
Abstract
Background:
Laparoscopic sleeve gastrectomy (LSG) is an effective surgical intervention for obesity, but managing complications post LSG remains crucial. Given the global prevalence of obesity, innovative approaches are needed to improve patient outcomes.
Objective:
This scoping review aimed to comprehensively map the existing literature on innovative approaches for managing complications in adult patients undergoing LSG to treat morbid obesity. This management strategy may include surgical techniques, perioperative care, nutritional support, or other relevant strategies.
Methods:
A systematic search of PubMed and Scopus databases was conducted to identify relevant studies. The prespecified inclusion criteria were applied through a two-stage screening process. Studies involving adult patients who underwent LSG for morbid obesity (body mass index > 35) and those investigating interventions related to complications were included. The scoping review process adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews. The results were summarized using a narrative approach.
Results:
This review included 31 studies with 4547 participants, showing diverse study designs, patient demographics, and surgical locations. Among them, 6 were case reports, 18 were randomized controlled trials, and 7 were retrospective studies. Complications of LSG include staple-line leaks, stenosis, hemorrhage, infection, gastric volvulus, and nutrient malabsorption. Innovative interventions, such as staple-line reinforcement, plication methods, and the Over-the-Scope Clip system, have been investigated for effective management.
Conclusion:
This scoping review provides valuable insights into innovative interventions for managing complications post LSG. This review highlights the need for further research to explore long-term outcomes, compare different interventions, and address the existing gaps in the literature.
Introduction
Obesity is a multifaceted and pervasive health issue that has become a global epidemic that transcends geographical and cultural boundaries.1–3 Characterized by the excess accumulation of body fat, obesity is a complex condition with far-reaching implications for both individual health and public well-being.4–7 Lifestyle factors, including sedentary behavior, unhealthy dietary patterns, and a confluence of genetic and environmental influences, contribute to the onset and progression of obesity.5,7–10 The escalating global prevalence of obesity has prompted the development of surgical interventions to counteract its profound health implications. The history of surgical interventions for obesity dates back to the mid-20th century, marked by pioneering procedures such as jejunoileal and gastric bypass.7,11–13 While showcasing the potential for significant weight loss, these early attempts were marred by complications and side effects, prompting the medical community to seek safer and more effective alternatives.13,14
In the late 20th century, the advent of laparoscopic surgery revolutionized the field of bariatrics. Laparoscopic procedures offer reduced invasiveness, shorter recovery times, and fewer postoperative complications compared with traditional open surgery. Among these interventions, laparoscopic sleeve gastrectomy (LSG) has emerged as the forefront procedure, demonstrating effectiveness for substantial and sustained weight loss.14–17 Originally introduced as the first stage of the more extensive duodenal switch procedure, LSG underwent a transformative journey, eventually evolving into a stand-alone procedure owing to its efficacy and relative simplicity. Its popularity surged as studies demonstrated not only significant weight loss but also improvements in comorbidities such as type 2 diabetes and hypertension.18,19 However, as the utilization of LSG expands, the need to optimize postoperative outcomes and manage associated metabolic stress and complications becomes increasingly evident.
Perioperative care plays a pivotal role in ensuring the success of LSG, with tailored strategies designed to address the unique needs of each patient.20,21 Preoperative optimization, meticulous intraoperative management, and vigilant postoperative monitoring contribute to a holistic approach that maximizes the benefits of surgical intervention while minimizing potential risks.22–24
Nutritional support is recognized as a cornerstone in the postoperative care of LSG recipients, with personalized dietary plans tailored to meet individual needs and optimize weight loss.25–27 Nutritional counseling and ongoing monitoring help patients navigate the challenges of dietary changes post-surgery, ensuring adequate nutrient intake and supporting long-term success.28,29
Postoperative complications, including leaks and strictures, present challenges in the postoperative trajectory of LSG recipients.30,31 Traditional interventions have shown efficacy, but the dynamic landscape of innovation reshapes the approach to managing these challenges. 32 Strategies, including surgical techniques, perioperative care, pharmacological interventions, and nutritional support, are being explored to enhance the overall effectiveness of LSG and improve patient outcomes.
This scoping review sought to systematically synthesize the existing literature on complications and innovative approaches to their management in patients with LSG. By comprehensively exploring the available evidence, this review aims to identify key themes, patterns, and gaps in the literature. The goal was to provide valuable insights into evidence-based clinical practices, guide future research directions, and foster advancements in the dynamic field of bariatric surgery.
Search Methodology
While preparing this scoping review, we followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews. A comprehensive search strategy was implemented to identify relevant studies on LSG and its association with potential complications. This strategy employed a combination of Medical Subject Headings (MeSH) terms and keywords in two primary databases: PubMed and Scopus. In PubMed, MeSH terms were utilized for search term mapping, including Laparoscopic Sleeve Gastrectomy, insulin resistance, postoperative complications, and surgical techniques. Boolean operator (AND) was employed to combine MeSH terms and keywords, ensuring that the retrieved articles addressed both LSG and designated outcome domains (metabolic stress/complications).
In Scopus, search terms were restricted to the abstract, keywords, and title fields to optimize retrieval accuracy while considering a database-specific search algorithm. Considering potential algorithm variations, the search strategy was further refined by applying filters for source type (e.g., peer-reviewed journals), language (e.g., English), and publication stage (e.g., published articles). During the search, unpublished or gray literature, such as conference abstracts, was excluded to maintain the quality of the published research. Fifteen searches were conducted. The retrieved citations were then merged and de-duplicated using a reference management software to generate a comprehensive list of potential studies for further evaluation. This refined search methodology aimed to capture a robust and relevant dataset for analyzing the relationship between LSG and possible complications.
Eligibility criteria
Given the orientation of systematic reviews in evidence-based health care, various frameworks have been established to comprehensively evaluate existing literature. In this study, we adopted the PICOS (Population, Intervention, Comparison, Outcomes, and Study Design) framework. This framework serves as an extension of the traditional PICO model by incorporating the qualitative aspects often encountered in small-sample systematic reviews. The PICOS framework guided the development of inclusion and exclusion criteria, as detailed below.
Inclusion criteria
Population
Adult patients (≥18 years old) diagnosed with obesity (body mass index ≥35) who underwent LSG.
Intervention
Studies investigating interventions for managing complications following LSG. It includes surgical techniques, perioperative care strategies, pharmacological interventions, nutritional support plans, and other relevant management strategies.
Comparators
Studies may include or exclude comparison groups. Studies comparing different management strategies for complications after LSG should be conducted.
Outcomes
Studies reporting the primary or secondary outcome related to complications after LSG. These include but are not limited to insulin resistance, weight loss, nutrient malabsorption, and postoperative complications (leaks, strictures, etc.).
Study design
To ensure robust evidence, only the studies with the following designs were included: randomized controlled trials (RCTs), cohort studies, case–control studies, and observational studies.
Exclusion criteria
Population
Studies involving (1) pediatric patients under 18 years of age, (2) patients with specific comorbidities not directly related to obesity (e.g., malignancies or severe cardiac diseases), and (3) patients undergoing gastrectomy for conditions other than morbid obesity.
Intervention
Studies that (1) did not investigate LSG and (2) did not address strategies for managing complications after LSG.
Comparators
Studies that (1) lacked relevant comparators or (2) had insufficient data for comparisons.
Outcomes
Studies that did not report primary or secondary outcomes relevant to complications following LSG (e.g., insulin resistance, weight loss, nutrient malabsorption, and specific complications).
Study design
Animal studies, case reports, reviews, opinion papers, and editorials.
Selection of studies and data extraction
To ensure reliable data collection, a two-step eligibility screening process was implemented, involving two independent evaluations based on the PICOS criteria for inclusion and exclusion. The Rayyan 33 web server was employed to ensure blind evaluation, data extraction, and deduplication. A two-step approach was used to ensure an efficient study design. Initially, all abstracts and titles were scanned for the exclusion criteria. Full-text articles were retrieved from only potentially relevant abstracts. Two reviewers independently reviewed the full-text articles to determine their eligibility based on the criteria mentioned above. Discrepancies during the screening process were resolved through discussion and consensus between reviewers.
After eligibility was established, the Rayyan software was used for independent data extraction. The following parameters (Table 1) were extracted from each eligible study.
Summary of Included Studies on Laparoscopic Sleeve Gastrectomy
BMI, body mass index; CR, case report; RCT, randomized control trial; RetCoh, Retrospective Cohort Study.
Results and Discussion
Search results and initial screening
Our search yielded 822 and 1500 records from PubMed and Scopus, respectively (Fig. 1). Of these 1609 records were imported to the Mendeley reference manager to automatically recognize and remove duplicates. In total, 375 duplicate records were identified and deleted. The remaining 1243 results were screened for eligibility based on the title and abstract. We have removed 1188 results from this phase. The full texts of the remaining 46 studies were obtained for the second stage of screening, based on the full manuscript. Finally, 31 studies met the inclusion criteria and were included in the present review. PRISMA extension for RISMA-S: PRISMA Search Reporting Extension is included as supplementary material. Among them, 6 were case reports, 18 were RCTs, and 7 were retrospective studies (Figs. 1 and 2). Geographically, the studies were conducted in various countries, reflecting the global interest and engagement in investigating LSG outcomes. The study included 4547 patients who underwent LSG.

PRISMA flow diagram for study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
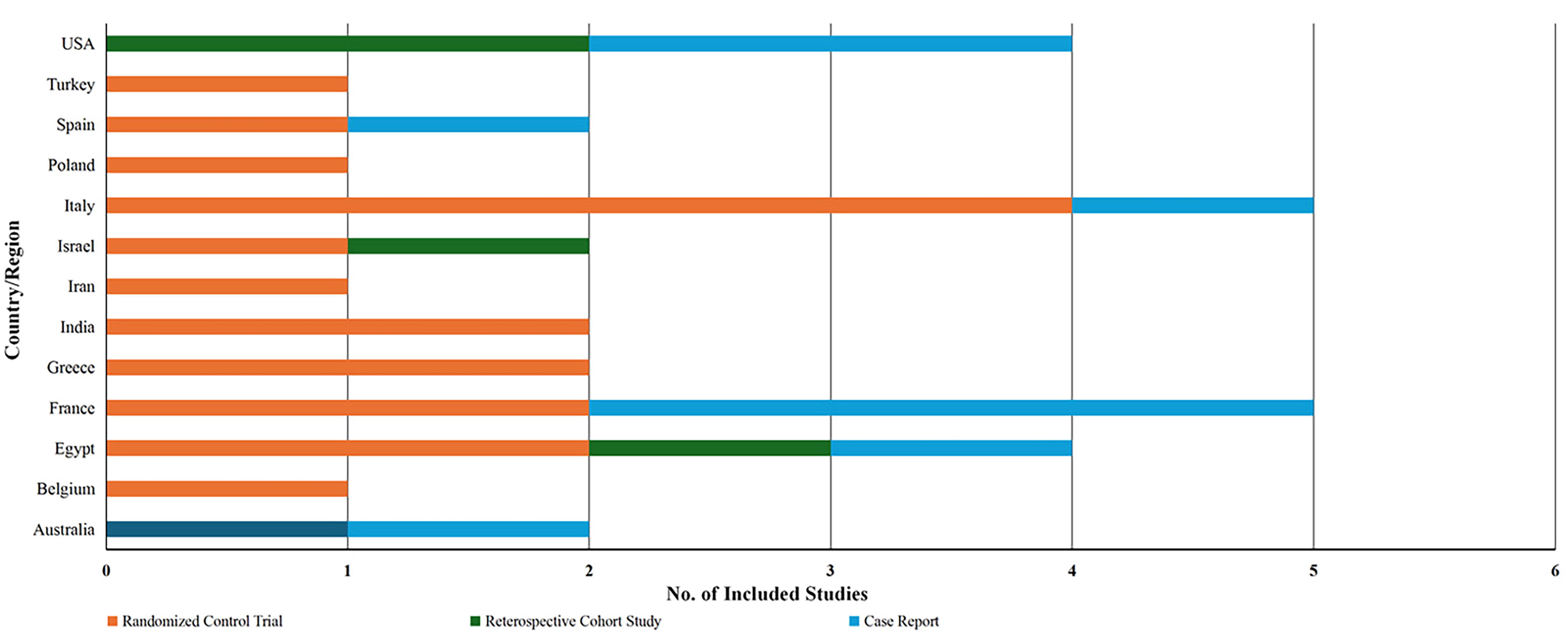
Graphical representation of the distribution of included studies according to regions.
Common complications associated with LSG
The identified complications associated with LSG, including staple-line leaks,39,46,47,51,56,57 symptomatic stenosis (SS), 38 hemorrhage,34,51,60,63 gastric volvulus, 63 and nutrient malabsorption, 53 underscore the multifaceted challenges in postoperative care. Late complications of LSG include staple-line bleeding, stricture, and staple-line leak. 65 These complications align with the existing literature, highlighting the importance of ongoing efforts to enhance the safety and efficacy of LSG procedures. 32
Although uncommon, staple-line leaks after LSG can cause anything from minor problems to death. 34 These leaks are the main cause of secondary complications, including mortality, postoperative hemorrhage/hematoma rate, and prolonged hospital stays. 46
A RCT aimed to assess the prevalence and management of bleeding complications associated with LSG. 52 The study included 165 patients randomly assigned to three arms: stapler line application of biological glue (Evicel™), over-suturing of the stapler line, or control. The results indicated that routine elevation of systolic blood pressure to 140 mmHg, coupled with over-suturing of the staple line, minimized hemorrhagic complications with reasonable prolongation of the procedure. The incidence of bleeding complications was notably lower in the over-suture reinforcement group than in the other groups. This study suggests that active blood pressure control and specific staple-line reinforcement techniques contribute to reducing bleeding complications in LSG, offering insights into effective management strategies for this common bariatric procedure.
The occurrence of a gastric volvulus after sleeve gastrectomy is rare. However, it can present with nonspecific symptoms and signs that require physician vigilance for an accurate diagnosis. In managing complex cases of gastric obstruction resulting from post-SG gastric volvulus, thorough adhesion lysis between the stomach and neighboring structures is advised. Specifically, in situations involving a sleeve gastrectomy and the onset of de novo reflux symptoms following the procedure, conversion to a Roux-en-Y gastric bypass is recommended for effective management. 63
Sleeve gastrectomy is believed to induce nutritional deficiencies. Therefore, the use of multivitamin supplements following various bariatric procedures, including LSG, has been emphasized in the literature. An RCT was conducted to assess the efficacy of this treatment. Patients were divided into two groups: one receiving multivitamin supplements for 3 months postsurgery and the other for 12 months postsurgery. The results indicated that maintaining multivitamin supplements beyond 3 months offered no discernible benefits. At 3 months, both groups showed similar rates of iron deficiency, which were corrected with specific supplements. Additionally, at 6 and 12 months, only isolated cases of deficiencies (iron and vitamin D) were observed, predominantly in the group that received supplements for 12 months. The study concluded that prolonged multivitamin supplementation may not be essential, instead advocating for monitoring laboratory values and administering specific supplements when deficiencies arise, highlighting the importance of individualized management post-LSG. 53
This retrospective study investigated the occurrence, causes, and management of SS after LSG. Among the 230 morbidly obese patients who underwent LSG, 3.5% (all female) developed SS, with endoscopic balloon dilation proving successful in treating short-segment stenoses. Long-segment stenoses unresponsive to endoscopic measures necessitate conversion to Roux-en-Y gastric bypass. Other severe complications, such as staple-line hematoma and leak, which ultimately require surgical revision, have also been reported. Overall, the findings suggest that symptomatic short-segment stenosis after LSG can be effectively managed endoscopically, whereas longer stenoses may require more extensive interventions, such as conversion to Roux-en-Y gastric bypass. 38
Postoperative infections, although uncommon, can be a complication of LSG. Infections may arise at the surgical site or in surrounding areas, necessitating vigilance in postoperative care. Early recognition and appropriate management of infections are crucial to prevent complications and promote optimal recovery. This highlights the importance of a comprehensive approach to postoperative care, including infection prevention strategies, thorough monitoring, and timely intervention, to ensure the safety and well-being of individuals undergoing LSG. 52
Innovative interventions
This scoping review identified several innovative interventions aimed at managing complications in patients who underwent LSG. Innovative interventions, such as staple-line reinforcement techniques, plication methods, and the use of Over-the-Scope Clip (OTSC), have emerged as key strategies to address these complications.
Staple-line reinforcement techniques
Staple-line leaks after LSG, although uncommon, can cause anything from minor problems to death (1%–3% mortality rate), and staple-line reinforcement techniques are key developments in managing these leaks. 34 Hany and Ibrahim 59 conducted an RCT and reported the positive impact of reinforcement of staple lines, albeit with a longer operation time and no significant difference in bleeding. 59
Aiolfi et al. conducted a comprehensive evaluation of the SLR techniques for LSG through a network meta-analysis of 17 RCTs. The study included 3994 patients and compared no reinforcement (NR), suture oversewing (SR), glue reinforcement (GR), bioabsorbable staple-line reinforcement (Gore® Seamguard®) (GoR), and clips reinforcement (CR). SR demonstrated a significantly reduced risk of bleeding, staple-line leak, and overall complications compared with NR, with no significant differences observed against GR, GoR, and CR. However, SR was associated with longer operative time. This study suggests that SR may offer clinical benefits in reducing certain complications, emphasizing the need for further trials to explore the efficacy of less studied techniques, such as GoR and CR. 66 According to Aggarwal et al., 42 buttressing staples using continuous suturing in obese patients leads to a reduction in staple leaks; however, the procedure incurs indirect costs in terms of greater operation time.42,57 Alamdari et al. 58 examined the efficiency of reinforced staple lines in patients (n = 199) undergoing LSG surgery for bleeding and leakage. Gentileschi et al. 39 reported that Staple line reinforcement with either polyglycolide acid with trimethylene carbonate or gelatin fibrin matrix was faster than oversewing. Similarly, Rebibo et al. 60 evaluated the effectiveness of fibrin sealant in preventing the development of staple-line complications after sleeve gastrectomy and identified that the sealant did not prevent the development of staple-line complications. 60
Donatelli et al. 44 evaluated the efficiency of endoscopic internal drainage for treating staple leaks using pigtail stents coupled with enteral nutrition. It was found that 20/21 (95.2%) of the leakage cases were healed using this approach without additional complications. 44 Parikh et al. 38 reported the successful management of short-segment stenoses through endoscopic balloon dilation, highlighting the potential of this technique to address specific post-LSG complications. 38
The effectiveness of SR in reducing the risk of bleeding and leaks, as demonstrated by Aiolfi et al.’s network meta-analysis, 66 suggests a promising avenue for improving the postoperative outcomes of LSG. Similarly, the exploration of plication techniques for managing SS and the application of the OTSC 41 to minimize bleeding complications indicates a dynamic landscape of interventions aimed at optimizing patient care.
OTSC system
Gastric staple-line fistulas following sleeve gastrectomy are infrequent but difficult to manage using traditional sewing methods. 41 Aly and Lim 41 reported two consecutive cases of successful management of sleeve leaks using OTSC devices that provided full-thickness or near-full-thickness circumferential closure of the perforation area. In another study, Gómez et al. 40 reported closure of iatrogenic perforations and bariatric gastric fistulas in a 45-year-old Hispanic woman using a larger OTSC. Closure of small mural defects was achieved using larger, more powerful endoscopic clips for a noninvasive bariatric procedure in obese individuals. 40
Conio et al. 35 identified the OTSC system as an innovative intervention for managing complications such as bleeding. 35 One RCT assessed the prevalence and management of bleeding complications associated with LSG. This study included an arm in which a stapler line was applied to the OTSC system. The results indicated a lower incidence of bleeding complications in this group than in the other reinforcement techniques, suggesting the potential utility of the OTSC system for enhancing the safety of LSG. In a retrospective control study, Mercky et al. 45 reported the postoperative outcomes of using OTSC chips for the treatment of complex gastrointestinal (GI) postoperative leakage and other relevant complications in patients (n = 30). With a healing rate of over 85%, OTSC placement was found to be safe and effective for the treatment of GI fistulas, with better results for GI leaks following LSG. 45
Clinical Implications and Future Research Directions
The findings of this scoping review have significant clinical implications for bariatric surgeons, health care professionals, and policymakers involved in the management of morbid obesity. Understanding the diverse complications associated with LSG and the innovative interventions available provides a foundation for evidence-based decision-making in clinical practice.
Bariatric surgeons should consider individualized approaches to nutritional management after LSG. For instance, prolonged multivitamin supplementation may not be universally necessary, and monitoring laboratory values can guide the administration of specific supplements when deficiencies occur. The successful management of complications through plication techniques and the OTSC system suggests that these interventions could be integrated into standardized protocols for postoperative care.
Furthermore, these findings highlight the importance of developing comprehensive postoperative care strategies that include early detection and intervention for complications such as staple-line leaks, stenosis, hemorrhage, infection, gastric volvulus, and nutrient malabsorption. Future research should address the feasibility, cost-effectiveness, and generalizability of these interventions across diverse patient populations and health care settings.
Conduct well-designed RCTs to directly compare the effectiveness, safety, and long-term outcomes of various staple-line reinforcement techniques. Investigate less-studied methods, such as bioabsorbable reinforcement, to provide a comprehensive understanding of their efficacy. Conduct prospective studies to establish standardized protocols for the early detection, intervention, and follow-up of SS. Explore innovative plication techniques and their role in preventing and managing stenotic complications. Conduct prospective and RCTs to evaluate the effectiveness of the OTSC system in diverse patient cohorts. Investigate its role in preventing and managing bleeding complications in comparison with traditional reinforcement techniques. Conduct studies to identify biomarkers or patient characteristics that can predict nutritional deficiencies after LSG. Investigate the efficacy of personalized nutritional plans, considering factors such as age, sex, and preoperative nutritional status. Incorporate patient-reported outcomes and quality-of-life assessments in research studies. Evaluate the psychosocial aspects of LSG, including patient satisfaction, mental health, and adherence to postoperative recommendations. Investigate the economic implications of innovative interventions and their cost-effectiveness. Future studies should consider standardized reporting of outcomes, enabling better comparisons and meta-analyses to inform evidence-based practice.
By addressing these research directions, future studies can provide valuable insights into optimizing LSG outcomes, enhancing patient quality of life, and ensuring the effective management of postoperative complications. The dynamic nature of bariatric surgery requires ongoing research to keep up with emerging techniques and technologies, ensuring that clinical practice remains at the forefront of innovation and patient care.
Limitations
Although the scoping review provides valuable insights into the management of complications in LSG, it is essential to acknowledge certain limitations that may impact the interpretation of the findings, including potential publication bias. Studies with statistically significant results were more likely to be published. Negative or inconclusive findings might have been underrepresented, potentially skewing the overall assessment of the interventions and outcomes associated with LSG. The studies included in this review were conducted in different geographical locations, reflecting diverse health care systems, patient demographics, and surgical practices. The variability in regional factors may limit the generalizability of the findings to a broader, more global context. Other limitations include language restrictions and the exclusion of gray literature, which could impact the comprehensiveness of the findings. Variability in study design, patient demographics, and geographical location should also be acknowledged as potential sources of heterogeneity. Finally, some of the included studies may have had relatively short-term follow-up periods, limiting their ability to assess the long-term durability and sustainability of interventions. Long-term outcomes, particularly those of staple-line reinforcement techniques and SS management, may not be fully captured.
Conclusion
In conclusion, this scoping review provides a comprehensive overview of innovative approaches to managing complications in adult patients undergoing LSG for the treatment of morbid obesity. This review underscores the significance of staple-line leaks and SS in LSG. These complications can have substantial consequences on patient outcomes and may require tailored interventions for effective management. The included studies highlighted the diversity of interventions, including SLR techniques, plication techniques, and OSCS. The recognition that prolonged multivitamin supplementation may not be universally essential post-LSG emphasizes the importance of individualized nutritional management. This finding advocates a personalized approach to postoperative care that considers patient-specific factors and monitoring deficiencies. The findings from this review underscore the importance of ongoing research to fill the existing gaps in the literature and further refine evidence-based clinical practice in the dynamic field of bariatric surgery.
Footnotes
Authors’ Contributions
C.W.: supervised other authors, helped integrate data, paper drafting, and editing. A.N.: contributed to conceptualization, literature search, screening, and writing. W.H.: provided additional data, helped interpret the results, and edited the article. H.J.: identified gaps and proposed solutions for further research.
Author Disclosure Statement
All authors have read and approved the article.
Funding Information
No funding was received for this article.