
Abstract
Background:
This study aimed to assess the impact of Enhanced Recovery After Surgery (ERAS) compliance and to identify which components of this protocol are most likely to affect postoperative outcomes in patients undergoing colorectal cancer surgery.
Methods:
This is a retrospective cohort evaluating patients who underwent elective colon resection. ERAS compliance was assessed based on adherence to the protocol components. The study examined the following outcomes: postoperative complications, readmission rates, mortality, conversion to open surgery, stoma creation, and length of hospital stay.
Results:
Of the 410 patients studied, 59% achieved ≥75% compliance. Comparison between compliance groups (<75% versus ≥75%) showed significant differences in overall complications (P = .002), severe complications (P = .001), and length of hospital stay (P < .001). The area under the receiver operating characteristic curve for predicting the absence of severe complications based on ERAS compliance was 0.677 (95% confidence interval: 0.602–0.752). Logistic regression analyses demonstrated that ERAS compliance was significantly associated with a reduced risk of severe complications (P < .001), as well as that the following items: avoiding prophylactic drains (P < .001), minimal use of postoperative opioids (P = .045), avoidance of postoperative salt and water overload (P < .001), postoperative nutritional support (P = .048), and early mobilization (P = .025).
Conclusion:
High ERAS compliance is associated with improved postoperative outcomes in colorectal cancer surgery. Key protocol components for preventing severe complications include avoiding prophylactic drains, minimal postoperative opioid use, avoiding salt and water overload, nutritional support, and early mobilization.
Introduction
Enhanced Recovery After Surgery (ERAS) is a comprehensive, evidence-based program designed to optimize patient outcomes and expedite recovery following surgical procedures. This multidisciplinary approach integrates preoperative, intraoperative, and postoperative care strategies.1–3 The ERAS program has been disseminated worldwide and is currently used for orthopedics, gynecology, urology, cardiac surgery, bariatrics, mastology, and colorectal surgery. 4
In the context of colorectal surgery for cancer, the implementation of ERAS protocols is especially significant. Colorectal cancer is a highly incident and potentially life-threatening condition, and surgery is the primary curative-intent treatment option. Colorectal cancer surgery is associated with significant physiological stress and a high risk of complications. 5 However, traditional perioperative care practices, characterized by prolonged fasting, liberal fluid administration, and opioid-based pain management, can contribute to increased complications, delayed recovery, and prolonged hospital stays. ERAS protocols challenge conventional practices by emphasizing a multimodal and evidence-based approach that aims to maintain physiological function, minimize surgical stress, and promote early recovery.6–12
While ERAS has been widely adopted and proven effective in various surgical specialties, achieving perfect compliance with ERAS protocols can be challenging and may vary for each patient. Despite efforts to standardize care, individual patient factors can impact the degree of adherence to ERAS guidelines. 14 Besides, it is still not certain the relative benefit of each specific item proposed in an ERAS protocol. 15 Therefore, understanding the impact of ERAS compliance on patient outcomes is crucial.
This study aims to assess the impact of ERAS compliance and to identify which components of this protocol are most likely to affect postoperative outcomes in patients undergoing colorectal cancer surgery.
Methods
Study design and ethics
A retrospective observational study was conducted at Vila Santa Catarina Hospital (Sociedade Beneficente Israelita Brasileira Albert Einstein) in Sao Paulo, Brazil. This study adhered to the Strengthening the Reporting of Observational Studies checklist guidelines. 16
Ethical approval for the study was obtained from the Institutional Review Board at Hospital Israelita Albert Einstein (CAAE #58157921.3.0000.0071). Given the retrospective design of the study, an exemption of informed consent was requested and approved.
Patient selection
This study included patients diagnosed with colorectal adenocarcinoma who were submitted to elective colon and/or rectum resection and were managed under the ERAS protocol between 2015 and 2022. Local resection, urgent surgeries, and multivisceral resection were excluded from the analysis.
The ERAS protocol
The ERAS protocol encompassed several components, including minimally invasive surgery, optimized preoperative management (prehabilitation), nutritional support, preadmission counseling, iron replacement for iron deficiency anemia, reduced fasting duration, selective mechanical bowel preparation, no premedication, antibiotic prophylaxis, thromboprophylaxis, avoidance of prophylactic drains, prevention of postoperative nausea and vomiting (PONV), use of short-acting anesthetic agents, multimodal anesthesia, maintenance of normothermia, avoidance of fluid overload, minimal use of opioids, avoidance of prophylactic nasogastric tube, avoidance of salt and water overload, avoidance of excess postoperative weight gain, postoperative nutritional support, stimulation of gut motility, early oral nutrition, early mobilization, and early removal of the urinary catheter. The global compliance with the ERAS protocol was assessed as the percentage of items adhered to by each patient. The definitions for adherence to qualitative and quantitative variables are presented in Table 1.
ERAS Components and Definitions of Compliance
BMI, body mass index; ERAS, Enhanced Recovery After Surgery; PONV, postoperative nausea and vomiting.
Data collection
Clinical data were obtained from electronic medical records and surgical databases, encompassing patient demographics, comorbidities, preoperative radiotherapy, operative details, postoperative complications, stoma creation, conversion to open surgery, length of hospital stay (LOS), hospital readmissions, and mortality. Data were prospectively inserted into the ERAS Interactive Audit System, an online secure platform developed by the ERAS Society that allows gathering information about perioperative care and patient outcomes. Postoperative complications were categorized according to the Clavien-Dindo17,18 classification, with Clavien-Dindo grade IIIa or higher considered severe. The ERAS compliance was assessed for each preoperative, intraoperative, and postoperative item.
Follow-up and outcomes
Each patient was followed for 30 days postoperatively. The primary outcome measure was the incidence of severe complications. Secondary outcomes included overall complications of LOS, hospital readmission, and 30-day mortality. We also analyzed specific outcomes associated with particular interventions among the ERAS guideline, such as the incidence of ileus with multimodal anesthesia, volume of hydration with subsequent acute kidney injury, and bowel preparation with surgical site infection.
Groups of study
A cutpoint of 75% was utilized to differentiate between satisfactory (≥75%) and unsatisfactory (<75%) compliance levels. These two groups were subsequently compared.
Statistical analysis
Descriptive statistics were employed to summarize patient demographics and clinical characteristics. Continuous variables were presented as means with standard deviations, while categorical variables were expressed as frequencies and percentages. Fisher’s exact test and Student’s t-test were utilized to compare categorical and continuous variables between the two study groups.
Logistic regression analyses were conducted to evaluate the association between ERAS compliance with its individual components and the occurrence of severe postoperative complications, with results expressed as log-odds ratios (ln OR). Adjusted ln ORs were estimated, accounting for potential confounders such as age (>65 versus ≤65 years old), sex (male versus female), obesity (BMI ≥30 kg/m2), diabetes, cardiac disease, pulmonary disease, previous abdominal surgeries, total mesorectal excision, and American Society of Anaesthesiologists (ASA) score.
A receiver operating characteristic (ROC) curve was constructed to assess the predictive ability of ERAS compliance for the absence of severe postoperative complications. Area Under the Curve (AUC) was calculated, and sensitivity, specificity, as well as positive and negative likelihood ratios for each cutpoint were determined.
All analyses were performed using STATA 18 software Standard Edition (StataCorp, Texas, USA), with statistical significance set at P < .05.
Results
Patients characteristics
The study evaluated 410 patients diagnosed with colorectal adenocarcinoma who underwent elective colorectal resection with perioperative care based on the ERAS protocol between 2015 and 2022 at Vila Santa Catarina Hospital. The overall compliance with ERAS was assessed, with 242 patients (59%) achieving a compliance level of ≥75%. The patient selection flow diagram is presented in Figure 1.

Patients included in the final analysis.
Characteristics of patients with severe postoperative complications
Patients who experienced ≥1 severe complication accounted for 14% (58/410) of the cohort. The most common severe complications included anastomotic leak (4.63%), intra-abdominal collection (1.95%), and obstruction (1.46%). See Table 2.
Types of Complications That Patients with Severe Postoperative Complications (Clavien-Dindo ≥ IIIa) Experienced
Some patients experienced more than one significant complication.
Comparison between patients with <75% and ≥75% compliance with ERAS
No significant differences were observed between patients with <75% and ≥75% compliance in terms of age, sex, obesity, previous surgeries, ASA score, readmission, and 30-day mortality. There were significant differences in the incidence of overall complications (39.9% versus 25.6%; P = .002), severe complications (20.8% versus 9.5%; P = .001), LOS (6.06 days versus 3.96 days; P < .001; Fig. 2), and total mesorectal excision (38.4% versus 61.5%; P = .005). Demographics are summarized in Table 3.
Box plot comparing the length of hospital stay in groups of patients with <70% and ≥70% compliance with ERAS. ERAS, Enhanced Recovery After Surgery.
Comparisons Between Groups with Considered Satisfactory (≥75%) and Unsatisfactory (<75%) Compliance Levels
P values highlighted in bold represent significant values (P < .05).
ASA, American Society of Anesthesiologists; BMI, body mass index; ERAS, Enhanced Recovery After Surgery; LOS, length of hospital stays.
Predicting severe complications according to ERAS compliance
A high ERAS compliance score was associated with an overall reduced risk of severe complications, even after adjusting for multiple confounders (adjusted OR 0.49, 95% confidence interval [CI]: 0.31–0.76, P = .002).
An ROC curve was constructed to assess the predictive ability of ERAS compliance for the absence of severe postoperative complications, with an AUC of 0.677 (95% CI: 0.602–0.752; see Fig. 3). Sensitivity, specificity, and positive and negative likelihood ratios were calculated for different cutpoints. For the cutpoint 70%, the sensitivity, specificity, and positive (LR+) and negative (LR−) likelihood ratios were 81.43%, 43.33%, 1.437, and 0.429, respectively. See Table 4.

ROC curve for global compliance to ERAS for predicting the absence of severe postoperative complications. ERAS, Enhanced Recovery After Surgery; ROC, receiver operating characteristic.
The Sensitivity, Specificity, and Positive (LR+) and Negative (LR−) Likelihood Ratios Were Estimated Based on Different Cutpoints for Global ERAS Compliance, for Predicting the Absence of Severe Postoperative Complications (Clavien-Dindo ≥ IIIa)
ERAS, Enhanced Recovery After Surgery.
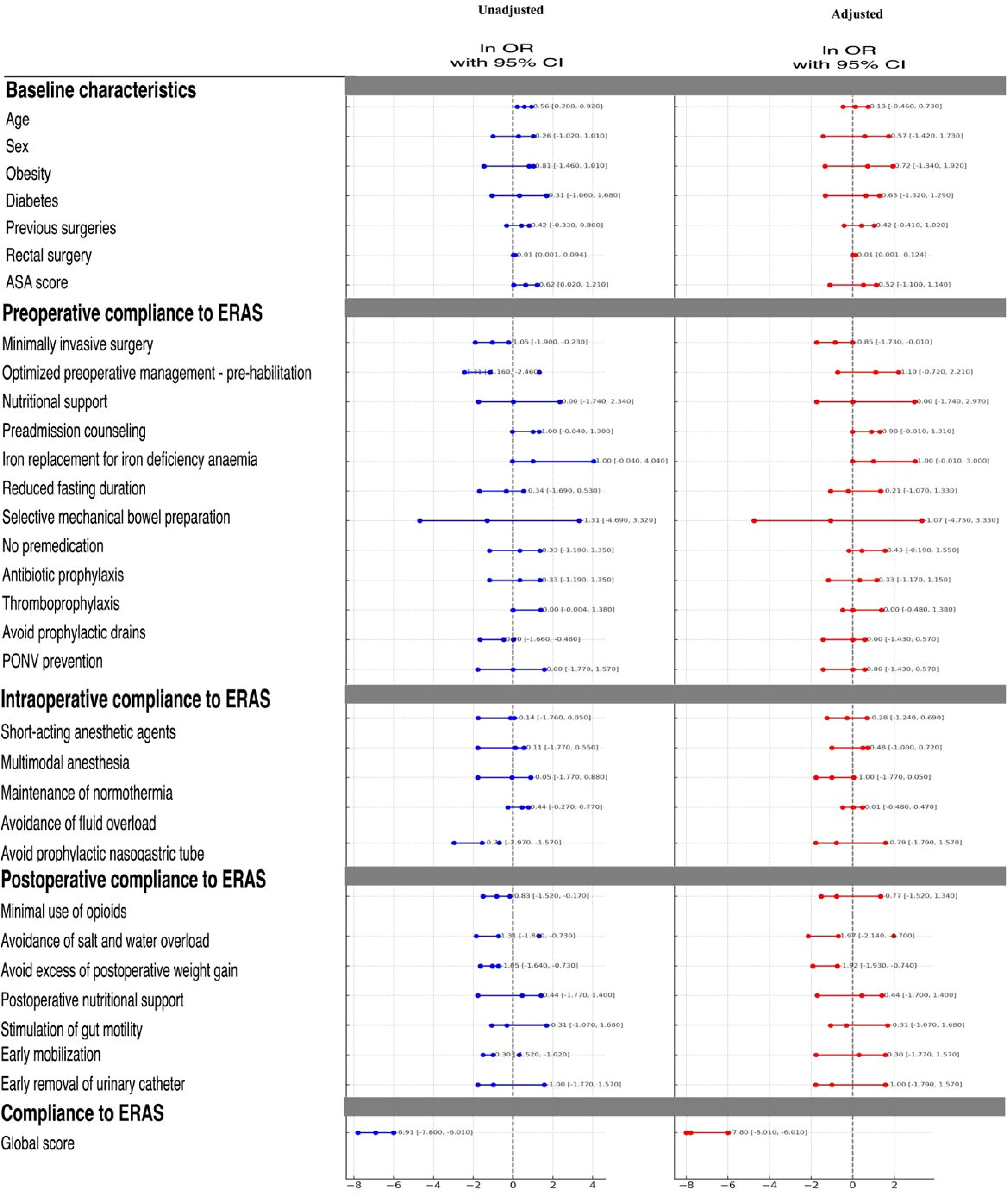
Logistic regression analyses were estimated based on unadjusted and adjusted ln OR. The ERAS items were adjusted for potential confounders such as age (>65 versus ≤65 years old), sex (male versus female), obesity (BMI ≥30 kg/m2), diabetes, previous abdominal surgeries, total mesolectal excision, and ASA score. For the adjusted ln OR, male sex (P = .018), diabetes (P = .036), rectal surgery (P < .01), compliance to pre-habilitation (P = .023), avoiding prophylactic drains (P < .001), minimal use of intraoperative opioids (P = .045), avoidance of postoperative salt and water overload (P < .001), postoperative nutritional support (P = .048), and early mobilization (P = .025) influenced the risk for postoperative severe complications. The global compliance with ERAS, as well as particular interventions, were impactful in predicting severe complications as demonstrated in Figure 4.

Logistic regression analyses were estimated based on unadjusted and adjusted log-odds ratio (ln OR).
Particular interventions included in ERAS
To further analyze the impact of individual interventions among ERAS, we analyzed the effect of particular interventions. Multimodal anesthesia was not associated with a reduced incidence of postoperative ileus (adjusted OR 1.03, 95% CI: 0.43–2.49, P = .935). Similarly, we did not find any association between bowel preparation and surgical site infection (adjusted OR 1.01, 95% CI: 0.51–6.12, P = .93). Of note, avoidance of fluid overload was significantly associated with a reduced incidence of acute kidney injury (adjusted OR 0.36, 95% CI: 0.13–0.98, P = .046).
Discussion
The findings of this study suggest that high compliance with ERAS protocols is associated with significantly lower overall complications and severe complications (Clavien-Dindo ≥ IIIa). These results underscore the importance of adhering to ERAS principles in colorectal cancer surgery to improve patient outcomes and expedite recovery. The novelty of our study is to show that an overall high compliance with ERAS protocols has a synergic effect to reduce overall complications when compared with the effect of each isolated intervention with expected improved outcomes.
The benefits of the ERAS programs are well established in the literature. The 2019 POWER Study demonstrated that individual adherence to ERAS interventions is associated with improved outcomes, even in centers without established protocolized care. 19 A Cochrane meta-analysis of randomized trials has shown an improvement in postoperative recovery of patients submitted to an ERAS care compared with conventional care, with a reduction in postoperative complications and LOS. 20 Our study suggests that outcomes are intimately related to high global adherence to the protocol. Other studies resulted in a similar association.21,22
Despite being essential for better outcomes, adherence to the protocol, especially to postoperative interventions, is challenging.13,21,23 This complexity can be explained by several reasons, such as the demand for close alignment between the multitude of specialties involved in postoperative care. Furthermore, the struggle to implement certain ERAS components can be associated with behaviors that are hard to change due to challenging traditional practices, such as early feeding, early removal of the urinary catheter, and the use of nonsteroidal anti-inflammatories. Consequently, the number of implemented items of the protocol included in previously published studies is not standardized. Guidelines for Perioperative Care in Elective Colonic and Rectal Surgery ERAS Society recommendations describe a 24 items protocol for colorectal surgery. 24 In our study, we included 22 of the ERAS elements, above the average number of items applied in most previously published studies. 25
In this sense, the necessity of compliance with all elements proposed in ERAS guidelines is still widely discussed. If the number of essential items in the protocol was reduced or only those with the most significant impact on outcomes were selected, it would be easier to apply it. More centers could adhere to the recommendations, with less need for changes in local habits. The Remove, Ambulate, Postoperative Analgesia, Introduce Diet protocol adopted a modified, enhanced recovery program with only four interventions. This adapted protocol resulted in a shortened LOS in open and laparoscopic colorectal resection. 26 As the enhanced recovery understanding develops, certain interventions may be nonessential.
Our study’s key protocol components for preventing severe complications (Clavien-Dindo ≥ IIIa) include avoiding prophylactic drains, minimal postoperative opioid use, avoiding salt and water overload, nutritional support, and early mobilization.
Regarding prehabilitation, in the present article, it was defined as the cessation of smoking and drinking at least 4 weeks before surgery, and it was associated with an increase in the complication rate. However, the benefits of cessation of smoking and drinking are well established in the literature. Surgical patients who are smokers have a higher risk for wound infections than nonsmokers. 27 The wound infection rate in smokers is 12% compared with 2% in nonsmokers (P < .05), and after 4 weeks, the rate is 1% in abstinent smokers (P < .05) when compared with smokers. 28 Smoking cessation restores the tissue microenvironment and inflammatory cellular functions. 29 A Cochrane meta-analysis showed that alcohol cessation lowers postoperative complication rates (OR = 0.22; P = .004). 30 Nevertheless, prehabilitation extends beyond merely stopping smoking or drinking. It entails a multimodal approach involving nutritional intervention, physical exercise, and psychological support. Therefore, more comprehensive prehabilitation programs than ours could potentially improve postoperative outcomes. A recently published randomized trial found that the rate of severe complications was significantly lower in patients submitted to prehabilitation when compared with the conventional approach (OR = 0.47; P = .02). 31 Despite our study isolating nutritional interventions from smoking and drinking cessation, it is evident that this specific component plays a crucial role in affecting morbidity.
In the current study, avoiding postoperative drainage has decreased the risk of postoperative severe complications. Drainage of the abdominal cavity is utilized to treat anastomotic leaks.32–34 However, the prophylactic use of drains is controversial since it has been shown to increase the incidence of infection, delay healing, and increase morbidity.35–38 Drains could stimulate fluid collection by causing a foreign-body reaction and hampering the dead space’s closure.39,40 Besides, prophylactic drains frequently fail to remove fluids when a leak is present. 41 Furthermore, drains are a discomfort to the patient and could impact recovery by several other factors such as increasing pain and restricting mobilization. Nevertheless, its use in extra-peritoneal resections is still defended since the incidence of anastomotic leak is higher.42–46 However, two recent meta-analyses found no significant difference in routine and prophylactic use of drains.47–49 It is important to consider the potential relationship between the use of drains and the development of complications in patients who may already be at a higher risk. Determining causality in an observational study design can be challenging, and a clearer understanding of this issue may only emerge from future trials.
Surgical stress and pain impair the functioning of the immune system, especially affecting the natural killers and cytotoxic T cells.50,51 This could increase the chance of cancerous cells scaping our immune defenses. Furthermore, opioids also facilitate cancer cell proliferation by inhibiting cellular and humoral immunity and increasing angiogenesis and migration.52,53 Epidural anesthesia has been shown to reduce the immunosuppressive effects of surgery and is associated with a lower recurrence of cancer after oncologic surgery for breast, prostate, and malignant melanoma.54–59 In colorectal cancer surgery, the use of peridural anesthesia results in an increase in a 5-year survival rate (62% versus 54%), especially in patients with worse health status. 60 This may be attributed to these patients’ more impaired immune system, resulting in a more important peridural effect in reducing the immunosuppressive effects of surgical stress.
In our study, the use of multimodal anesthesia and short-acting agents during surgery was not significantly associated with a reduced risk of postoperative complications. However, the minimal use of opioids postoperatively did show a risk reduction. A recent study found that patients submitted to opioid-free anesthesia had lower pain score in the first 72 hours after open colorectal surgery and less need for rescue analgesia postoperatively in comparison with opioid-based and low-opioid anesthesia. 61 The “opioid paradox” suggests that the more use of opioids, the less resistance to pain the patient develops, and even more opioids are needed.62,63 Thus, the use of multimodal anesthesia and short-acting agents, even though not significantly associated with a reduced risk of complications, could have led to a decreased use of opioids postoperatively, which in turn resulted in a decrease in complications.
Opioid use significantly increases the risk of PONV and other adverse effects, such as postoperative ileus, urinary retention, shivering, respiratory depression, sleep-disordered breathing, and delirium.64–70 Interestingly, our study did not find any evidence of reduced ileus with this anesthetic approach. Evidence from the Lancet Global Commission has highlighted the significant gap in access to safe and affordable anesthesia between high-income and low/middle-income countries. 71 A meta-analysis showed that the use of transverse abdominis plane blocks, spinal anesthesia, and epidural blockade were some of the intraoperative ERAS components more prevalent in cohorts from high than low/middle-income countries. 72 Those items also often come with a greater cost and burden on hospital resources and could have influenced the adherence to multimodal anesthesia in our study.73–75
Avoiding volume overload has been shown to reduce postoperative complications in multiple studies.76–79 However, there is a wide range of variation between definitions, and a standardized target is yet to be defined. Other studies have different definitions of compliance for this item.25,80 Similar to Gustafsson et al., 81 our study considers balanced fluid therapy when the sum of intravenous fluids administered intraoperatively and in the first 24 hours do not exceed 3000 mL in colonic resection and 3500 mL in rectal. Our study demonstrated that avoiding salt and water overload is associated with a decline in postoperative morbidity. Excessive volume infusion can lead to organ dysfunctions such as cardiopulmonary failure, increased renal function, delayed anastomotic healing due to poor tissue oxygenation, haemodilution, and increased thrombosis risk. 82 However, a too-severe fluid restriction can impair organ perfusion and tissue homeostasis. 83 Thus, a euvolemic state is the goal to be pursued.84–88 Our results point to a significant reduction in acute kidney injury with avoidance of fluid overload.
Oral supplementation in the preoperative period is recommended to support the synthesis of acute phase protein, immune cells, and wound healing. 89 Malnutrition is an independent risk factor for infectious complications, mortality, LOS, and costs in surgical patients. 90 To reduce insulin resistance and increase glycogen reserves before surgery, regardless of nutritional status, it is recommended to administer oral carbohydrate drinks before surgery.91,92 Although it is likely to help the patient withstand the surgical insult, a Cochrane Review found that carbohydrate loading for elective surgical patients was associated with a small decrease in LOS in comparison to placebo or fasting (reduction risk by 0.30 days; 95% CI: 0.56–0.04) and did not have an impact on morbidity (RR = 0.98; 95% CI: 0.86–1.11). 93 Similarly, in the current study, carbohydrate treatment was not significantly associated with a decrease in complications. Future trials should address different oral drinks for reduced fasting. A mixture of carbohydrates and amino acids has been shown to increase insulin concentration and anabolic effects.94–96
In the postoperative period, early feeding is recommended to stimulate gut motility, immune response, and anabolism.87–101 A randomized trial found that oral nutritional supplements administered after surgery (15% versus 34%; P < .05) or both in the pre and postoperative periods (15% versus 34%; P < .05) resulted in a significant reduction in complications. 102 The mean intake of oral nutritional supplements in the inpatient phase in the former was 258 kcal/day, and in the latter was 300 kcal/day. Our study used the cutpoint of more than 300 kcal of nutritional supplements on the day of surgery. Although early feeding didn’t significantly impact complication rates, the use of postoperative nutritional supplements significantly resulted in less morbidity. Postoperative nutritional care was also an intervention more commonly reported in high-income countries (OR = 2.36; 95% CI: 2.18–2.56). 72 An evaluation of each component’s cost and impact on the service budget could be proposed in subsequential studies. This better nutritional load may be a possible explanation for the observed benefit in anatomical leak incidence.
Catabolism is further exacerbated by long-term bed rest.103–106 Early mobilization is associated with better gastrointestinal function and improved body composition.107,108 A meta-analysis found that early mobilization correlates to a faster clinical gastrointestinal recovery, defined as the passage of the first flatus or bowel movements (mean difference: −11.53 hours; P = .03). 109 Prolonged bed rest is associated with a risk of developing pulmonary complications, decreased skeletal muscle strength, thromboembolic complications, and insulin resistance.110–112 In our study, early mobilization was associated with a reduction in morbidity. Early mobilization is relatively inexpensive and can be easily implemented in high- and low/middle-income countries.113–116
Furthermore, there are reasons to believe that some components of the ERAS program work synergistically.117,118 The overall cooperation in a multidisciplinary team ensures each recommendation is performed while managing to secure the success of the global pathway. This team effort may increase compliance and explain why adherence to the entire protocol increases the likelihood of enhanced recovery for the surgical patient. Finally, the relationship between complications and compliance to an ERAS pathway seems more complex than the general cause-and-effect association of poor compliance causing poor outcomes. 119
Choosing a cutpoint for ERAS compliance is a critical consideration in assessing its impact on postoperative outcomes. While many studies, including ours, use a cutpoint of 75%, the selection of this threshold is not universally defined.14,18,19,23,25,81 The lack of a standardized target compliance value leads to different study methods that could influence results. However, the appropriateness of a cutpoint depends on the primary goals of the evaluation. Scores with high sensitivity and negative predictive values are typically used as screening tools. In contrast, scores with high specificity, positive predictive values, and post-test probability are employed to provide greater certainty in outcome prediction. 120 In our study, by adopting higher cutpoints for ERAS compliance, the natural tendency is to increase specificity and LR+ to predict the absence of severe complications, and the highest LR+ value is found in a threshold of 85% compliance. Since the goal of our study is to predict the occurrence of severe complications in patients submitted to the ERAS protocol, ideally, a more specific cutpoint should be determined. Thus, if we had been more rigorous with the cutpoint, e.g., around 80%–85%, a more important impact in severe complications would be observed.
The strengths of the present study include the close follow-up on well-characterized consecutive patients, with full adherence data recorded in a well-defined ERAS protocol. Limitations of our study include its single-center design, which may limit the generalizability of the findings. Statistical analyses were made adjusting for covariates that could influence outcomes to mitigate its effects and isolate the ERAS components’ impact on said outcomes. However, due to the retrospective and observational nature of the study, not all potential confounding factors can be addressed. Also, it is important to highlight that the negative associations could also result from a type II error, which occurs when the statistical analysis cannot reject a false hypothesis. Also, the institutional protocol only included mechanical and antibiotic bowel preparation in total mesorectal excision cases, which may have altered the observed benefits of this approach regarding surgical site infection incidence. Furthermore, we only assessed perioperative outcomes, and there is still a need to understand better the impact of the ERAS program on long-term survival analysis. Future studies should aim to validate our findings in larger, multicenter cohorts and consider other factors, such as patient-reported outcomes and long-term follow-up, to provide a more comprehensive assessment of ERAS compliance and its impact on colorectal cancer surgery outcomes.
Conclusion
High ERAS compliance is associated with improved postoperative outcomes in colorectal cancer surgery. Key protocol components for preventing severe complications include avoiding prophylactic drains, minimal postoperative opioid use, avoiding salt and water overload, nutritional support, and early mobilization.
Footnotes
Authors' Contributions
Conceptualization: A.S.P., M.L.V.O., F.T., and S.E.A.A. Statistical Aanalysis: F.T. and R.M.A.L. Writing of manuscript: A.S.P., M.A.V.O., R.M.A.L., F.T., V.E.S., L.S.G., R.V.P., and S.E.A.A.
Availability of Data and Materials
Data supporting the findings of this study are available from the corresponding author upon request.
Ethical Approval and Consent to Participate
Ethical approval for the study was obtained from the Institutional Review Board at Hospital Israelita Albert Einstein (Protocol Number: CAAE #58157921.3.0000.0071), and all patients provided informed consent.
Disclosure Statement
No competing financial interests exist.
Funding Information
The study was not funded.