
Abstract
Background:
Laparo-endoscopic hernia surgery is recommended by various international bodies. However, its uptake by general surgeon is low. We aim to assess the impact of Three Dimensional (3D) endovision system in learning laparoscopic transabdominal preperitoneal (TAPP) repair of groin hernia and transferability of skills acquired from 3D to the Two Dimensional (2D) environment.
Methodology:
Senior resident doctor with no previous experience in laparoscopic hernia surgery did 20 consecutive cases of TAPP repair using 3D endovision system followed by another five cases of TAPP repair using 2D endovision system. Total operating time, operating time during different phases of hernia surgery, faculty take over time, path length of needle holder, and scissors were recorded. Cumulative sum (CUSUM) and split group analysis were done to assess the learning process. Trainee’s operating time was compared with that of experts’ from previously published study of the same group. Data were compared between last block of five cases done using 3D system and cases done using 2D system for skill transferability.
Results:
CUSUM method provided inflection points of total operating time, hernia dissection and mesh placement at 9th case, and peritoneal suturing at 11th case in learning TAPP hernia. After 10th case, trainee’s operating time was within the middle 50 percentage of experts operating time. Total operating time in last block of cases done under 3D vision and that of 2D endovision comparable, although peritoneal closure was significantly longer in 2D vision (P = .074, .2, .145, .001).
Conclusion:
Reduction on operating time appears after ninth case of TAPP hernia repair using the 3D endovision system. The skills acquired under 3D endovision system are transferable to perform the procedure under 2D endovision system, albeit incompletely. Use of 3D technology may facilitate adaptation of TAPP hernia repair by young surgeons.
Introduction
Inguinal hernia surgeries are one of the most frequently performed surgical procedures globally. There are diverse described techniques in the treatment of groin hernia, necessitating global guidelines and recommendations favoring one technique over other. Laparo-endoscopic repair has been found to have lower incidence of wound infections, hematoma formation, nerve injury, chronic pain syndrome, and it allows an early return to normal activities. Presently, it is the recommended approach for groin hernia repair, provided that necessary expertise is available.1–3 However, the surgeons’ adoption of minimally invasive techniques in hernia repair has been poor. 4 Most commonly reported drawbacks of laparo-endoscopic repairs were difficult and unfamiliar anatomy, lack of expert guidance, concerns of patient safety, long learning curve, and loss of depth perception. 5
Traditional laparoscopic systems have 2D display, which limits surgeon’s depth perception. The introduction of 3D endovision systems has mitigated this age-old concern of laparoscopy and was found to enable faster skill acquisition, reduction in operating time, and complications.6–11 A 3D laparoscopy was associated with significant reduction in operating time, without compromising patient safety and long-term outcomes of laparoscopic transabdominal preperitoneal (TAPP) repair. 12 However, whether use of 3D technology will hasten learning process of TAPP hernia repair and thereby facilitate adoption of laparo-endoscopic hernia repair was never evaluated.
We hypothesized that the use of 3D systems may expedite the learning process of the surgeon and may help to acquire the necessary technical skills for laparoscopic inguinal hernia repair. This study was designed to evaluate the learning process of laparoscopic TAPP repair using 3D endovision system and to evaluate whether skills acquired using 3D endovision system are transferable to perform hernia surgery using 2D endovision system.
Materials and Methods
This prospective observational study was performed at a tertiary care teaching hospital during the period between September 2022 and March 2023. A senior surgical resident at fourth to fifth year of surgical residency training was the operating surgeon. At the initiation of the study, he had no experience of laparoscopic inguinal hernia repair, however, he was assisting various laparoscopic procedures and had experience of performing six cases of laparoscopic cholecystectomy. Before starting the study, he underwent 100 hours of ex vivo training in box-endo trainer, assisted 17 cases of TAPP repair, reviewed another 20 operative videos of TAPP hernia repair, edited those videos to learn different steps of the procedure. He also underwent stereovision test using Randot® stereotest (Stereo Optical, Chicago, IL, USA) and found to be stereo-enable. As a part of the study, he performed 25 procedures of TAPP repair for unilateral groin hernia. The first 20 cases were performed using 3D endovision system and last five cases were performed using 2D endovision system. All procedures were performed under the direct supervision of an expert surgeon (faculty) in the field of laparoscopic hernia repairs. The supervising faculty provided technical help deemed necessary and took over the procedure from the trainee if there were any technical difficulties or there was nonprogression of the procedure.
The patients with unilateral, uncomplicated, incomplete inguinal hernias, who were being prepared for elective surgery, were included in the study. Patients with ages more than 60 and less than 18 years, those who had not consented to the study, those with bilateral hernias, irreducible or obstructed hernia, recurrent hernia, patients with a history of lower abdominal surgeries, and patients with American Society of Anesthesiologist score III or more, were excluded. Written informed consent was obtained for the patients. This study was cleared by the Institutional Ethics Committee and was registered in the Clinical Trial Registry of India (CTRI-REF/2021/10/048132).
Operative procedure and equipment
All patients underwent the procedure under general anesthesia. Surgeon and camera assistant stood on the side opposite to the hernia. The monitor was placed at the foot end of the patient. Pneumoperitoneum was established using closed technique through an umbilical incision. A 12 mm Endopath XCEL™ port (Ethicon Endo-Surgery LLC, Guaynabo, USA) was placed in the umbilical region for telescope. Both working trocars (5 mm, Endopath XCEL™) were placed under vision in the pararectal line at the level of umbilicus on either side. Patient was then placed in a Trendelenburg position, turned 15° toward the surgeon.
For 3D endovision, Karl Storz system (Karl Storz Endoscopy, Tuttlingen, Germany) with TIPCAM telescope and monitor (LCD monitor, 32-inch Model number EJ-NDA32EK2) were used. The endovision system used in 2D HD was Stryker Laparoscopy System (Stryker Endoscopy, San Jose, USA) and 26-inch monitor (Vision pro26-inch LED display, Model number-BPM150524511).
TAPP repair was carried out in a standard fashion. Polypropylene heavy-weight mesh was used to cover the entire myopectineal orifice. At least two absorbable tackers were used to fix the mesh at two points and peritoneal incision was closed using barbed 3-0 polydiaxone suture (V-Loc180/Covidien, Mansfield, MA). All videos were recorded in 2D HD format for further evaluation.
The primary endpoint of the study was to evaluate the impact of 3D endovision system on learning TAPP hernia repair. The total operating time as well as the time taken for dissection, mesh placement, and peritoneal closure were looked at. The total operating time was the time from the skin incision made for insertion of the Veress needle to the closure of the skin after completion of the procedure. The dissection time was the time between peritoneal incision and the beginning of mesh insertion. The mesh placement time was the duration between insertion of the mesh to the insertion of the needle for peritoneal closure. The peritoneal closure time is the duration between insertion of the needle for peritoneal closure to the division of suture after completion of peritoneal closure. All durations were expressed in minutes. The trainee’s total operating time and time taken during various segments of the procedure were compared with that of a historical cohort of experts, based on a previously published experience of TAPP hernia repair using a 3D endovision system by the same group. 13
Secondary endpoint was to evaluate whether the skills acquired during TAPP hernia repair using 3D endovision system are transferable to perform hernia repair using 2D HD endovision system in terms of the operating time and economy of instrument movements. The recorded 2D videos of the procedure were assessed to identify the instrument path length in terms of pixels using Kinovea© (GNU GENERAL PUBLIC LICENSE Version 2, June 1991 Copyright©1989, 1991 Free Software Foundation, Inc.). This system provides an acceptable level of accuracy in angular and linear measurements obtained via digitization of x- and y-axis coordinates. 14 The economy of movement in incising the peritoneum and suturing to close it was analyzed. The faculty take over time, including the number of times and duration of the faculty takes over as operating surgeon, was recorded in each phase. Any untoward events that occurred during surgery and after surgery are recorded in a prestructured proforma.
Data analysis
The average of values or the mean values of operating time is calculated. Values by subtracting each variable are taken and plotted as a cumulative sum (CUSUM). This technique gives a graphical representation. There can be one or more inflection points where the graph descends or achieves a stable value. This was later compared by paired t-test/Wilcoxon signed-rank test, to compare the cohort before and after the inflection point which brings out the statistical probability of significant change. If there were more than one inflection point, we took the inflection point that has a more stable efferent limb.
Values were also compared in blocks using one-way ANOVA/Kruskal–Wallis test. For the purpose of the study, we divided the data into group of five. First to fifth cases were taken as first block (3D Block 1) and the consequent five cases as second, third, and fourth blocks (3D Blocks 2, 3, and 4). Last five cases of 2D endovision system were considered as 2D block.
Visual graphs and CUSUM technique were used to compare faculty take over time and trainee’s time with that of published expert cohort values. Fischer’s exact test was done to assess the distribution of comorbidities and complications. Graphical comparison was made between the faculty take over time and trainee time using area graphs in each phase of the operating time.
The analysis of the instrument path characteristics was made in terms of pixels. Path lengths in the settings of peritoneal incision and suturing process were assessed. Dominant hand movement was assessed by using the tracker in Kinovea©0.9.5 software which gave raw data. Path length was later calculated using Microsoft Excel formulas and macros to assess the values in pixels per frame. Pixel data were used to plot graphs and assess the CUSUM and split group analysis techniques. Data were analyzed using STATA 18 and Medcalc Statistical Software version 22.009 (Medcalc Software Ltd., Ostend, Belgium).
Results
A total of 25 patients underwent TAPP repair for the study. Ten patients had left-sided inguinal hernia and rest had right-sided hernia. Direct hernia was noted in 12 patients. Eight patients had comorbidities, which were evenly distributed among blocks. Four patients had identifiable predisposing factors like chronic cough, constipation, and prostatism, which were controlled before surgery. None of the patients had previous abdominal surgery or any complications of hernia preoperatively. All procedures were completed laparoscopically. There were no cases of bowel, solid organ, vascular, or bladder injuries. Bleeding that occurred during dissections was minimal and none required sutures or suction for hemostasis.
The mean operating time for TAPP repair with 3D endovision system was 74.6 minutes. CUSUM was charted for total operating time and for operating time during various phases of the procedure. Inflection point was identified and values were compared before and after it. The trainee achieved inflection point at 9th and 11th cases for total operating time and various phases of it (Fig. 1 and Table 1).

CUSUM for total operating time and operating time at different phases. Blue circles denote the cases done in 3D endovision system and red squares denote the cases done in 2D endovision system. Grey circles marked with dashed lines indicate the inflection point. CUSUM, cumulative sum.
Total Operating Time, Operating Time During Different Phases of the Procedure with Inflection Point, and Comparison Between the Cohort Before and After the Inflection Point
Split group analysis showed drop in the operating time and its phases in third block in all phases which correspond to the value in CUSUM analysis (9th–11th cases) (Fig. 2 and Table 2).

Box and whisker plot of operating time and its different phases.
Split Group Analysis of Operating Time and Its Phases Under 3D Endovision System
Skill transferability
2D block was compared with 3D Block 1 and 3D Block 4 in terms of total operating time and operating time at different phases of the procedure. Although the operating time was shorter in 2D block than that in 3D Block 1, these differences were not significant statistically. The operating time was longer in 2D block compared with the last block under 3D endovision system, that is, 3D Block 4. These differences were statistically significant for time taken to close the peritoneal incision (Fig. 2 and Table 3).
Comparison Between 3D Block 1 and 3D Block 4 with 2D Block
Faculty had taken over during the first 11 cases frequently, most of which were during the dissection of the sac and peritoneal closure (Fig. 3). There was no significant difference in faculty take over time between cases done under 2D endovision and first five cases done under 3D endovision (3D Block 1) (P = .11). However, there was a significant difference in the last five cases done under 3D systems and cases done under 2D systems, P = .0375.

Graphical representation of the trainee and faculty take over time compared with published expert cohort mean operating time. After the inflection point, the trainee values stay inside the IQR. IQR, interquartile range.
Comparative analysis of trainee’s operating times with historical expert cohort data
We have taken a historical expert cohort for comparison from a previous published study by our group. 13 That study showed mean durations of total operation 63.80 ± 18.5 minutes, preperitoneal dissection 29.1 ± 10.8 minutes, mesh placement 04.5 ± 01.4 minutes, and peritoneal fap closure 09.4 ± 04.1 minutes. Trainee’s operating duration and that of expert’s are presented in Table 4. Graphical representation of the operating time against the mean and different percentile of the expert cohort distribution shows that from the 10th case, operating time was within the middle 50 percentage (interquartile range [IQR]) of the expert cohort (Fig. 3).
Comparison of the Trainee Operating Time and Its Phases When Compared with the Expert Cohort in 3D System
Economy of movement
Scissors path length
The average path length traveled by the scissor in each case was 62,616 pixels. On CUSUM plot, the path length traversed had two inflection points, one at sixth case and another at eighth case. Since the progress was consistent after ninth case, we have accepted eighth case as inflection point (Fig. 4). The average path length of the scissor was 26,796 in 2D block, while that in 3D Blocks 1 and 4 were 156,011 pixels and 38,242, respectively. This difference was statically significant (P = .0079 and P = .00159, respectively).
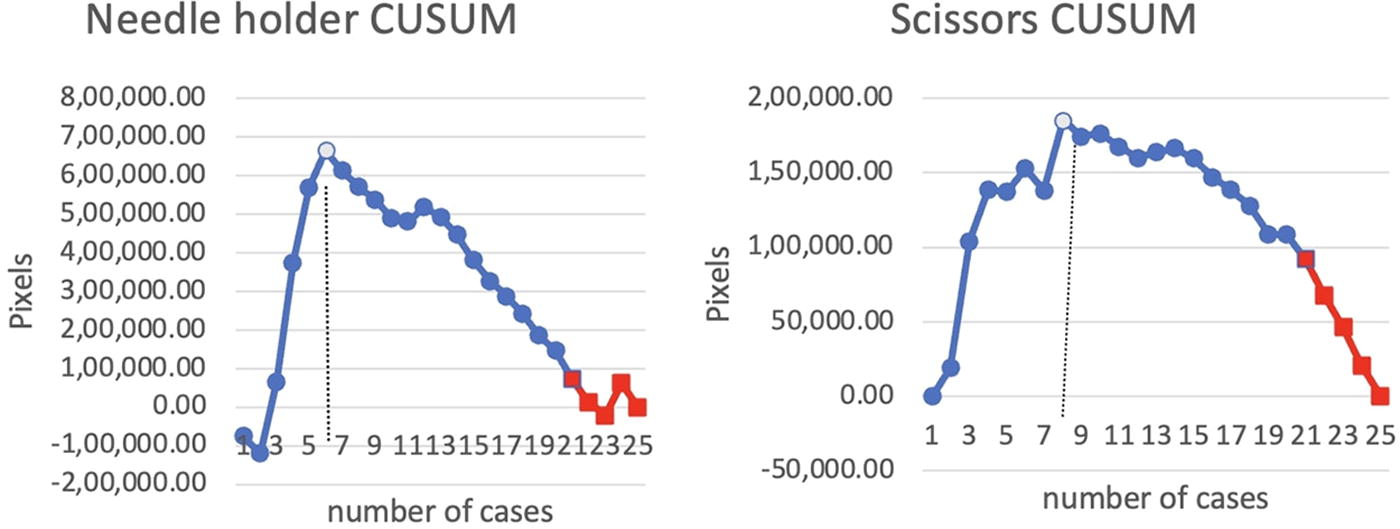
CUSUM plot analysis for path length of needle holder and scissors. Blue circles denote cases done in 3D endovision system, while red squares show cases done in 2D endovision system. Gray circle is inflection point. CUSUM, cumulative sum.
Needle holder path length
During the needle holder application, the inflection point for path length was seen at the sixth case (P = .09) in 3D system. The path length of cases done in 2D system was longer than last block of 3D but shorter than 3D Block 1, although, not significant statistically (P = .695, P = .395, respectively) (Fig. 4).
Accidental peritoneal rents happened during flap dissection and closure, the incidence was more during 2D phase than last block under 3D vision though was not statistically significant (P = .6434).
Postoperative pain was assessed on visual analog scale (VAS) of 10 on postoperative day 1. Mean VAS score was 2.56. There were no significant differences between 3D blocks and 2D endovision systems.
There were no incidences of seroma, edema of cord, or recurrence at 6 weeks. One patient had umbilical port site superficial infection requiring opening of skin incision. Culture of the fluid was sterile.
Discussion
This study was done to evaluate the impact of 3D endovision system in the learning of TAPP repair for inguinal hernia and to see if the skills acquired using 3D endovision system are transferable to perform the same procedure using 2D endovision system. A total of 25 procedures were performed by a surgical trainee, first 20 cases were done in 3D and last 5 cases in 2D endovision systems. On CUSUM analysis, inflection points were noted at 9–11th for total operating time and for various segments of procedure, and similar findings were noted on split group analysis. When compared with historical data of experts cohort, trainee’s operating time was within the middle 50 percentage (IQR) after 10th case. The total operating time although was longer in in 2D when compared with fourth block under 3D endovision, these were not significant. However, time taken for closing the peritoneal incision was significantly longer in 2D vision than that in Block 4 under 3D vision (P = .02). To the best of our knowledge, this was the first study evaluating the impact of 3D endovision technology in learning process of laparoscopic inguinal hernia repair and skill transferability from 3D to 2D environment.
Previous studies on learning process of TAPP repair under 2D endovision system showed the need for 30–75 procedures to master the technique.15–17 A meta-regression analysis showed 32.5 cases to reach proficiency. 18 A study by Bansal et al. on surgeons who were new to laparoscopic inguinal hernia repairs, but otherwise laparoscopically expert, showed operating time reaching plateau or reaching that of expert at 13th cases. 19
Our findings of infection point at 9th case represent a new insight on impact of 3D endovision system on learning process of TAPP repair for groin hernia. This along with the fact that trainees’ mean operating time was within 50th percentage of experts’ mean operating time from 10th case onwards, suggests a positive influence of 3D technology in faster learning of TAPP repair. Laparoscopic expertise of the surgical trainee in our study was limited and comparable to that of the study by Bracale et al. 16 They suggested the possibility of establishing a minimum volume of TAPP to guarantee correct training and this was found to be 65 in 2D endovision. Our study shows a possibility of faster learning of TAPP under 3D vision and could potentially change the minimum volume that the trainee requires to perform during their residency. The utility of 3D in learning of TAPP for laparoscopically expert surgeons can potentially be explored in the near future.
Our study used CUSUM method to investigate the learning process of TAPP repair. CUSUM was initially designed for detecting and improving the performance of industrial manufacturing. In recent years, it has been widely used to evaluate the learning process of novel surgical technique. It provides an objective index to estimate the minimal number of cases for acquiring skills of a new technique. CUSUM transforms original data into a continuous sum of all differences between a single figure with the mean of all figures and provides visual impression on learning process. We relied upon operating time as one of the primary criteria to evaluate the learning process. Operating time is easily measurable, statistically simpler to assess, and often accepted as a surrogate of performance. Previous studies by Brittner’s group, demonstrated that under standardized protocol, trainee surgeons were able to perform TAPP repair with similar recurrence and complication rate as that of experts, however, requiring longer operating time; suggesting the presence of learning curve only for operative duration. 17
Similar findings of operating time as the only parameter exhibiting a notable learning curve in learning TAPP hernia repair were echoed by other researchers as well.20,21
The availability of 3D endovision systems is limited at present, raising the question of transferability of surgical skills pertinent to TAPP from 3D to 2D platform. The mean total operating time and its phases in 2D were shorter than those of in the first five cases done under 3D vision although not significant. The mean total operating time and its phases were longer in 2D block than in last five cases performed in 3D and were significant for the closure of peritoneum. Trainee is thus being able to transfer his skills acquired while performing surgery in 3D to 2D, although incompletely, and raises the possibility of a second learning curve.22,23
Suturing time in 2D was significantly higher than last five cases in 3D. There have been conflicting reports regarding advantage of 3D over 2D for laparoscopic suturing, with studies showing no advantage,24,25 and other showing benefit. 26 Suturing is a complex activity that requires advanced laparoscopic skills and could potentially benefit from depth perception in 3D, which has been the case here. Trainee has shown inflection point in peritoneal closure at 11th case, but the learning trend was not uniform when endovision system was changed to 2D and required significantly more time to accomplish that under 2D vision. The direct depth cues from 3D endovision may limit the ability of the resident to do suturing with same proficiency under 2D endovision, where one needs to master the depth perception from various indirect cues. This may suggest for additional training to learn suturing utilizing indirect depth cues. On the contrary, finer skill to reduce the hernia, separation of cord structure from the sack, creation of space are mesh placement, and its placement was transferable to 2D endovision.
Main strength of the study was its prospective design and stringent methodology. Second, an objective video-based semiautomatic instrument path-length assessment protocol was used for evaluating learning process of laparoscopic hernia repair and skill transferability. Third, impact of 3D system was evaluated on performance of a surgical resident, thus the finding of positive impact of 3D system in learning TAPP repair hernia has direct clinical and educational relevance and may influence surgical education. The study is limited by the fact that bilateral hernias, complicated hernias, recurrent hernia, etc. were excluded, thus leaning pattern may be different if these patients were included. However, by exclusion of those difficult cases provided us a homogenous cohort of patients to evaluate the skill-acquiring process. Moreover, residents during their early phases of career are unlikely to endeavor for such difficult cases. Second, the study assess the learning curve for a single surgeon. Multiple residents performing more number of TAPP cases in 3D and 2D could have given a wider perspective on learning curve. Third, the residents in our study did practiced substantial time in endo-trainers, followed a standardized stepwise approach to learn the procedure, thus the results may not be reproducible elsewhere. Nevertheless, our study provide an new insight of application of 3D technology for faster learning of TAPP repair of groin hernia and may influence wider adaptation of the technique.
In conclusion, we have shown a faster learning of laparoscopic TAPP repair for groin hernia with 3D endovision system. The skills acquired under 3D endovision system are transferable to perform the procedure under 2D endovision system, albeit incompletely. The use of 3D technology may facilitate the adaptation of TAPP hernia repair by young surgeons.
Footnotes
Authors’ Contributions
H.K.B.: Conceptualization, methodology, project administration, writing—original draft, and writing—review and editing. D.J.K.: Data curation, formal analysis, resources, software, and writing—original draft. D.K.P.: Data curation. S.C.: Data curation and methodology. W.F.K.: Supervision and writing—review and editing. S.P.: Formal analysis. M.J.: Supervision. S.: Supervision. R.P.: Supervision.
Ethical Clearance
A formal ethical clearance was taken for this study.
Disclosure Statement
The authors have declared that they have no competing interests.
Funding Information
The authors have declared that they have no financial ties to disclose.