
Abstract
Background:
Surgeons are exposed to unavoidable distractions while operating. Distractions can cause stress, and stress can impair cognition and motor skills to the detriment of surgeon performance. This study assessed the impact of distractions on surgeon stress levels and surgeon performance during simulated laparoscopic tasks.
Methods:
Twelve surgical trainees completed a peg-thread transfer task three times on a laparoscopic simulator in a neutral environment. Six trainees then completed the task three more times in an environment overlain with distractions commonly found in the operating theatre. Six others completed three more tasks in a neutral environment. Stress was measured by recording heart rate and by assessing responses to the NASA Task Load Index. Performance was measured using instrument tracking metrics and time to complete the task.
Results:
The distracted participants reported significantly higher effort, frustration, and physical demand than the neutral group, as measured by the NASA Task Load Index, (P = .001, .031, and .044, respectively). The neutral group completed their final task significantly faster compared with baseline (P = .049), while the distracted group failed to show this improvement. The distracted group showed higher hand discordance, suggesting reduced ambidexterity.
Conclusion:
Distraction negatively impacted some aspects of performance and resulted in subjective increased stress. In future, simulation may have a role in “stress inoculation,” enabling surgeons to maintain performance, despite distractions.
Introduction
While stress can motivate, there is a point at which high stress levels impair ability 1 and when arousal may be too high to be beneficial to performance. 2 The relationship between stress and performance is relevant to surgeons. High levels of stress can impair task completion when “divided attention, working memory, retrieval of information from memory, and decision making” are crucial. 3 These skills are needed in surgery to ensure effectiveness, efficiency, and patient safety. Distractions in surgery include personnel movements, talking, smartphone use, telephone calls, and missing instruments/materials. 4 Surgeons exposed to stress report feeling “shaky, clumsy, less dexterous, and making small mistakes.” 5 Arora et al. 6 reported that stress was associated with increased time to complete tasks and increased errors in a simulated surgical environment. The effect of stress on performance appears to lessen as surgeon experience increases, 5 suggesting that experience confers the ability to better maintain performance in stressful situations.
Surgical simulation has become increasingly popular as the traditional apprenticeship model of training moves toward a competency-based model. With reduced overall working hours and reduced operating hours, the opportunity for experience-based learning is more limited. 7 Simulation allows surgical teaching in a safe and controlled environment with no risk to patient safety. Tasks can be repeated infinitely with instant feedback, 8 and evidence has shown that simulation-based learning is transferrable to the operating theater. 9 However, the calm and stress-free environment within which surgical simulation normally takes place is not reflective of the real world, where operating room distractions and interruptions draw attention away from the core task and increase stress. 10 Currently, trainees learn to cope with this stress by making mistakes or by observing their seniors in stressful scenarios. 11
Stress inoculation training is a “cognitive behavioral approach” where people are exposed to stress in order to implement better coping techniques when stressed in real-world situations 12 and has been used successfully in aviation and military settings.13,14 Akin to this, stress habituation is a form of learning “in which the magnitude of the response to a specific stimulus decreases with repeated exposures to that stimulus.” 15 These concepts may have a role in surgical training, facilitating a decreased response to stress and potentially improving patient safety. Evidence for stress-inoculation training in health care is currently limited. However, 91% of surgical residents who undertook stress training rated it as valuable when completing future surgical tasks. 16
The aim of this study was to model stressful distractions within a simulated laparoscopic surgery environment. Furthermore, we sought to assess the impact of distraction upon performance, hypothesizing that external distractors would negatively impact surgeon performance or learning.
Materials and Methods
Twelve surgical residents in Scotland were recruited between January 2024 and March 2024. All participants had completed at least 3 years of surgical residency training, including experience in laparoscopic surgery. Informed consent from participants and regional ethical approval were obtained.
Participants were divided into two groups: distracted and neutral. All 12 completed a previously validated 17 peg-thread transfer task on a laparoscopic box simulator (eoSim, Limbs&Things, Bristol, UK). They first completed the task three times in a neutral environment to establish baseline performance measurements. The neutral group then completed three assessed tasks in the same neutral, quiet environment. The distracted group completed the task three more times in an environment overlain with distractions. An audio track played during all distracted tasks and included anesthetic machine and electrocardiogram noises, conversations unrelated to the task, and a phone ringing intermittently. Prior to the initial distracted task, the surgeon was briefed on a clinical scenario and asked to remember pertinent information for subsequent recall. During the first distracted task, an object was dropped loudly, in proximity, during task completion. During the second distracted task, the participant was questioned about the clinical case previously discussed. During the final distracted task, a nearby door was opened and closed.
Our aim was to create a simulated environment that accurately recapitulated distractions found in surgical environments. Distractors used for this study were therefore realistic and similar to those present in real operating theatres. The audio tape played for all the distracted tasks included machinery beeping, conversations unrelated to the task, and a phone ringing. Based on operating theatre observations, Feuerbacher et al. 10 found that a ringing phone and an unrelated side conversation were realistic operating room distractions and interruptions. The same study also identified the sound of a dropped metal tray to be a realistic distraction in the operating theatre. Distraction 1 in this study was therefore an object being dropped loudly in proximity. Distraction 2 involved the surgeon being asked a question about an unrelated clinical case, which the participant had been briefed on previously. Lee et al. 18 found that 72% of urologists stated that they “commonly discussed consults with trainees while in the OR.” This is an example of a realistic situation in which dual-tasking is required. Van Harten et al. 4 found that door movements were a common distractor in operating theatres, especially during induction of anesthesia, leading to distraction 3, which was the door opening and closing during the task.
All participants completed the NASA Task Load Index questionnaire 19 at the end of the study. This questionnaire is a validated tool to assess mental demand, physical demand, and temporal demand of a task, as well as failure to perform, effort used, and frustration felt during a task. Each dimension is scored on a scale from 0 to 100 in increments of 5 (with higher scores reflecting higher mental demand, higher frustration, etc.).
Time to complete the task (seconds) and instrument tracking measurements (instrument path distance, handedness, time off screen, and motion smoothness) were used to assess performance. 20 These data were collected using instrument tracking software (SurgTrac, Limbs&Things, Bristol, UK), where colored fiducials on the tips of each instrument are tracked automatically.
An Apple watch SE (Apple, California, USA) was used to measure participants’ mean heart rate during each task. To account for the learning curve associated with attempting a new task, data from task 3 (the final practice task) were used as a baseline. The percentage change for each task compared with the baseline data was calculated for each participant.
Data were analyzed using RStudio. 21 For normally distributed data with equal variances, the independent samples t-test was used. For data not normally distributed, the Mann–Whitney U test was used. For data with unequal variances, Welch’s t-test was used. Significance was set at P < .05.
Results
Stress
Figure 1 shows the mean NASA Task Load Index scores for the distracted group (red) and the neutral group (blue). Each metric of the NASA Task Load Index scored higher in the distracted group compared to the neutral. Physical demand was rated significantly higher in the distracted group with P = .0442 (95% confidence interval [CI]: 1.14, 62.2), as well as effort with P = .00153 (95% CI: 17.3, 54.3). Frustration was also rated significantly higher by the distracted group with P = .0314 (95% CI: 3.27, 56.7).
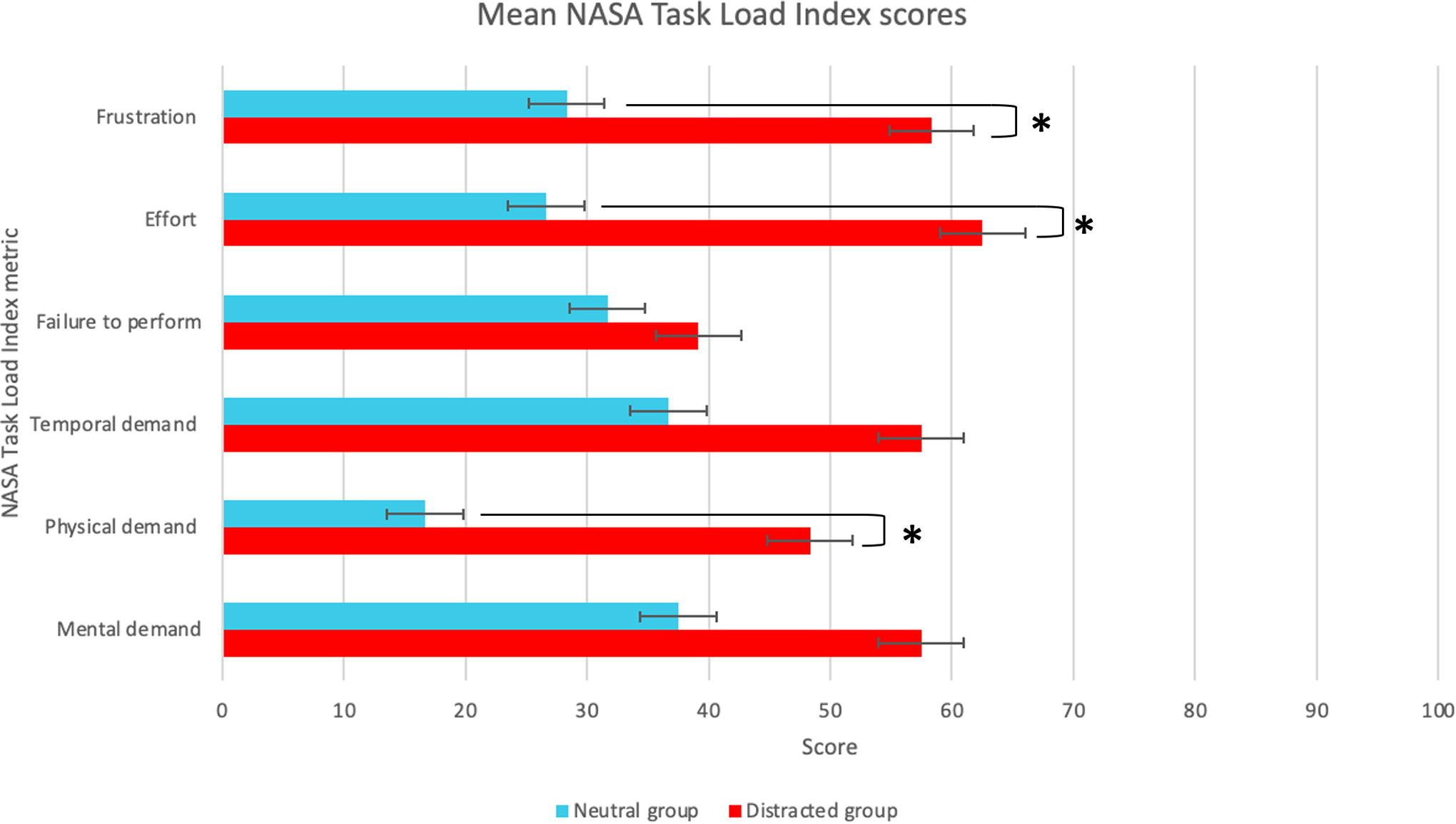
A graph to show the mean NASA Task Load Index scores for each group (* indicates a significant result).
There was no statistically significant difference between the mean heart rate of the two groups for any of the tasks. There was also no significant difference between either group’s mean heart rate in the assessed tasks compared to baseline.
Performance
Figure 2 shows the mean time taken to complete each task in seconds for the distracted group (red) and the neutral group (blue) for all three practice tasks (1–3), as well as the three assessed tasks (4–6). This graph shows both groups improving between each task until the assessed tasks, where the neutral group continues to improve and the distracted group appears to plateau.

A graph to show the mean time taken to complete each task (s) for both groups.
Figure 3 shows the mean change in time taken to complete the three assessed tasks compared with the baseline task for the distracted group. Figure 4 shows the same for the neutral group. Task 1 is the baseline, and the following 3 are the assessed tasks. There was no statistically significant difference between the two groups for each task. There was also no statistically significant difference between the distracted group’s assessed tasks compared to their baseline. The neutral group, however, became significantly faster in completing their final assessed task compared with their baseline task (P = .0493 [95% CI: 0.0556, 0.293]).

A graph to show the mean change in time taken to complete assessed tasks compared with the baseline task for the distracted group.
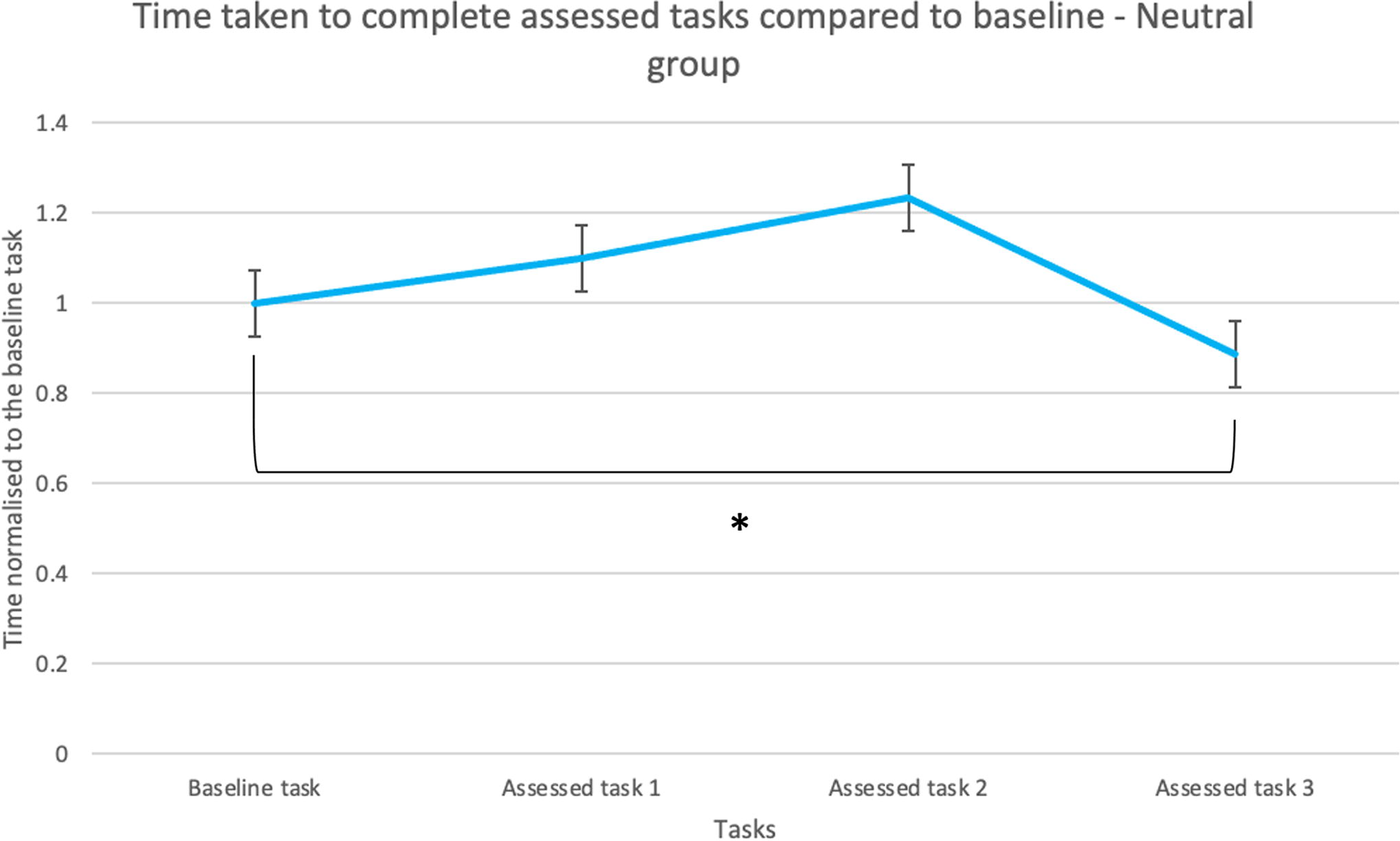
A graph to show the mean change in time taken to complete assessed tasks compared with the baseline task for the neutral group (* indicates a significant result).
Combined distance travelled by both instruments (m)
Figure 5 shows the mean change in combined distance travelled by instruments (left and right) for each assessed task, compared with the baseline for the distracted group (red) and the neutral group (blue). There was no statistically significant difference between the two groups or between the assessed tasks compared with the baseline task for either the distracted or neutral group.

A graph to show the mean change in total combined distance traveled by both instruments for the assessed tasks compared with baseline for both groups.
Time instruments spent off screen (%)
Figure 6 shows the mean change in the percentage of time instruments (left or right) was off screen during each assessed task compared with the baseline task for the distracted group (red) and the neutral group (blue). There was no statistically significant difference between the two groups, nor between the assessed tasks compared to the baseline task—for either the distracted or the neutral group.
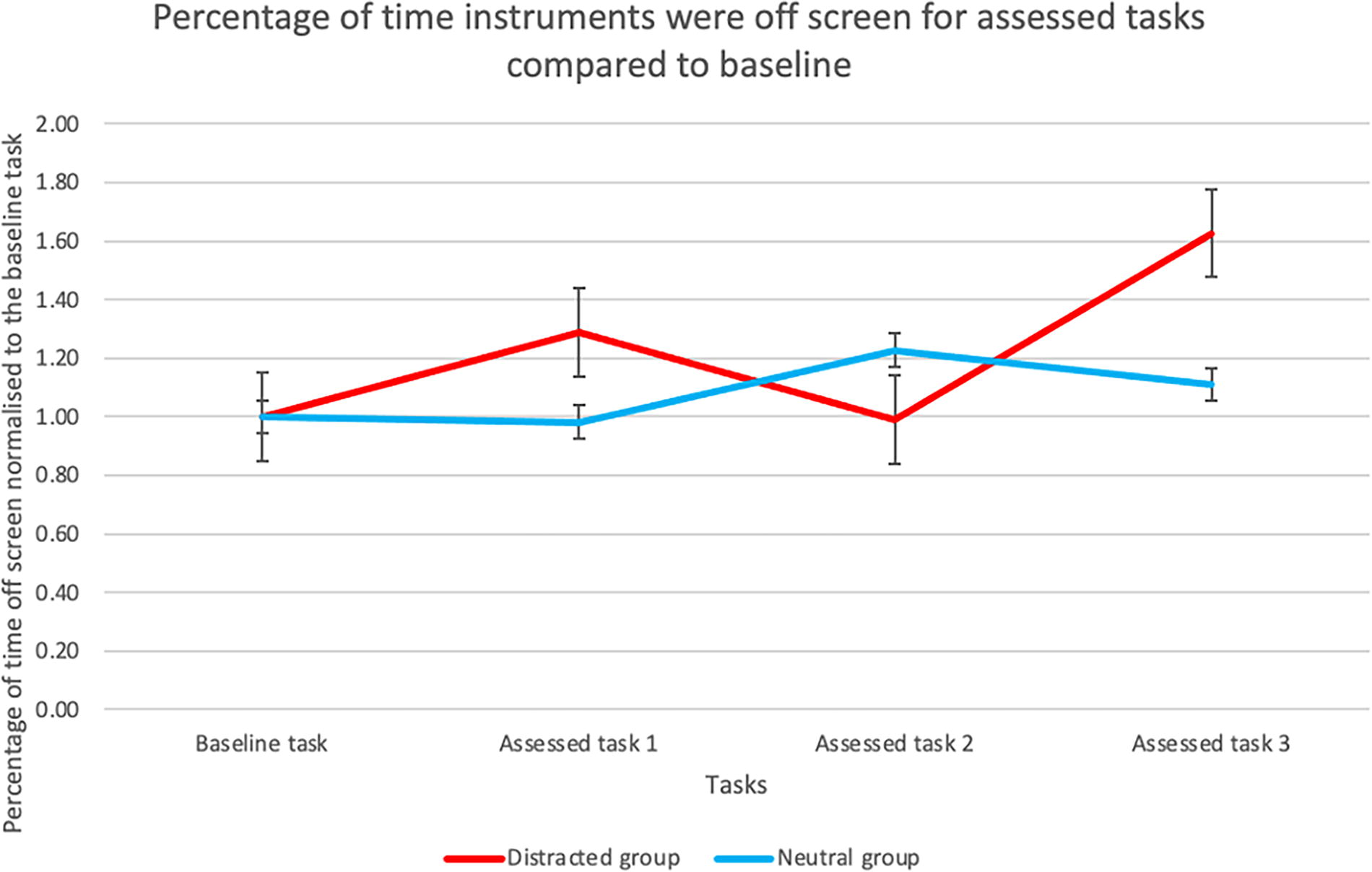
A graph to show the mean change in off screen time for both instruments for the assessed tasks compared to baseline for both groups.
Hand discordance
Hand discordance was calculated by subtracting left handedness from right handedness and converting the results to a positive number. In this way, an entirely ambidextrous surgeon who shared movements equally across left and right instruments would have a hand discordance value of 0. Figure 7 shows the mean change in hand discordance for each assessed task compared with the baseline task for the distracted group (red) and the neutral group (blue). Hand discordance increased more, when compared with baseline, in the distracted group than in the neutral group. There was no statistically significant difference between the two groups for any of the assessed tasks, although some results were very near to the 5% significance level. The difference between the two groups for the first assessed task had a P value of .0576 (95% CI: −0.137, 6.30) and the difference between the two groups for the third assessed task has a P value of .0518 (95% CI: −0.0286, 5.39). There was no statistically significant difference between any of the assessed tasks and the baseline task for either of the groups.
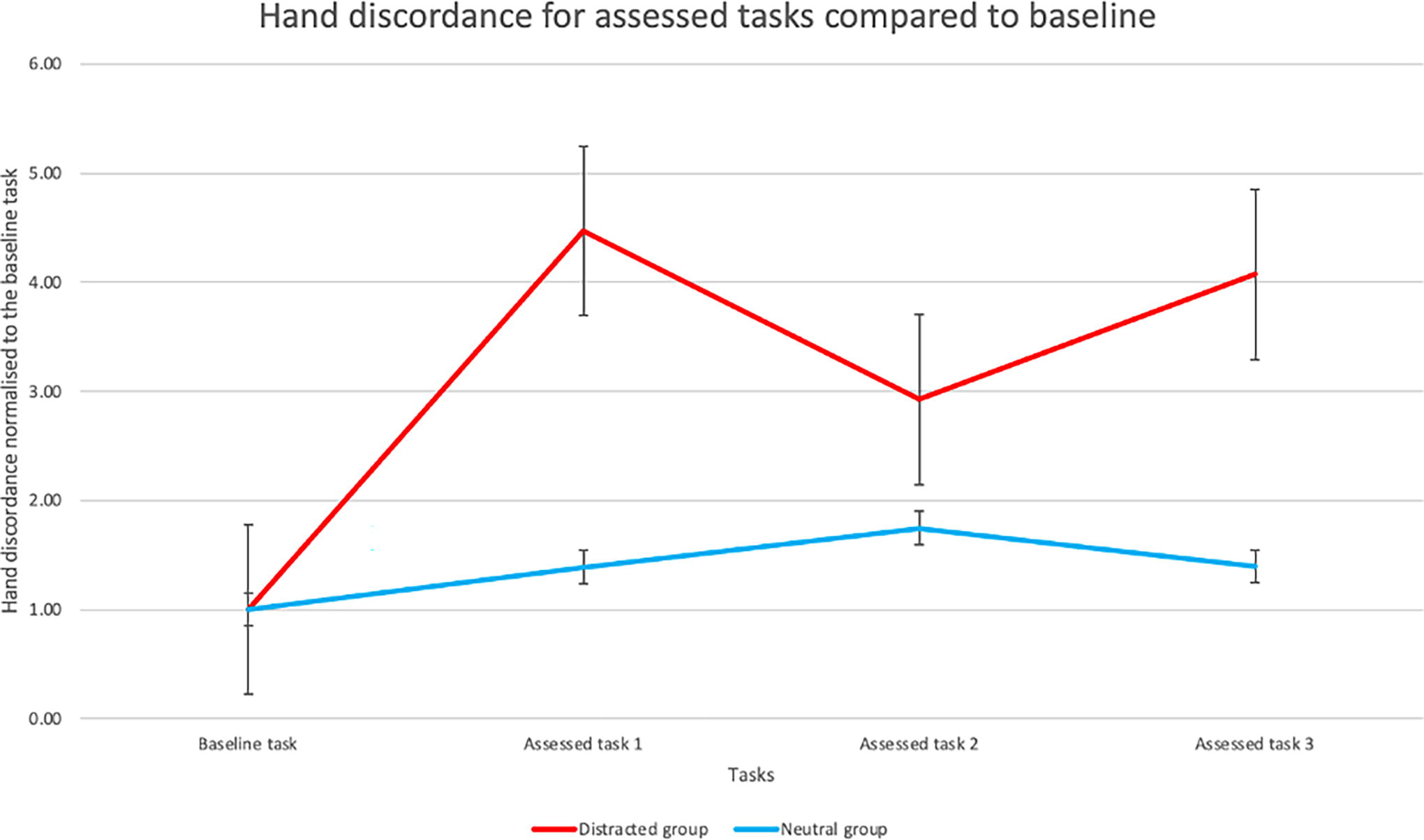
A graph to show the mean change in hand discordance for each assessed task compared to baseline for both groups.
Discussion
In this study, distracted surgeons reported higher levels of stress according to the NASA Task Load Index, rating physical demand, effort, and frustration significantly higher than the nondistracted, neutral group. This illustrates that the distracting environment successfully generated higher levels of perceived stress than the neutral environment. Mean heart rate has been shown to increase due to stressful situations. 22 In our study, however, there was no change in mean heart rate for either group compared to their baseline.
As the two groups performed differently during the practice tasks, data for each participant’s assessed tasks were normalized as a percentage change compared with their baseline performance (the final practice task). Laparoscopic performance can be assessed using motion analysis parameters such as time taken and path length of instruments. 23 Time taken to complete tasks can successfully distinguish between experienced and novice surgeons. 24 In this study, both groups showed a steep improvement in time taken during the three practice tasks, illustrating learning. The neutral group continued to learn, becoming significantly faster in their final performance compared with their baseline. The distracted group, however, failed to improve in this way. This performance plateau suggests that distraction inhibited their learning curve.
Studies have previously shown that distractions cause increased length of operating time, with more experienced surgeons having a greater ability to multitask. 25 The two surgeons with the slowest mean time taken to complete assessed tasks were both in year 3 of training, the lowest training year eligible for this study, whereas the three surgeons with the fastest mean time taken to complete assessed tasks were in years 4, 8, and 8 of training, respectively. This variation in experience may have contributed to the range of times seen, as well as the surgeon’s abilities to withstand distraction during the assessed tasks.
Distance travelled by instruments is a measure of precision, with shorter distances indicating more controlled and purposeful movements. 20 There was no significant difference between the two groups, or between the assessed and baseline tasks for either group. The neutral group appeared to stay more consistent in assessed tasks compared with the baseline, whereas the distracted group showed increased and decreased distances depending on the task.
Keeping instruments in the operative field is essential when performing laparoscopic surgery as instrument’s out of field may cause harm. There was no significant difference for percentage of time that instruments spent off screen when comparing the two groups.
Several studies have shown that more experienced surgeons have a greater degree of ambidexterity than novice surgeons.26,27 The distracted group in this study showed a higher level of hand discordance (i.e., less ambidexterity) in the assessed tasks compared with baseline and compared with the neutral group, but the difference was not statistically significant.
Implications of this study and suggestions for future work
Distracted surgeons have previously been shown to commit more surgical errors, 8 and it is known that stress can negatively impact cognitive processes and motor skills, 9 both of which are essential for surgery. Currently, there is limited focus on the management of stress associated with surgery. 16 The success of stress inoculation training in other industries should encourage healthcare to explore the same approach for surgery. 14 With simulation training becoming an increasingly necessary component of surgical curricula, 28 stress inoculation training is feasible. Future studies may focus on the effectiveness of stress inoculation training for surgeons in training, and the practicality of implementing this within training curricula. Beyond the individual, the impact of stress on wider team dynamics also demands exploration.
Limitations
This study has a small sample size, limiting the statistical power of results. The two groups were not identical in terms of surgical experience and subspecialty background. The distracted group had a mean year of training of four, whereas the neutral group had a mean year of training of six. This may have contributed to the differences in performance between the two groups. Moreover, we intentionally recruited only surgical trainees with a minimum of 3 years prior laparoscopic experience.
Mean heart rate is a simple and noninvasive method to monitor physiological stress but is not exhaustive. Other methods of monitoring stress, such as salivary cortisol, skin conductance, or heart rate variability, are frequently used in research and may have a role in future studies.
Conclusion
We have generated a simulated laparoscopic environment that incorporates realistic operating theater distractions, and these resulted in significantly increased stress to the operating surgeon. Importantly, distraction impeded learning. Future studies, with a larger number of participants performing more tasks, are needed. In future, simulation of this sort might have value in “stress inoculation,” enabling surgeons to cope with distraction and stress and therefore perform better.
Footnotes
Acknowledgements
We acknowledge Limbs & Things Ltd, UK for the loan of simulators used in this research and thank the residents for taking part.
Authors’ Contributions
I.I.: Methodology, data curation, and writing—original draft preparation. M.A.H.: Conceptualization and writing—reviewing and editing.
Disclosure Statement
I.I. has no conflict of interests or financial ties to disclose. M.H. helped to develop the eoSim simulator as part of eoSurgical Ltd., which has since been acquired by Limbs & Things Ltd, for whom he maintains a consultancy role.
Funding Information
This research did not receive any funding from agencies in the public, commercial, or not-for-profit sectors.