
Abstract
Background:
Incisional hernias (IHs) represent a frequently encountered postoperative complication in patients undergoing liver transplantation. Traditionally, these hernias have been addressed through open surgical techniques. However, laparoscopic repair has been increasingly recognized for its association with a reduced complication rate in the management of ventral hernias. Our objective is to conduct a comparative analysis of the outcomes associated with open versus laparoscopic repair techniques in liver transplant recipients.
Methods:
We conducted a comprehensive literature review across multiple databases, including PubMed, Cochrane, LILACS, SciELO, and EMBASE, to identify studies that compare the efficacy of open and laparoscopic repair methods for IHs postliver transplantation. For the statistical analysis of gathered data, we used the Review Manager software, version 5.4. To evaluate the variability among the study outcomes, we assessed heterogeneity using the I2 statistic.
Results:
After an initial screening of 334 studies, 6 studies with a combined total of 338 patients fulfilled our inclusion criteria. Our analysis revealed that laparoscopic repair tends to be associated with longer operation times, with a mean difference of 20.30 minutes (confidence interval [CI]: 2.14–38.46; P = .03). We observed no significant differences between laparoscopic and open repair regarding infection rates, recurrence rates, overall surgical complications, or hospital stay duration.
Conclusion:
Both surgical approaches yield comparable postoperative outcomes. However, laparoscopic repair is associated with an increased operation time duration. To substantiate these findings, further research involving prospective, randomized studies is necessary.
Introduction
The emergence of incisional hernia (IH) as a frequent outcome following midline laparotomy during abdominal surgery underscores the enduring challenge of postoperative complications. Notably, this issue extends beyond conventional abdominal procedures, as evidence suggests that IH is a prevalent concern following liver transplantation, with reported incidence rates spanning from 5% to 46%. 1 Liver transplant (LT) recipients, characterized by their immunosuppressive regimens, intricate comorbidities, and type of abdominal incision, especially Mercedes type (large transverse associated with midline), confront a heightened susceptibility to postoperative wound complications.1,2
For a comprehensive understanding of the incidence of IHs within this population, an in-depth review and synthesis of the primary research literature are crucial. Previous analyses have focused on the incidence of IH post-liver transplantation. Butler et al. 3 utilized a proportional meta-analysis to assess the incidence rates across studies that encompassed both laparoscopic and open surgical repair methods, providing a pooled incidence rate for each technique separately. Another study by Frountzas et al. focused solely on the frequency of hernia occurrence and its subsequent recurrence rate without differentiating between the surgical techniques used for hernia repair. 4
Our study aims to enhance clarity by conducting a systematic review and meta-analysis that directly compare both outcomes of laparoscopic versus open repair techniques in LT patients with IH.
Materials and Methods
Search strategy and data extraction
This review was conducted according to the recommendations from the Cochrane Collaboration and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement guidelines. 5 The literature review was conducted independently by two authors (V.S. and J.P.G.K.). PubMed and EMBASE databases were searched from inception to October 2023 for studies published using the following heading terms: “Incisional Hernia” and “Liver transplantation.” We did not restrict the publication years. The prespecified research protocol has been registered and it is available at PROSPERO CRD42024547820.
Eligibility criteria
Studies that met the following criteria were included: (1) studies including LT patients who underwent IH repair; (2) studies that compared laparoscopic repair versus open repair; (3) studies that reported at least one of the outcomes of interest; and (4) studies in English, Portuguese, and Spanish. Reviews, case reports, and editorials were excluded.
Outcomes of interest
A systematic review and meta-analysis on the following endpoints were conducted: infection rate, recurrence rate, length of hospital stay, operative time, and overall surgical complications (including infection, seroma, hematoma, ileus, wound dehiscence, and recurrence).
Quality assessment
We used the Cochrane Collaboration tool to assess the Risk of Bias in Nonrandomized Studies of Interventions 6 to appraise the nonrandomized studies. Each study was categorized as critical, serious, moderate, and low risk in all the following seven domains: confounding, selection, classification, deviations from intended interventions, missing data, measurement of the outcomes, and selection of reported results. Risk of bias and quality assessment of each study were performed independently by two authors (J.P.G.K. and V.S.).
Statistical analysis
We conducted this systematic review and meta-analysis according to the recommendations from the Cochrane Collaboration and the PRISMA statement guidelines. Review Manager 5.4 (Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) was used for statistical analysis. Odds ratio (OR) was used to determine the effects of binary outcomes with 95% of confidence intervals (CIs). Weighted mean differences were used for continuous outcomes. Cochran Q test and I2 statistics were used to evaluate heterogeneity; P values inferior to .10 and I2 > 25% were considered significant for heterogeneity. A fixed-effect model was used for endpoints with I2 < 25%, low heterogeneity, and a random-effects model when the heterogeneity was high.
Results
Study characteristics and selection
We searched 334 results; 14 remained for full-text review after removal of the duplicates and studies that did not meet inclusion criteria based on title and abstract screening, detailed in Figure 1. We included six studies in our analysis,7–12 comprising 338 patients: 109 (32%) in the laparoscopic group and 229 (68%) the open repair group. Table 1 summarizes the baseline characteristics between the groups.
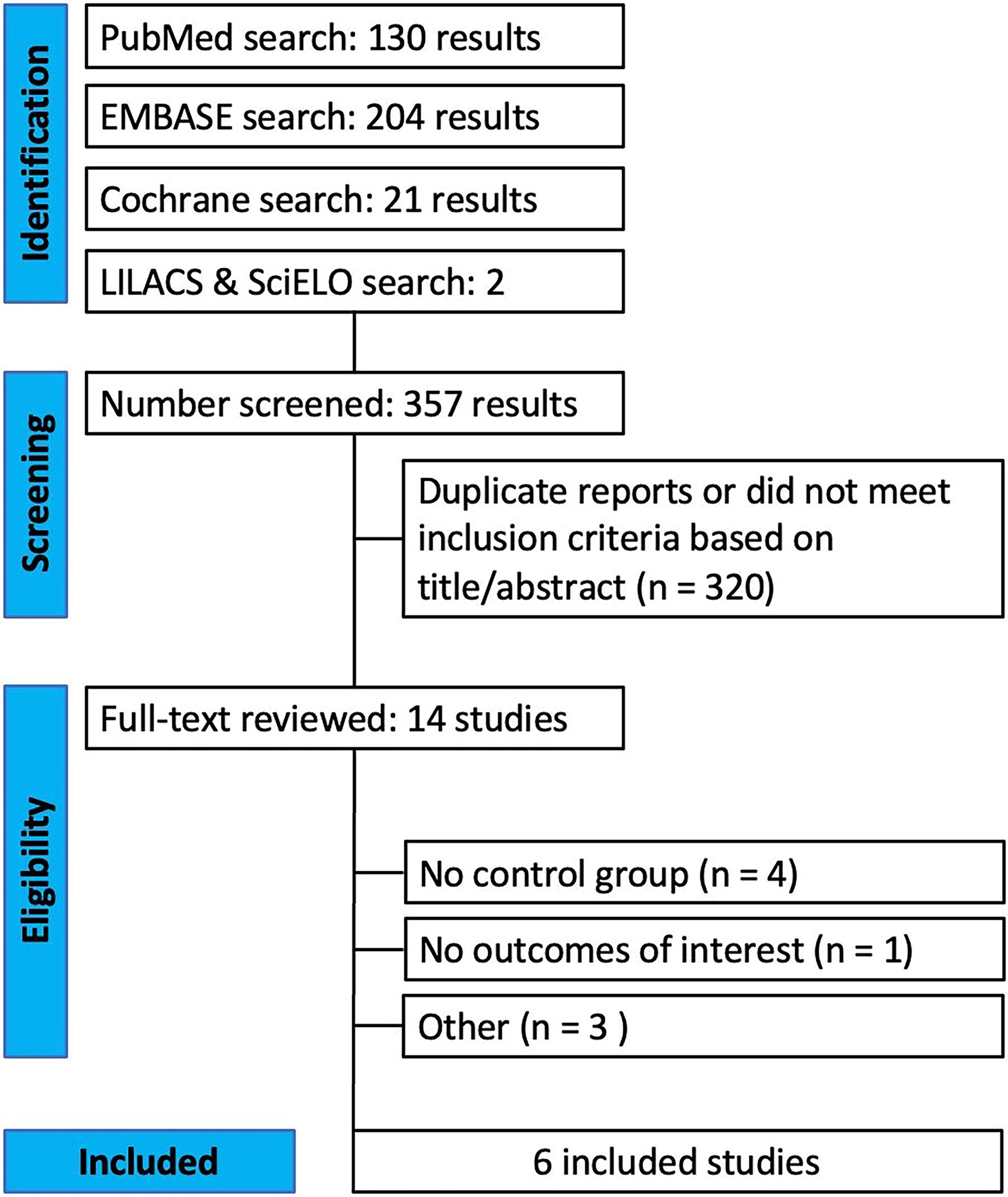
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flowchart.
Characteristics and Intraoperative Outcomes in Identified Studies on Incisional Hernia of Patients Following Liver Transplantation Comparing Open Versus Laparoscopic Approaches
Categorical data are presented as absolute numbers. Continuous data are presented as median (range) or mean (±standard deviation).
BMI, body mass index; HBV, hepatitis B viral infection; HCV, hepatitis C viral infection; LT, liver transplant; MELD score, model for end-stage liver disease score.
Pooled analysis
Five studies reported the infection rate and length of hospital stay (LOS), and five reported the recurrence rate. Not every study reported the other major outcomes of interest, such as wound dehiscence and hematomas. Table 2 summarizes the operioerative outcomes.
We performed analysis on the four major endpoints. The meta-analysis found that laparoscopic repair was associated with increased operation time compared with open repair with the mean difference (MD: 20.30; CI: 2.14–38.46; P = .03) (Fig. 2). On the contrary, no significant difference in the infection rate was found between the groups (OR: 1.12; CI: 0.34–3.63; P = .85) (Fig. 3).

Operation time: laparoscopic versus open.

Infection rate: laparoscopic versus open.
The LOS was comparable between the laparoscopic repair and open repair (MD: 0.67; CI: −2.30 to 0.97; P = .42) (Fig. 4). Both groups presented similar recurrence rates (OR: 0.61; CI: 0.28–1.33; P = .22) (Fig. 5). There was no difference in overall surgical complications in the groups (OR: 0.59; CI: 0.31–1.13; P = .11) (Fig. 6).
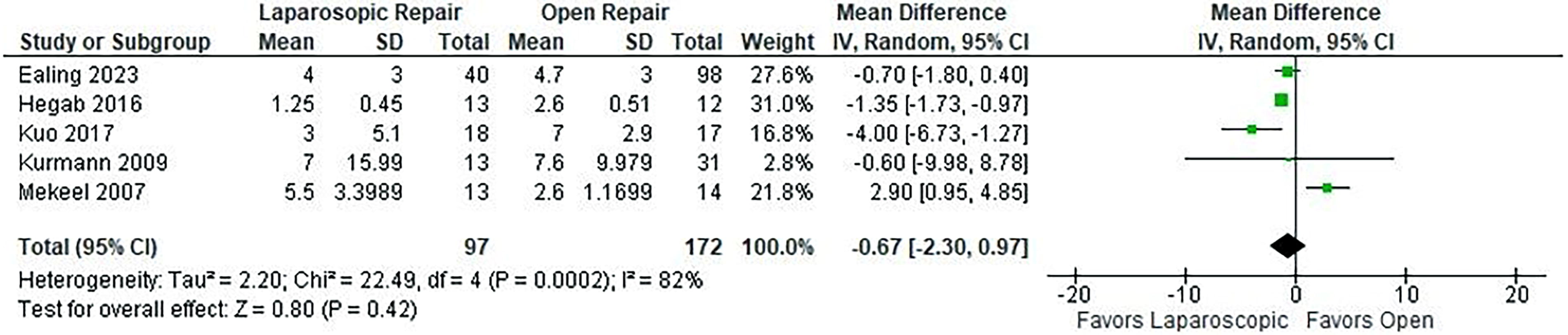
Length of hospital stay: laparoscopic versus open.

Recurrence rate: laparoscopic versus open.
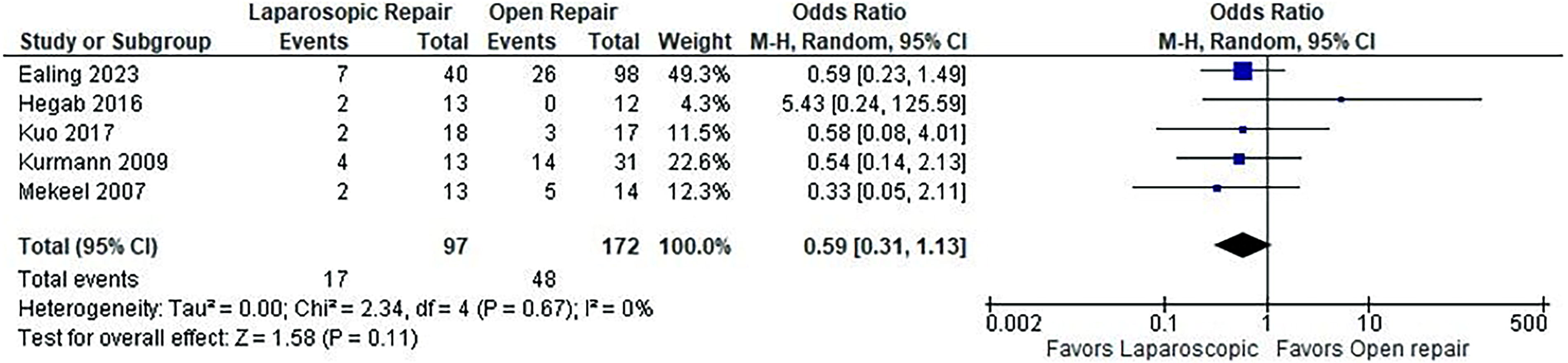
Overall surgical complications: laparoscopic versus open.
Perioperative and Outcomes Related to Incisional Hernia in Patients Following Liver Transplantation Comparing Open Versus Laparoscopic Approaches
Categorical data are presented as absolute numbers. Continuous data are presented as median (range) or mean (±standard deviation).
HBV, hepatitis B viral infection; HCV, hepatitis C viral infection; MELD score, model for end-stage liver disease score.
Quality assessment
We included six nonrandomized studies in this meta-analysis. The appraisal of each individual study is reported in Supplementary Figure S1. In summary, most of the studies were classified as having moderate risk of bias, and one study was classified as having serious risk of bias.
Discussion
This systematic review and meta-analysis of six studies and 338 patients compared the outcomes between open repair versus laparoscopic repair of IH following LT. The main findings in our study were that laparoscopic IH repair following liver transplantation is associated with prolonged operative time compared with open repair, with similar Surgical Site Infection (SSI) rate between the groups. Finally, there was no difference in LOS, recurrence rate, and overall surgical complications.
IH is a prevalent complication following LT. Laparoscopic repair has been proven to decrease complication rates and shorten the length of stay in ventral hernia repair compared with conventional open repair.13,14 In the transplant population, open repair is still widely used due to concerns about intra-abdominal adhesion and complications related to immunosuppression when performing laparoscopic repair. Studies have investigated the laparoscopic repair of IH after LT.7–12 Prior meta-analysis included 18 studies, most of which were either laparoscopic repair or open repair; the authors performed a proportional meta-analysis and compared pooled outcomes of the laparoscopic approach versus open. 4 This is the first meta-analysis that included only studies that compared both approaches in the analysis.
Pereira et al., in their randomized controlled trial with 60 patients undergoing ventral hernia repair, found longer operative time in the laparoscopic group compared with open (P < .01). 15 Similarly, Kuo et al. reported longer operative time in the group of patients undergoing laparoscopic repair for IH repair after LT. However, other similar studies did not find the difference between the two approaches.8,9 This meta-analysis also found that laparoscopic repair is associated with prolonged operation time when compared with the open technique. This might happen due to the challenging nature of the laparoscopic repair, which includes extensive lysis of adhesions for proper defect closure and mesh positioning.
Surgical site infection is a common complication after IH repair in LT patients. Frountzas et al. reported an overall incidence (17%) of surgical site infections. Most of the studies that evaluated the incidence of infection after hernia repair in transplant patients did not find a difference when comparing the two approaches, laparoscopic versus open.8,10,12 Our analysis found a comparable infection rate between the two surgical approaches.
The recurrence rate following hernia repair in the transplant population is concerning; a meta-analysis reported a recurrence rate of 12.4% after first repair. 3 Five studies included in this meta-analysis reported recurrence rate, with follow up between 6 and 61 months. Individually, all the studies did not find significant differences between the groups.7–11 Frountzas et al., in their proportional meta-analysis, reported a higher pool net recurrence rate after open repair (12%) compared with laparoscopic repair (6%). 4 In our study, combining studies that evaluated both approaches, we did not find a significant difference in the recurrence rate (OR: 0.61; P = .22).
Laparoscopic ventral hernia repair in nontransplant patients is associated with shorter LOS. 15 Ealing et al. reported shorter hospital stays with the laparoscopic approach in LT patients with large hernia (>5cm) undergoing IH repair. On the contrary, Mekeel et al. reported prolonged hospital stays in laparoscopic repair compared with open repair in LT patients (P = 0.0059) in their analysis. The pooled analysis did not find a statistically significant difference in the LOS. In the same way, the overall surgical complications were similar between the two groups.
Limitations
This is the first meta-analysis that evaluated only studies that compared laparoscopic versus open approaches. However, this study has limitations. First, our data are mostly based on observational studies, and we cannot infer causality. Second, the sample size was small; in addition, the laparoscopic group had a lower follow-up period. Third, studies reported different LT incision types, and the type of mesh used widely varies across the studies. And lastly, some of these studies are susceptible to retrospective data collection bias. Larger randomized controlled trials are required to provide more robust evidence.
Conclusion
Our findings indicate that the laparoscopic technique does not exacerbate the risk of infection, extend the hospitalization period, increase the rate of hernia recurrence, or elevate the overall rate of surgical complications when compared with open repair, however, it is associated with a longer surgical duration.
Footnotes
Authors’ Contributions
Each of the authors contributed significantly to this research as per the guidelines of the International Committee of Medical Journal Editors. Study design: V.S., J.P.G.K., D.L.L., L.T.C., F.M., and R.N. Data collection and analysis: V.S., J.P.G.K., D.L.L., and R.N. Article preparation and editing: V.S., J.P.G.K., D.L.L., F.M., and L.T.C.
Disclosure Statement
V.S., J.P.G.K., D.L.L., R.N., and P.S. disclose no conflict of interest. L.T.C. discloses consulting fees from BD and Medtronic outside the submitted study. F.M. discloses consulting fees from BD, Intuitive, Integra, DeepBlue, Allergan, and Medtronic, outside the submitted study.
Funding Information
There was no funding for this project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.