
Abstract
Background:
Gastrointestinal (GI) perforation in the neonatal period can result from different conditions with varying degrees of severity. Optimal timing for surgery is challenging to establish and laparoscopy has been proposed as a diagnostic tool to minimize surgical delays and refine surgical indications. However, no standard animal model is universally accepted for training laparoscopic management of neonatal GI perforations. We aimed to define a small-sized animal model and (1) assess the effectiveness of laparoscopy in identifying GI perforations and (2) evaluate the viability of intracorporeal suturing, in a confined working space.
Methods:
In total, 30 Sprague Dawley rats underwent laparoscopy. In Part I, a random GI perforation was performed. In Part II, the perforation was identified and sutured. The surgeon of Part II remained blinded during Part I. The suture line was assessed for leaks and strictures once the rats were euthanized.
Results:
In Part I, 29 perforations were created: 22 in the ileum, 3 in the colon, 2 in the jejunum, 1 in the stomach, and 1 in the duodenum. In one rat, the GI tract was left intact. In Part II, all 29 perforations were identified and sutured. The average duration of Part II was 53 ± 16 minutes. During suture evaluation, a leak was observed in two cases, and a stricture in two additional cases.
Conclusions:
Laparoscopy was technically feasible and highly sensitive in detecting isolated GI perforation in a rat model. This model holds particular value for training laparoscopic skills in a space-limited setting. Further investigation is needed to see if a learning curve can be achieved.
Introduction
Neonatal pneumoperitoneum typically originates from a gastrointestinal (GI) perforation and is considered a critical condition. Necrotizing enterocolitis (NEC) is commonly implicated as the leading etiological factor. 1 However, recent data revealed that around 50% of pneumoperitoneum cases in neonates are not associated with NEC.2,3A variety of other conditions can also lead to GI tract perforation in neonates, including spontaneous intestinal perforation (SIP), among others. Interestingly, pneumoperitoneum may also occur without any identifiable intestinal perforation, often resulting in unnecessary laparotomy in many instances.2,4–7
The decision to perform surgery on critically ill neonates should be backed by strong surgical evidence, as both delayed diagnosis and unnecessary laparotomy can lead to devastating outcomes. Minimally invasive surgery in infants and neonates has gained considerable attention over the past decade, facilitating decision-making while minimizing surgical trauma.
The role of laparoscopy in the management of NEC has been extensively researched and proven to be a safe clinical procedure that may avoid the need for urgent laparotomy. In instances where laparotomy is considered imperative, laparoscopy can precisely locate the perforation site, thereby guiding and limiting the extent of laparotomy.8–12 Laparoscopy has also proved to be useful in the diagnosis of various other conditions.13–16 In fact, Burgmeier et al. demonstrated that subsequent laparotomy could be avoided in 53% of neonates with acute abdominal conditions who initially underwent laparoscopy. 17
Despite all encouraging findings, the use of laparoscopy in these clinical scenarios demands high technical expertise given the small dimensions and fragile physiological state of neonates. To our knowledge, there are no previous studies that have focused exclusively on laparoscopic diagnosis and treatment of neonatal GI perforations. The possibility to perform a minimally invasive and definitive treatment could be highly advantageous in the management of these infants.
Thus, our study aimed to (1) establish a small-sized animal model to evaluate the efficacy of laparoscopy in exploring the GI tract and localize a perforation and (2) assess the feasibility of intracorporeal suturing in an in vivo model, simulating the specific technical challenges encountered in neonatal laparoscopy.
Materials/Methods
This study was conducted at the Endoscopic Laboratory of the Life and Health Sciences Research Institute (ICVS), in Braga, Portugal. Ethical approval was granted by the National Authority for Animal Protection (Direção Geral de Alimentação e Veterinária–DGAV 013778) in September 2022, in compliance with Directive 2010/63/EU of the European Parliament.
The study involved 30 Sprague Dawley rats. Surgical procedures were carried out by a team of one pediatric surgeon and two senior residents, with basic experience in human laparoscopy. Each member underwent a specific dry lab training for this exercise. All animals were euthanized postsurgery.
Experimental design
The surgical procedure was divided into two parts. Part I entailed trocar placement and the creation of a random small single perforation in the GI tract. Not creating a perforation was also an option, to simulate idiopathic pneumoperitoneum. In Part II, exploratory laparoscopy was conducted to identify the perforation (if present) and to close it using intracorporeal suturing.
All three surgeons were assigned a specific role in the procedure: surgeon in Part I, surgeon in Part II, or as a camera assistant in both parts. The surgeon of Part II was not present during Part I to remain unaware of the perforation’s location and to ensure a blinded procedure.
An exploratory laparotomy was performed in posteuthanasia to assess the suture line.
Anesthetic technique
The rats were anesthetized intraperitoneally with ketamine 75 mg/kg (Ketamidor, Richter Pharma AG, Wels, Austria), medetomidine 0.5 mg/kg (Sededorm, Vetpharma Animal Health SL, Barcelona, Spain), and buprenorphine 0.05 mg/kg (Bupaq, Richter Pharma AG, Wels, Austria). The animals underwent tracheostomy and were ventilated. Euthanasia was executed using an intracardiac injection of phentobarbital 200 mg/kg (Euthasol, Le Vet B.V., Oudewater, Netherlands).
Operative technique
Part I
The animals were placed in a neutral supine position and secured with tapes (Fig. 1). The abdominal region was shaved. An optical port was inserted in the left upper quadrant using the Hasson technique and secured with a cerclage (Fig. 2). A 5 mm Karl-Storz Rotalock® was initially used in the first 10 surgeries, followed by a standard 5 mm metal sheath trocar in the subsequent 20 surgeries. The pneumoperitoneum was maintained at a pressure of 3 mmHg, with a flow rate of 0.7 L/min. A 30-degree 5 mm telescope was introduced into the peritoneal cavity. Two additional trocars (3.5 mm Karl-Storz Rotalock®) were inserted in the left flank and right hypochondrium (Fig. 2). The surgeon of Part I randomly selected a location to create a perforation using a 3 mm atraumatic grasper and a 3 mm Metzenbaum scissors, ensuring the perforation did not exceed 1 cm (Fig. 3).

Anesthetized and positioned rat. After anesthesia, the rats were secured with adhesive tape to maintain the right positioning throughout the procedure.

Placement of trocars. To ensure maximum visualization of the GI tract, the optical port was placed in the left upper quadrant, and the two working ports in the right hypochondrium and left flank. GI, gastrointestinal.
Part I: Creation of the perforation.
Part II
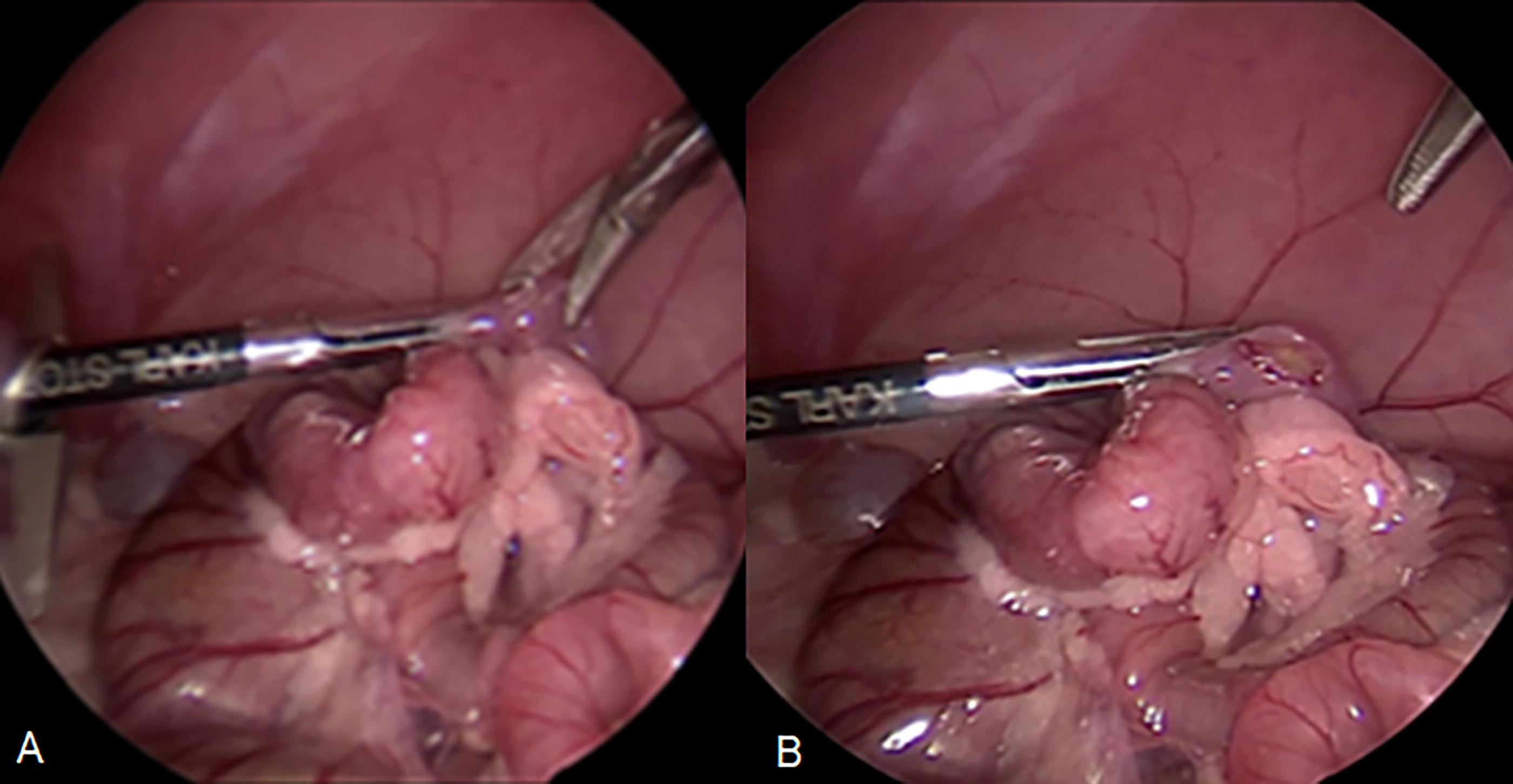
Pat II commenced 15 minutes after Part I. The entire length of the GI tract was inspected. Identified perforations were sutured using interrupted stitches (Fig. 4). Vicryl, Ethicon® 5/0 RB-1 PLUS, was used in the first 10 surgeries, and PDS Ethicon® II 5/0 RB-2, was used in the following 20 surgeries.

Part II: Laparoscopic finding and suturing of the perforation. Final aspect of a perforation closed with interrupted stitches.
Evaluation of the suture
A postmortem exploratory laparotomy was conducted for anastomosis quality assessment. Clamping was done proximal and distal to the suture line, and methylene blue was injected proximal to the anastomosis using a 22G needle until the dye reached the distal part. The presence of leaks or strictures was observed.
Data collection
Prior to surgery, the rats’ weight and abdominal perimeter (at the central point of the xipho-pubic line) were measured. Data collected in Part I included abdominal perimeter postpneumoperitoneum, difficulties encountered in trocar placement, and the location of the perforation (if created). Data collected in Part II included the identification of the perforated site, suturing challenges, and the number of stitches used. The duration of part II was also recorded. Any observed leakage or strictures were reported, during the final suture evaluation.
Results
A total of 30 surgeries were conducted on 30 rats in this current study. The majority were female (86.7%), with an average weight of 283 ± 66.9 g. The preoperative mean abdominal circumference was 17.4 ± 1.7 cm, which increased to 19 ± 1.8 cm postpneumoperitoneum.
Each team member rotated roles and performed 10 times as the surgeon for Part I, 10 times as the surgeon for Part II, and 10 times as the camera assistant. The roles were randomly assigned to the participating surgeons for each procedure.
Thirty procedures were conducted in part I: a perforation was created in 29 rats, and no perforation was made in one rat. Perforations were mostly located in the ileum (22), followed by the colon (3), jejunum (2), stomach (1), and duodenum (1).
During Part II, all 29 perforations were successfully identified, and the entire GI tract was thoroughly examined in the nonperforated rat. Laparoscopic suturing of all perforations was completed. The average duration of Part II, including laparoscopic inspection and suturing, was 53 ± 16 minutes. The average time taken for suturing was 37 ± 14 minutes. The average number of interrupted stitches per suture was 2.5 (range 1–7), which varied according to the size of the perforation and the surgeon’s assessment. Table 1 exhibits the average time of suturing (time per stitch) and shows differences between the initial and last cases performed, by surgeon. The average time per stitch was slightly inferior in the last cases performed, but no statistical differences were found.
Average Time Per Stitch: Differences Between Initial and Last Cases Performed, by Surgeon
Table 1 shows mean time spent for suturing, by surgeon. Differences between time for suturing during first and last cases performed are displayed. Student t test was used to determine if P value is <.05.
Technical challenges were noted in the first 10 surgeries: the needle size was disproportionate to the bowel and dimensions of the GI perforations, and the blind intra-abdominal opening of the jaws of the first Rotalock® trocar led to omentum and bowel trapping in two cases. These issues were resolved by switching to a smaller needle (PDS, Ethicon® 5/0 RB-2) and replacing the optical port with a standard 5 mm trocar. Additionally, high flow loss of pneumoperitoneum was observed in one case and was managed by replacing a leaking trocar.
Intraoperative complications included mesenteric tears observed in two cases during bowel manipulation for inspection and accidental enlargement of the perforation site in one case. None of these incidents led to serious complications such as bleeding, perforation, or ischemia.
Suture evaluation was conducted via postmortem laparotomy: A slight suture leakage was observed in two cases following the injection of methylene blue (6.9%). Moderate and severe strictures were present in another two cases (6.9%) and resulted in minor and absent passage of the dye through the suture site. All leaks and strictures occurred in anastomoses located in the small bowel.
Discussion
GI perforations in the pediatric population can occur at any age but are more prevalent in neonates.1,18 These perforations are often found in the small intestine, colon, and stomach, with varying proportions.1,18–20 Identifying the underlying causes of such perforations is crucial in determining both management and prognosis.
NEC and SIP are the most common causes of neonatal GI perforation, and their early differentiation is strongly advocated by the authors of the Necrotizing Enterocolitis Surgery Trial. 21 This distinction significantly impacts treatment approaches. 22 However, without direct bowel visualization, making an accurate differential diagnosis can be challenging.23,24
Laparoscopy has been proposed as a diagnostic and therapeutic tool for neonates with suspected NEC and other acute abdominal conditions.13–17 Knudsen et al. recently proposed laparoscopy as a feasible tool for diagnosing NEC lesions in a porcine model and demonstrated a high positive predictive value. 25 The direct visualization of the GI tract in patients suspected of NEC has also proven to be useful in clinical practice. A review of 44 cases across 7 studies by Smith et al. revealed that direct visualization of the bowel via laparoscopy prevented laparotomy in a fifth of neonates, and in some cases facilitated limited microlaparotomy. 10
Montalva et al. have studied the largest cohort of neonates (N = 48) with suspected NEC undergoing laparoscopy and have revealed an association between early laparoscopy and decreased postoperative C-reactive protein levels (P < .005) and strictures (P = .04). 12 This finding suggests a possible anti-inflammatory effect of carbon dioxide insufflation, a correlation previously reported by other researchers.26–29
Unlike NEC, SIP typically presents as a focal perforation in an otherwise normal-appearing bowel. 30 A limited and precise approach might be beneficial in this condition. Nevertheless, there are no previous studies that have explored laparoscopy as a tool for both diagnosing and treating GI perforations in newborns.
Our team developed a novel animal model to assess the feasibility of laparoscopic diagnosis and management of neonatal GI perforation. The Sprague Dawley rat, though infrequently used as an animal model for laparoscopic skill training,31–34 was chosen for this study. To our knowledge, this is the first study to employ the rat as a training model for neonatal laparoscopic surgery. The rat offers several advantages: it is well-studied, commercially available, inexpensive, and its reduced anatomical scale is analogous to that of premature and low-birth-weight infants, who are commonly at risk for GI perforations. 35 The mean abdominal perimeter of the animals in our study was 17 ± 2 cm, slightly less than the reference value for abdominal circumference in premature newborns (24–30 cm). 36 The rat’s bowel is also narrower than that of premature infants, thus presenting additional challenges beyond those expected in real conditions.
Literature reports a varying pneumoperitoneum pressure from 4 to 15 mmHg in newborns8,9,12 and those in rat models range from 5 to 12 mmHg.31–33 A reduced pneumoperitoneum pressure of 3 mmHg was used in our study, which did not interfere with cardiovascular or ventilatory stability and was suitable for the surgical procedures.
The primary goal of our study was to evaluate the effectiveness of laparoscopic examination of the entire GI tract to detect a GI perforation. The GI tract was fully examined in all 30 rats, despite technical difficulties associated with the model (delicate bowel handling in a confined space). A common concern with minimally invasive procedures in newborns is the risk of false negatives, as the dilated bowel in the small peritoneal cavities may hinder proper visualization. However, other indirect signs, such as peritoneal soiling or fibrin, can be equally informative. A clinical series by Pierro et al. reported only one case (1/11, 9%) where the entire intestine could not be visualized. 9 Montalva et al. noted two cases (2/48, 4%) in which alarming findings were not initially identified at laparoscopy but required reintervention for perforated NEC. 12 It remains unclear whether these perforations were pre-existing or developed subsequently.
The second objective of our study was to assess the feasibility of laparoscopic sutures in a neonatal animal model, a technique not widely recognized. Laparoscopic repair of isolated perforations was achievable in all cases, despite evident spatial constraints. Over 80% of the sutures performed (25/29, 86%) were nonobstructive and continent. The four cases presenting with anastomotic stricture or leakage highlight the challenges of achieving optimal suturing and emphasize the need for a structured training plan. Further studies are needed to determine if a learning curve can be established using our training model, to efficiently assist surgeons in developing these specific laparoscopic skills.
We recognize the need for careful selection criteria before recommending exploratory laparoscopy to investigate pneumoperitoneum in small infants. We believe that incorporating this approach into management algorithms for neonatal pneumoperitoneum could be particularly beneficial; it may potentially reduce the common delay in diagnosis seen in these cases, 37 which is a significant factor linked to prognosis and mortality. 38 However, additional studies are needed to confirm the feasibility and safety of performing laparoscopy in neonates, to establish appropriate indications and optimize its application.
We acknowledge the limitations of this study, including anatomical and physiological differences between the model used and human neonates, which affects extrapolation to clinical practice. Additionally, intestinal perforation was created soon before diagnostic laparoscopy (Part II was performed 15 minutes after Part I, under the same anesthesia), which is normally not the case in real-life settings. Evidence of contamination, omentum adherence, and ischemia are findings that may occur over time, potentially complicating or facilitating the localization of the perforation, and these factors were not addressed in our study design.
Future steps to improve our model should include replicating physiological derangements and widespread abdominal inflammation associated with intestinal perforation. The model’s effectiveness for more complex hollow–visceral interventions such as resection and anastomosis should also be evaluated, as it may serve as a potential valuable tool for training advanced laparoscopic skills in pediatric surgery.
Conclusions
Our study demonstrates that laparoscopy is a technically feasible and highly sensitive procedure in detecting isolated GI perforation in a small infant animal model. Laparoscopic suturing of GI perforation in rats, though highly challenging, is suitable for training in limited space conditions. The rat model is an adequate and affordable training method for this surgical approach.
Footnotes
Acknowledgments
The authors would like to thank Karl Storz GmbH for technical support and equipment. The authors would like to acknowledge the collaboration of Doctor Inês Braga and Doctor Sofia Martinho for their precious and insightful feedback, contributing to the successful planning and execution of the procedures. The authors extend their gratitude to Doctor Kinga Sandor-Bajusz for her contribution in meticulously reviewing this article for grammatical accuracy and readability.
Authors’ Contributions
Each author has participated in this work and takes public responsibility for all contents. V.L.M.: Investigation, technical procedures, data interpretation, and drafting of the article. E.S.: Investigation, technical procedures, data interpretation, and drafting of the article. E.V.Q.: Investigation, technical procedures, data interpretation, and drafting of the article. A.M.: Technical procedures, operationalization, and drafting of the article. P.E.: Operationalization, data interpretation, reviewing and editing, project administration, critical revision, and supervision. J.C.-P.: Operationalization, data interpretation, reviewing and editing, project administration, critical revision, and supervision.
Disclosure Statement
The authors have no conflict of interests to disclose.
Funding Information
The authors declare that no funds, grants, or other support were received during the preparation of this article.