
Abstract
Background:
Laparoscopic procedure for rectal prolapse has extend throughout the world as a minimally invasive treatment. Various techniques have been reported regarding the use of mesh, fixation, and rectal mobilization. However, a standard technique has not been established yet.
Method:
The original procedure of laparoscopic ventral mesh rectopexy was modified as described below. The posterior rectal cavity was dissected in proximity to the levator ani, and the lateral ligament was partially divided. After mobilization of the rectum, trimmed polypropylene mesh was placed on the ventral side of the upper rectum and fixed. The mesh was fixed in a semi-spiral shape along the long axis of the intestinal tract.
Results:
Fifteen patients underwent this procedure. The length of rectal prolapse were 5 (4–30) cm. The grade of rectal prolapse according to the Oxford Grading System was V in all patients. The median operative time and blood loss were 176 (range: 100–252) minutes and 0 (0–43) mL, respectively. No postoperative complications were observed in any of the patients. One patient experienced recurrence (6.7%). The remaining 14 patients did not experience recurrence during the follow-up period, which had a median of 54.5 months (range: 6–119 months).
Conclusion:
This modified laparoscopic semi-spiral mesh rectopexy may be considered for the surgical treatment of rectal prolapse.
Introduction
The application of minimally invasive approaches, such as laparoscopic and robotic surgery, has expanded worldwide, and these surgical procedures are also becoming common as abdominal approaches for rectal prolapse. Such approaches are also reported to be associated with better functional outcomes and lower recurrence rates than the perineal approach. 1 The recurrence rate was significantly reduced, and a recent review article reported recurrence rates of laparoscopic rectopexy as follows: 0%−12% for laparoscopic suture rectopexy, 0%−12% for laparoscopic posterior mesh rectopexy, and 0%−8% for laparoscopic ventral mesh rectopexy. 1 Under these conditions, various techniques have been reported for mesh, fixation, and rectal mobilization. However, a standard technique has not been established yet.
Laparoscopic ventral mesh rectopexy is a surgical procedure used to manage rectal prolapse.2,3 This method involves fixation of the mesh with the ventral rectum onto the sacral promontory without mobilization of the posterior wall of the rectum.2,3 While this procedure only requires mobilization of the anterior side of the rectum, it may not be sufficient to address any posterior rectal prolapse, potentially leading to recurrence.
Given the above, we modified this procedure by adding mobilization of the posterior wall, expecting secure curability and a reduced recurrence rate, and fixing the mesh by wrapping it around the rectum in a semi-circumferential spiral. We herein report the cases of laparoscopic modified ventral mesh rectopexy and discuss the outcomes of this study.
Materials and Methods
Patients
A retrospective study was conducted among 15 consecutive patients who underwent laparoscopic-modified ventral mesh rectopexy at a single institution in the Department of Surgery, Faculty of Medicine, Saga University, between September 2013 and February 2024. The medical records of all the patients were reviewed in detail.
Surgical procedure
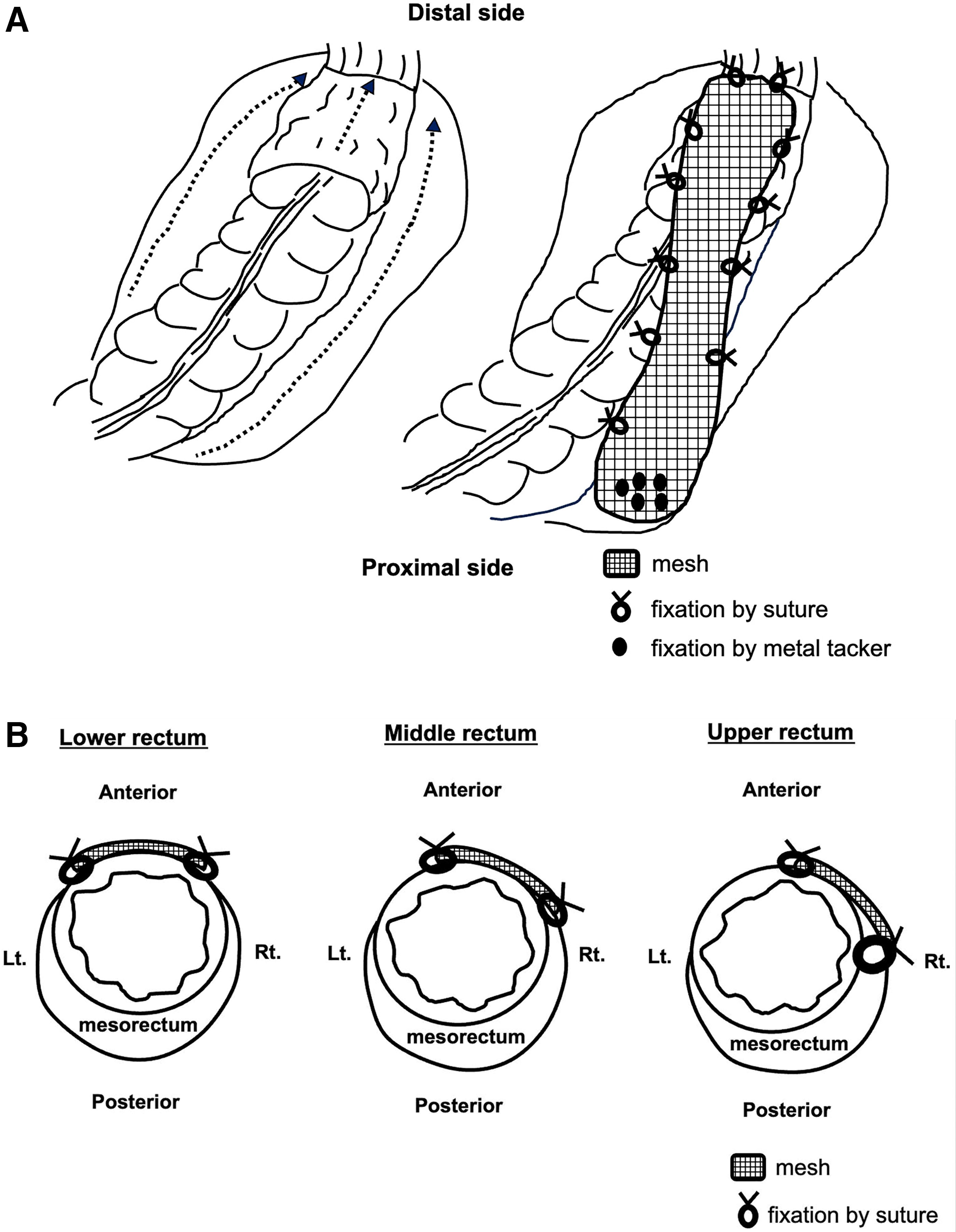
Each patient was placed in the lithotomy position, and five ports were placed. The movie of this procedure is shown in the Supplementary video SV1. [Scene 1] Mobilization of the rectosigmoid and rectum was initiated with an incision in the serosa on the right side of the rectosigmoid, entering the posterior rectal cavity and preserving the hypogastric nerve (Fig. 1a). [Scene 2] The serosal membranes on either side of the rectum were incised to further mobilize the rectum toward the anal side (Fig. 1b). [Scene 3] The posterior rectal cavity was dissected in proximity to the levator ani. [Scene 4] The incision was made at the peritoneal reflection, and the rectum was dissected (Fig. 1c). [Scene 5] After mobilization of the rectum, a trimmed polypropylene mesh (5 × 15 cm) was placed on the ventral side of the upper rectum and fixed with 3-0 or 4-0 sutures (Fig. 1d). [Scene 6] The mesh was pulled cephalad to confirm that the rectal prolapse had refluxed and then fixed to the sacral promontory using a metal tacker (Fig. 1e). The mesh was additionally fixed in a semi-spiral shape from the right lateral wall of the rectum and near the posterior wall, if possible (Fig. 1f). The peritoneum of the pelvic floor was sutured with 3-0 barbed sutures and/or 4-0 monofilament to avoid mesh exposure (Fig. 1g). The schema of the procedure is shown in the Figure 2a and 2b.
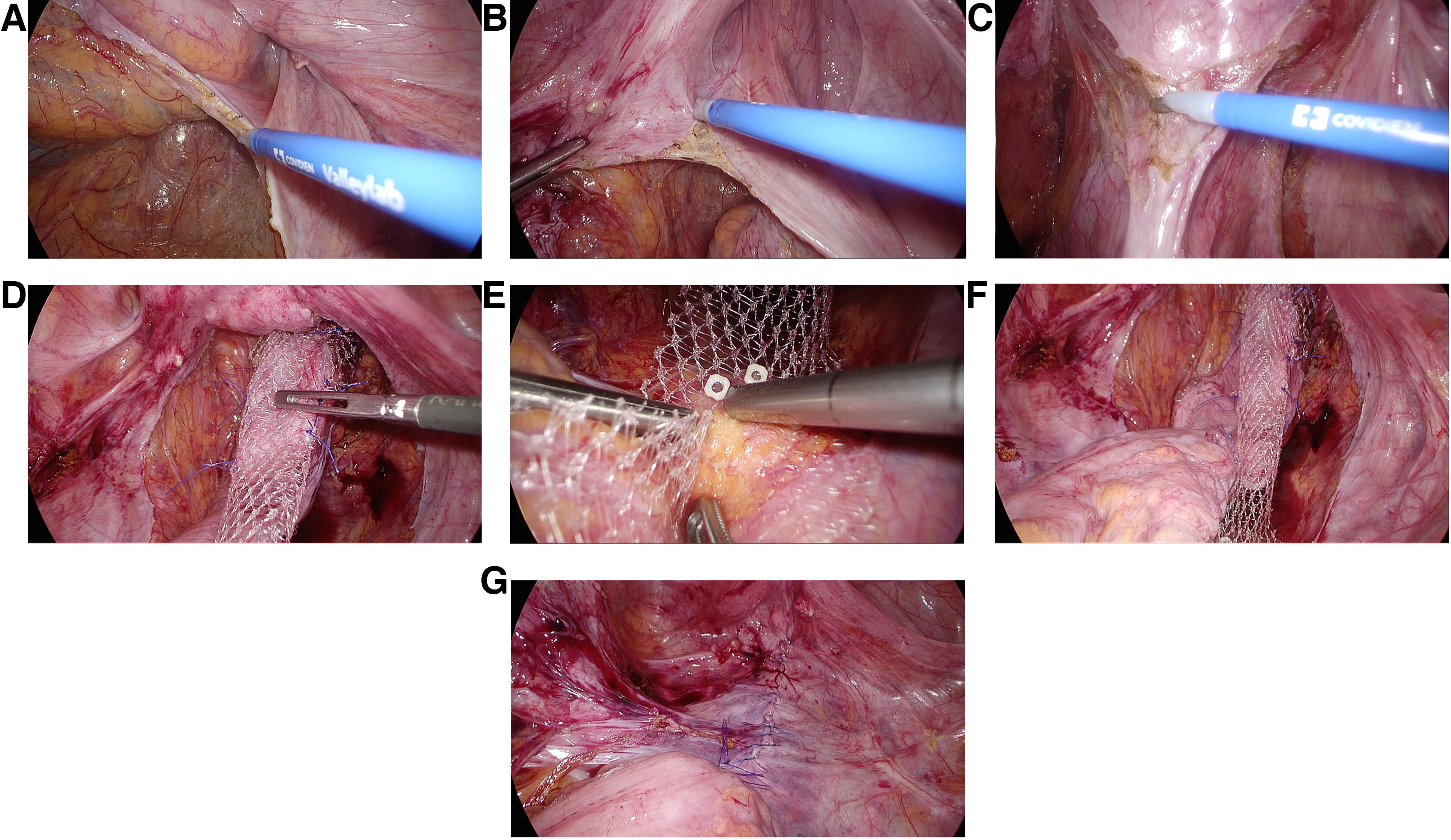
The mobilization of the rectosigmoid and rectum with an incision in the serosa on the right side of rectosigmoid and entering the posterior rectal cavity
Results
The patient characteristics are shown in Table 1. Fifteen patients (2 males and 13 females) underwent this procedure. The median age, body mass index, period of illness, and length of the rectal prolapse were 80 (range: 40–92) years old, 22.4 (range: 17.0–28.4) kg/m2, 2 (1–27) months, and 5 (4–30) cm, respectively. The grade of rectal prolapse according to the Oxford Grading System was V in all patients. A history of surgical treatment with perineal approaches for rectal prolapse was seen in 4 patients (27%). Coexisting pelvic organ prolapse was observed in 3 patients (20%). The results of the operations and their outcomes are shown in Table 2. The median operative time and blood loss were 176 (range: 100–252) minutes and 0 (0–25) mg, respectively. No conversion to laparotomy was observed. No postoperative complications were observed in any of the patients, and the median postoperative hospital stay was 6 days (range: 5–15). One patient experienced recurrence (6.7%). The remaining 14 patients did not experience recurrence during the follow-up period, which had a median of 54.5 months (range: 6–119 months).
Patient Characteristics
Results of the Operation and Outcomes
CD, Clavien–Dindo.
Discussion
The original technique of laparoscopic ventral mesh rectopexy involves dissection over the right side of the sacral promontory, extended in an inverted J-shape along the rectum and over the pouch of Douglas. 3 This procedure does not require rectal mobilization or lateral dissection, and the mesh is sutured to the ventral aspect of the distal rectum and securely fixed onto the sacral promontory.2,3 This procedure effectively reduces the recurrence rate of rectal prolapse compared with the perineal approach. 1 However, this procedure does not require mobilization of the posterior rectal wall. Consequently, Sileri et al. raised the concern that anterior “pexy” alone may not be sufficient for certain patients, and attention should also be paid to addressing any posterior residual prolapse. 4 Therefore, adequate dissection of the posterior rectal space and cephalic traction of the rectum are necessary.
The novel procedures in this approach included the additional mobilization of the posterior wall, expecting to secure curability and reduce the recurrence rate, and involved fixing the mesh by wrapping it around the rectum in a semi-circumferential spiral. The essence of our procedure was to dissect the posterior rectal cavity up to the proximity of the levator ani. To obtain full contraction of the lower rectum cephalad, this would be indispensable. Since mesh fixation to the rectum is not limited to a single point but rather spirals along the long axis of the rectum, intestinal peristalsis may be less likely to be inhibited than with other approaches of mesh rectopexy. Fixation of the mesorectum alone, such as suture rectopexy, may result in mesorectal extension and recurrence. Therefore, the use of mesh and fixation with the rectal wall would be essential.
A recent review revealed varying constipation rates after different rectopexy procedures, ranging from 0% to 44%, including laparoscopic suture rectopexy, laparoscopic posterior mesh rectopexy, and laparoscopic ventral rectopexy. 1 Postoperative constipation may be a cause. The first reason for this is related to the inhibition of normal bowel movements due to rectal fixation with the mesh. The new-onset constipation rate seems to be higher with posterior mesh rectopexy than with other procedures. 1 This may be because the mesh was fixed in a band at a single point in the short-axis direction relative to the intestinal axis, which prevented intestinal peristalsis. Fixing the mesh in a spiral pattern against the rectum may be one way to solve this problem. The second cause of new-onset constipation is rectal mobilization and lateral ligament division, potentially causing autonomic nerve injury and bowel dysmotility.5,6 Laparoscopic suture rectopexy requires complete mobilization of the rectum to the level of the levator muscle. A topic for future discussion is the degree of constipation associated with dissection and passivation of the posterior rectal space. We lack sufficient data to examine the long-term outcomes of fecal incontinence, as most of the patients were elderly, and it was challenging to follow them as outpatients. Therefore, future studies are required to confirm these long-term results.
The present retrospective study had some limitations. This study was conducted at a single institution and included a small number of patients. In addition, follow-up period is not insufficient to evaluate the outcome. Therefore, further studies are needed to confirm the efficacy of laparoscopic modified semi-spiral mesh rectopexy for rectal prolapse.
Conclusion
This modification of laparoscopic ventral mesh rectopexy may be acceptable in the treatment of prolapse recti. However, the long-term results in a large number of patients, including recurrence, constipation, fecal incontinence, and mesh-related complications, remain controversial. Therefore, further studies are required. In addition, improvements to reduce the recurrence rates may be necessary.
Footnotes
Authors’ Contributions
M.H., Y.K., S.M., H.M., S.T., T.M., and H.N. treated the patients. M.H. wrote the drafting of article. All the authors made critical revision of article. All authors approved the final version of the article.
Availability of Data and Material
The datasets generated during this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All patients and their families were informed of the surgical procedure and provided written consent. Broad consent was obtained for the present study. The medical ethics committee of Saga University reviewed and approved this study (permission number: 2019-09-R-03).
Disclosure Statement
All the authors declared no conflicts of interest.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.