR (AOR) were calculated using multivariate binary logistic regression and depicted 95% confidence intervals (CI) for comparison of independent variables in patients with and without 30-day mortality after surgery. To provide appropriately adjusted models, all preoperative variables were included in the multivariate comparisons. Both adjusted and unadjusted values were included. SAS Version 9.4 (Cary, NC) was used for all data analyses with P ≤ .05 used to determine significance.
Results
A total of 11,547 patients with complete data were included in this study. The demographics are summarized in Table 1. Of the included patients, 92 patients (0.8%) died within 30 days of surgery. Patients who died were male, older, and had a lower BMI (P < .05). These patients were also more likely to undergo either a vascular (40.2% versus 15.5%; p < .01) or general surgery (31.6% versus 26.5%; P < .001) procedure. Patients who died were more likely to have preoperative risk factors including a higher creatinine and WBC count and a lower baseline hematocrit (P < .05). Baseline platelet count (P = .108) and history of transient ischemic attacks (P = .113) were the only findings not significantly different between the two groups. These findings are summarized in Table 2 and Figure 1. Patients who died within 30 days of their procedure were more likely to have pneumonia and all non-infectious complications (P < .001) except for deep vein thrombosis (P = .286; Table 3).
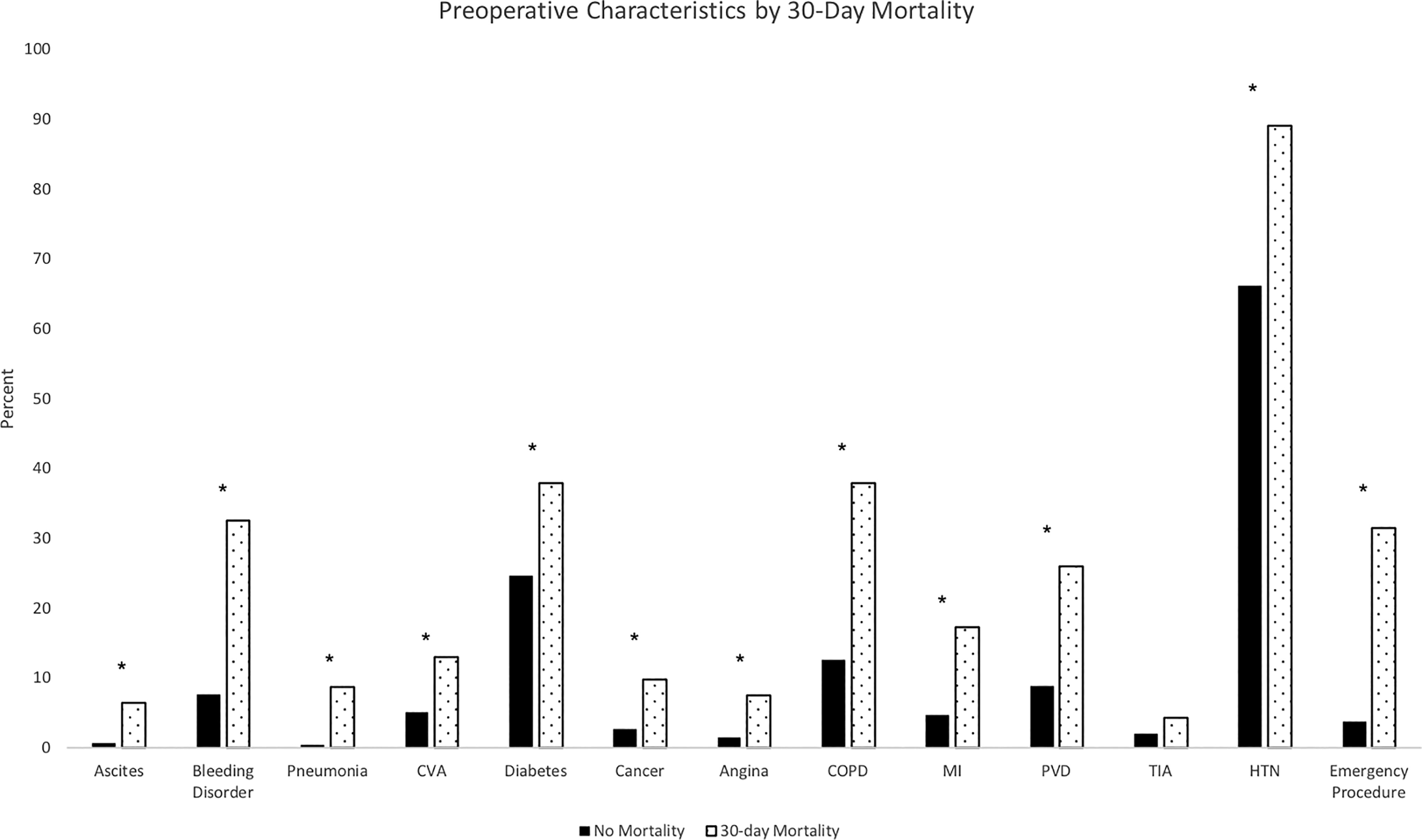
CVA, cerebral vascular accident; COPD, chronic obstructive pulmonary disease; MI, myocardial infarction history; PVD, peripheral vascular disease; TIA, transient ischemic attack; HTN, hypertension.* indicates significant difference at P < .05.
Demographics Stratified by 30-Day Mortality
t-test.
BMI, body mass index; ENT, ear nose throat; SD, standard deviation.
Preoperative Characteristics Dichotomized by 30-Day Mortality
t-test.
Chi-Square.
ASA, American Society of Anesthesiology; COPD, chronic obstructive pulmonary disease; CVA, cerebral vascular accident; HTN, hypertension; MI, myocardial infarction history; PVD, peripheral vascular disease; SD, standard deviation; TIA, transient ischemic attack.
Postoperative Outcomes Stratified by 30-Day Mortality
Chi-Square.
CVA, cerebral vascular accident; DVT, deep vein thrombosis; MI, myocardial infarction; PE, pulmonary embolism; SSI, surgical site infection; UTI, urinary tract infection.
Multivariate regression analyses (Table 4) showed that a higher preoperative hematocrit (AOR = 1.0 [95% CI:.9–1.0]) was protective against 30-day mortality. A perioperative transfusion (AOR = 2.6 [95%CI: 1.4–4.6]), bleeding disorder (AOR = 1.9 [95% CI: 1.1–3.1]), COPD (AOR = 2.0 [95% CI: 1.2–3.2]), history of a myocardial infarction (AOR = 1.9 [95% CI: 1.1–3.6]), higher ASA class (AOR = 1.7 [95% CI: 1.1–2.7]), and an emergency procedure (AOR = 3.0 [95% CI: 1.7–5.3]) significantly raised the likelihood of 30-day mortality by approximately two-fold or more. Age and elevated WBC count increased the risk of 30-day mortality, though the adjusted finding was negligible (P < .05).
Univariate and Multivariate Regression Model for 30-Day Mortality
Multivariate regression controlled for: preoperative creatinine, platelet count, body mass index, sex, race (ethnicity, alcohol use, tobacco use, ascites, pneumonia, cerebral vascular accident history, diabetes, cancer, history of angina, peripheral vascular disease, transient ischemic attack, hypertension, and surgical specialty.
ASA, American Society of Anesthesiology; COPD, chronic obstructive pulmonary disorder; Hct, hematocrit; MI, myocardial infarction; aOR, adjusted odds ratio; OR, odds ratio; WBC, white blood cell count.
Discussion
The literature documents that VHA provides high quality care in surgery along with primary care, preventative services, and mental health.4,6 While much of the quality research focuses on comparisons between VHA and the private sector, this article identifies the characteristics that contribute to mortality after surgery at a single VHA facility. Within the context of non-cardiac surgical care, the overall incidence of mortality is low. Within this low incidence, the opportunity exists to effect significant improvement in mortality with small changes. In fact, that effort is evident by the decreasing mortality rate at VHA facilities since the advent of VASQIP 3 decades ago. Other studies illustrate that the mortality rate using VASQIP is around 1.0%, which is consistent with the findings in this study.7,8 This study corroborates previous literature that documented that pulmonary complications and sepsis contribute to an increased risk of mortality after surgery. 9 While low preoperative albumin is associated with mortality, no other recent studies report these perioperative components and the relationship with mortality. 10
By recognizing the perioperative factors associated with mortality, surgeons may identify those veterans at risk for mortality and provide prophylactic care to mitigate these risk factors. Some of the factors are not modifiable, such as age, presence of bleeding disorder or an emergent procedure. Yet, this data may be used to counsel patients and their families when these various characteristics are present preoperatively. This data also presents modifiable risk factors that contribute to mortality including anemia, coronary artery disease and COPD. Optimizing these comorbid conditions in the perioperative period may yield a reduction in mortality. Single institution program changes illustrate the capacity to reduce postoperative complications. Specifically, the literature reports that a preoperative clinical conference for Veterans deemed high risk reduces mortality. In addition, multiple studies verify that preoperative pulmonary physiotherapy reduces postoperative complications. 6 , 7 , 11 , 12
The methods of this research are not without limitations. This study used only one VHA center to identify risk factors for mortality. The medical center serves an urban population and the results may not be generalized to all VHA facilities. In addition, as is common within VA Health facilities, most patients included in this study are male. In the future, the percentage of females who undergo surgeries at VA facilities will increase. Future research may focus on sex-based differences in surgical outcomes at VHA centers.
Veterans that seek care at VA hospitals face unique medical, social, and economic challenges that influence their outcomes. 13 VHA continues to implement programmatic changes to reduce mortality rates. This paper identifies those risk factors that contribute to a higher rate of mortality at a single VA medical center. In the future, research should continue to analyze the VASQIP database to determine if programmatic modifications impact mortality.
Conclusion
Veterans who seek surgical care at VHA centers receive high quality care with a low mortality rate. Identifying risk factors for perioperative mortality provides the opportunity to stratify those veterans at highest risk.
Footnotes
Authors’ Contributions
J.A.R.: Conceptualization, methodology, software, formal analysis, writing. S.O.D.: conceptualization, writing, validation. F.B.: Data curation, writing, supervision, project administration
Disclosure Statement
J. Alex Randall, Fred Brody, and Samuel Dennis have no funding/conflicts to disclose. The views expressed in this submission are those of the authors and not an official position of the institution or agency.
Funding Information
No funding was received for this article.