
Abstract
Objective:
The aim of our study was to assess the learning curve of robotic assisted low anterior resection with diverting loop ileostomy (LARDLI) for low and mid rectal cancer performed by novice in robotic-assisted surgery colorectal surgeon in a public hospital with limited access to the robotic platform.
Methods:
A retrospective analysis of all low and mid rectal cancer robotic-assisted operations was conducted. All procedures were performed by a single surgeon with a once per week access to the Da Vinci® Si™ Surgical System, Intuitive Surgical Inc. Demographic, clinical, and pathological data were reviewed. The cumulative sum (CUSUM) analysis was utilized to analyze learning curve for operative time.
Results:
A total of 107 consecutive patients who underwent LARDLI for lower and mid rectal cancer between November 2011 and July 2020 were included in the analysis. The median patients’ age was 65 (range, 32–85) years, 72% were males (n = 77), and 91% (n = 97) received neoadjuvant therapy. Median operative time was 295.5 (range, 180–551) minutes. The conversion rate was 3.7% (n = 4). Median length of hospital stay was 6 (range, 1–41) days. There were 35 (32.7%) postoperative complications, of these 7 (6.5%) were major complications (≥Grade 3, according to the Clavien–Dindo classification). There was only one intraoperative complication (.9%). CUSUM analysis showed that the learning curve was 49 cases to achieve a plateau.
Conclusions:
The learning curve of robotic assisted low anterior resection for lower and mid rectal cancer for a novice in robotic surgery colorectal surgeon with limited access to the robotic platform is 49 cases. Surgeon and operative team dedication, alongside sufficient hospital support, may lower the number of cases of the learning curve.
Introduction
Colorectal cancer (CRC) is the third most common neoplastic disorder in both men and women worldwide. Approximately 150,000 patients are diagnosed with CRC annually. Of these, approximately one-third of patients are diagnosed with rectal cancer. 1
Rectal cancer treatment has undergone significant changes over the past few decades. 2 First, the introduction of total mesorectal excision (TME) following the anatomical “Holy Plane” described by Heald et al., 3 significantly contributed to the standardization of rectal cancer surgery worldwide, increasing patients’ overall survival. Second, the introduction of preoperative neoadjuvant therapy, including preoperative radiation along with preoperative chemotherapy, reduces the rates of local and distant recurrence. 4 Furthermore, preoperative neoadjuvant therapy results in a complete clinical response of the tumor in about 15%–25% of patients, opening the possibility of a rectal sparing treatment strategy and follow-up. 5
Another significant change in rectal cancer management is the operating approach and platform. Minimally invasive surgery has evolved significantly over the past 3 decades, and new robotic platforms have been introduced into practice. In rectal cancer surgery, robot-assisted surgery has become the standard of care, especially for low- and mid-rectal tumors.6,7 The advantages of the robot, which include improved visualization and dexterity, are particularly notable in small spaces, making it an ideal platform for pelvic surgery. Recent studies have demonstrated that the advantages of robotic platforms contribute to improved surgical outcomes, including lower rates of short- and long-term sequelae, along with improved overall survival.8,9
Despite these inherent advantages of the robotic platform, adoption of robotic surgery has been relatively slow, mainly due to increased costs and the need for additional training and education by surgeons. 10 Previous studies demonstrated that robotic surgery for rectal cancer requires a steep learning curve as it involves mastering new technical skills, overcoming the challenges posed by the limited pelvic space, and the complex anatomy and surgical techniques involved.11,12
Understanding the learning curve of robotic surgery in rectal cancer is essential for optimizing patient outcomes and ensuring patient safety. In this study, we aimed to evaluate the learning curve for robotic rectal cancer surgery in a public tertiary single center, in which a single laparoscopic trained colorectal surgeon had weekly access to the Da Vinci® Si™ Surgical System, Intuitive Surgical Inc. in order to guide surgeons who wish to adopt the robotic platform for these complex surgical cases.
Methods
We conducted a retrospective analysis using a prospectively maintained database to investigate the learning curve for robotic resections of low and mid rectal cancers performed at a single tertiary center between November 2011 and July 2020. The study included cases performed after the introduction of Da Vinci® Si™ Surgical System, Intuitive Surgical Inc., when an experienced colorectal surgeon (M.K.) started adoption of the robotic platform. These robotic cases were performed consecutively and were part of the general learning curve in robotic colorectal surgery. We collected various variables of interest, including age, gender, body mass index, American Society of Anesthesiologists (ASA) grade, height of tumor location (low, middle, or upper rectum), and American Joint Committee on Cancer (AJCC) tumor stage. These variables were recorded in a structured database. The outcome variables examined were operation time (minutes), conversion rate, lymph node harvest, length of hospital stay (days), reoperation rate, major complications (Clavien–Dindo Grade 3a–4b), and 30-day mortality. The size of the study was determined by the number of consecutive robotic cases performed by the surgeon. Operative time was defined as the duration from the skin incision to the final stitch, including docking time. The study protocol received approval from the local institutional review board (IRB #: 2801-20-SMC).
Operative procedure
Before the adoption of robotic-assisted low anterior resection (LAR), the primary technique used for rectal cancer surgeries was laparoscopic surgery. On days when the robotic platform was not available, laparoscopic LAR was performed. Although detailed operative times for laparoscopic procedures were not recorded systematically, the transition phase involved comparing outcomes and adapting to the new robotic technology. The surgeon performing these procedures had extensive experience in laparoscopic colorectal surgery before transitioning to robotic-assisted techniques. A standardized approach was followed for performing robotic-assisted proctectomies with total mesorectal excisions. A single docking method was employed during the surgical procedure including robotic-assisted pelvic drain insertion and an ileostomy preparing. The robotic operation was mostly assisted by surgical residents (junior and senior) and some of the cases by board-certified general surgeons. It is noteworthy that the assistants had no prior experience in robotic-assisted surgery.
Cumulative sum analysis
To monitor the surgeon’s performance, particularly in terms of operative time, cumulative sum (CUSUM) curves were utilized. 13 The X-axis of the graph represents the consecutive case number, while the Y-axis represents the CUSUM score. The CUSUM curves ascend when the predefined targets are not met, indicating an ongoing learning process. When the performance remains consistent from case to case, the curve plateaus (running more or less parallel to the X-axis), indicating no further learning. Conversely, a downward trend in the curve suggests improvement in performance, with more successful outcomes achieved than initially anticipated.
Statistical methods
Categorical variables were compared using either a chi-square or Fisher’s exact test, as appropriate. Continuous variables were compared using the Mann–Whitney U test. The statistical analyses were conducted using R Software (version 3.6.2, R Core Team, Vienna, Austria).
Results
In this study, we analyzed data of 107 patients who underwent robotic-assisted surgery for low- and mid-rectal cancer during the study period. The cohort was predominantly male (72%) with an average age of 63 years (SD 11). The majority of patients in this study were classified as ASA 2 (45.8%) and ASA 3 (51.4%). A total of 70.1% of patients were diagnosed with locally advanced disease (stage II-III). Ninety-seven patients (90.7%) received neoadjuvant treatment and 64.5% received adjuvant treatment following surgery. Patients’ demographic and clinical data is summarized in Table 1.
Patients Demographic and Clinical Data
ASA, American Society of Anesthesiologists; LN, Lymph node; LAR, Low anterior resection; ISR, Intersphincteric resection; APR, Abdominoperineal resection.
The conversion rate was 3.7%. The median duration of hospital postoperative stay was 6 (range, 1–41) days, and patients were followed up for a median duration of 770 days. Approximately one-third of the patients (32.7%) experienced complications following the surgery. Of these 7 (6.5%) were major complications (≥Grade 3, according to the Clavien–Dindo classification). There was only one intraoperative complication (.9%). The mortality rate at 30 days post-surgery was 1.9%.
Median operative time was 295.5 (range, 180–551) minutes. The analysis of the learning curve revealed three distinct phases: phase 1 (initial 16 cases), phase 2 (second 16 cases), and phase 3 (subsequent 25 cases). The longest operation time was observed in phase 2. CUSUM analysis showed that the learning curve was 49 cases to achieve a plateau (Fig. 1). In addition, the CUSUM analysis indicated that consistent operative times were achieved after approximately 65 cases.
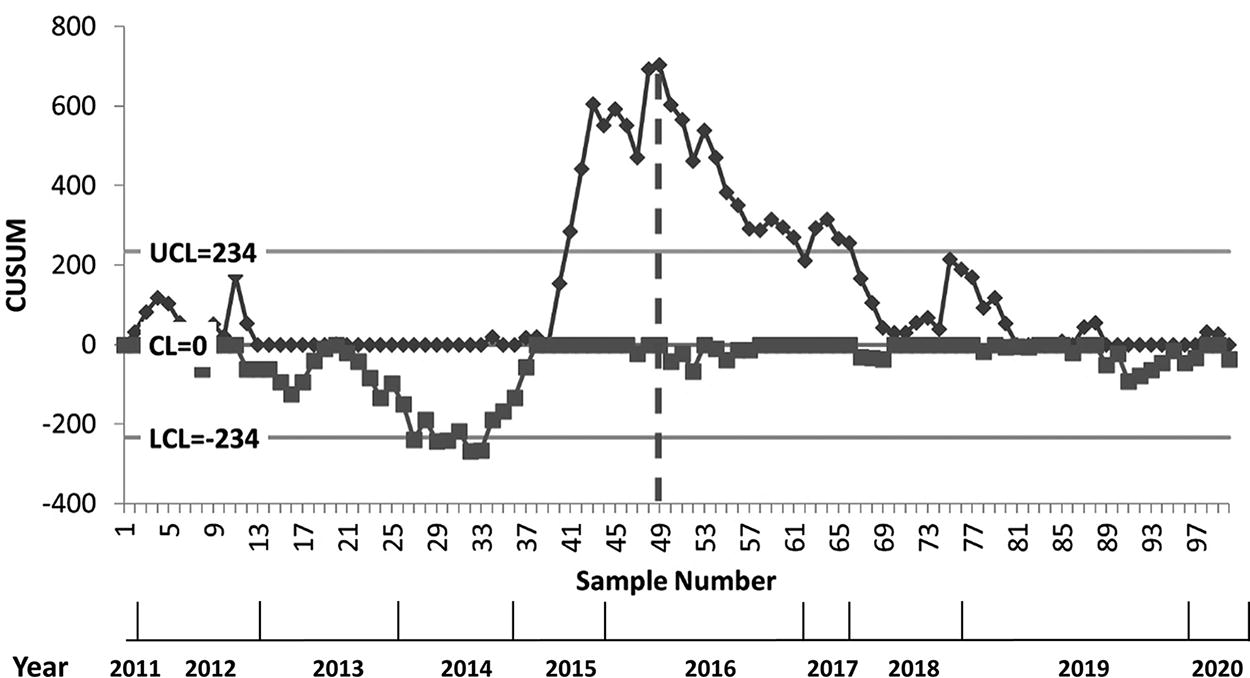
Cumulative sum (CUSUM) analysis for operative time of robotic assisted low anterior resection with diverting loop ileostomy for low and mid rectal cancer.
Discussion
Robotic-assisted surgery has gained significant attention in the field of rectal cancer treatment, offering advantages such as improved visualization, dexterity, and surgical outcomes. 14 In our study, we aimed to evaluate the learning curve of robotic-assisted surgery in rectal cancer and optimize patient outcomes. Our findings provide valuable insights into the adoption of this technique and its impact on surgical proficiency.
Our analysis revealed a distinct learning curve consisting of three phases: phase 1 (initial 16 cases), phase 2 (next 16 cases), and phase 3 (subsequent 25 cases). Using CUSUM analysis, we observed that the learning curve reached stabilization after 49 cases, indicating the attainment of surgical proficiency. While the CUSUM analysis indicated a learning curve plateau at 49 cases, a statistical process control chart approach suggested that consistent operative times were achieved after approximately 65 cases. This discrepancy underscores the complexity and variability in mastering robotic-assisted surgery. The extended learning phase reflects the surgeon’s exposure to a broader range of cases with varying complexities, highlighting the importance of continuous performance monitoring and adjustment of surgical techniques to achieve proficiency.
Comparing our findings with other publications, we observed similarities in terms of the number of cases required to achieve proficiency. Several studies have reported learning curves ranging from 40 to 60 cases for robotic rectal surgery. While the exact number may vary depending on factors such as surgeon experience and institutional settings, our study aligns with the existing literature in demonstrating the need for a sufficient case volume to optimize surgical outcomes.15–17
It is important to note that the learning curve and outcomes can be influenced by various factors, including the availability of the robotic platform.18,19 In many public hospitals, the robot is shared among different surgical disciplines, limiting its accessibility for colorectal surgeons. 14 This factor can affect the learning curve, potentially requiring a longer duration to achieve proficiency. To address this limitation, hospitals can consider implementing strategies to enhance access to the robot, such as dedicated time slots for colorectal procedures and interdisciplinary collaborations.20,21
The learning curve observed in this study suggests that a 1-year fellowship may not be sufficient for trainees to achieve proficiency in robotic-assisted rectal surgery. This necessitates a reconsideration of training paradigms, potentially focusing on a single surgical approach to maximize case volume and skill acquisition. Post-fellowship mentoring and continued practice are essential for completing the learning curve and ensuring optimal patient outcomes. Additionally, the training program should integrate other robotic colorectal procedures to familiarize trainees with the ergonomics and technical aspects of the robotic platform, thereby accelerating their learning process.
Despite the insights provided by our study, there are some limitations to consider. Our study was conducted in a single center, which may limit the generalizability of our findings. Another limitation is the lack of detailed operative time data for the laparoscopic procedures performed before the adoption of the robotic platform. This limits the ability to directly compare the efficiency of the two techniques. Additionally, the quality of TME was not systematically measured throughout the study period, nor was there sufficient follow-up to report on local recurrence rates. Lastly, our analysis focused on surgical outcomes and did not comprehensively assess other factors such as patient-reported outcomes and cost-effectiveness. Future studies could explore these aspects to provide a more comprehensive understanding of the learning curve of robotic surgery in rectal cancer.
In conclusion, our study contributes to the growing body of knowledge on the learning curve of robotic-assisted surgery in rectal cancer. The findings highlight the importance of a sufficient case volume and optimized access to the robotic system for surgeons to achieve proficiency. By addressing the limitations and implementing strategies to enhance access and training, hospitals can maximize the benefits of robotic surgery and improve patient outcomes in rectal cancer treatment.
Footnotes
Authors’ Contributions
N.H.: Conceptualization, methodology, writing—original draft, writing—review and editing. R.A.: Data curation, investigation, formal analysis. M.S.: Visualization, software, writing—review and editing. Y.Z.: Supervision, validation, project administration. M.K.: Resources, funding acquisition, writing—review and editing.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.