
Abstract
Background:
Abdominal perineal resection (APR) remains the gold standard for lower rectal cancer involving the anal sphincter. However, the optimal patient position remains unclear. While lithotomy or Lloyd-Davies are commonly used, APR and extra-levator abdominal perineal excision (ELAPE) in a prone jackknife position have been linked to better oncological outcomes.
Methods:
We searched PubMed, Embase, the Central Register of Clinical Trials, and Web of Science for randomized controlled trials (RCTs) and observational studies published up to February 2024. Odds ratios (ORs) with 95% confidence intervals (CIs) were pooled using a random-effects model. Heterogeneity was assessed using I2 statistics. Statistical analysis was performed with R Software version 4.4.1.
Results:
Two RCTs and 26 observational studies, including 4529 patients, were analyzed. Among them, 2249 (49.7%) underwent APR or ELAPE in the prone position and 2280 (50.3%) in the supine position. The prone position was associated with reduced surgical specimen perforation (5.3% versus 9.4%; OR: 0.44; 95% CI: 0.39–0.78; P < .001), lower positive circumferential resection margins (CRMs) rates (9.8% versus 14.3%; OR: 0.69; 95% CI: 0.53–0.89; P < .001), and decreased intraoperative bleeding (mean difference: –63.7 mL; 95% CI: −104.5, −22.8; P < .01). No significant differences were observed in operative time, urinary retention, urinary injury, wound infections, perineal dehiscence, Clavien–Dindo ≥3, reoperation, local recurrence, distal recurrence, or overall survival.
Conclusion:
The prone position during APR is associated with reduced specimen perforation, lower positive CRM rates, and less intraoperative bleeding without significant differences in other clinical outcomes.
Introduction
The gold standard treatment for locally advanced lower rectal cancer is neoadjuvant therapy followed by total mesorectal excision. 1 When the tumor involves the anal sphincter complex, the current standard approaches are abdominal perineal resection (APR) or extra-levator abdominal perineal excision (ELAPE) for extensively infiltrated lesions in the anal canal.2–5 Both procedures are performed in two stages: the abdominal and perineal phases. Conventionally, patients are positioned in lithotomy or Lloyd-Davis positions, allowing two different surgeons to operate simultaneously on both phases.6–8 However, supine approaches have not shown improved outcomes.7–11 The primary reasons for these results include a higher incidence of positive circumferential resection margins (CRM) and intraoperative bowel perforation.2–5,7–12 Some studies suggest that performing APR/ELAPE in a prone jackknife position could improve the quality of oncological specimens.3,8,9,13
In 2007, Holm described the extended posterior perineal approach, which involves preserving the mesorectum’s attachment to the levator muscles, performing perineal dissection in the prone position, disarticulating the coccyx, and removing these muscles along with the anus and lower rectum as a single unit.3,8,9,13 This approach creates a cylindrical specimen while maintaining the integrity of the anal canal and mesorectum.3,7–9,13–15 In addition, the increased tissue surrounding the tumor improves the likelihood of achieving a clear CRM and reduces the risk of intraoperative bowel perforation.5,6,8,9 However, it remains unclear whether the creation of more cylindrical specimens results from the more extensive resection itself or from the change in patient positioning to the jack-knife position, which allows better anatomical exposure during the perineal phase.
Two meta-analyses have compared APR performed in the prone jackknife position versus the lithotomy position, with conflicting results.15,16 Recently, new studies have been published comparing conventional APR or ELAPE in the prone position versus the lithotomy position. As a result, we conducted an updated systematic review and meta-analysis comparing these techniques in the prone versus supine positions.
Materials and Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (Supplementary Data S2) guidelines. 17 The study protocol was registered in the International Prospective Register of Systematic Reviews with the registration number CRD42024530969. 18
Search strategy
A systematic search was performed on PubMed, Cochrane Central Register of Clinical Trials, Web of Science, and Embase for studies published up to February 2024. Studies were identified using the following search strategy: (“Rectal Neoplasms” OR “Low rectal cancer” OR “anorectal adenocarcinoma”) AND (“Extralevator abdominoperineal excision” OR “Extralevator abdominoperineal resection” OR “Extralevator Abdominal perineal” OR ELAPE OR “Prone position” OR jackknife) AND (“conventional abdominoperineal excision” OR “conventional abdominoperineal resection” OR “standard abdominoperineal excision” OR “Standard abdominoperineal resection” OR “Abdominal perineal excision” OR “abdominal perineal resection” OR “rectal amputation” OR “Miles operation” OR APR OR APE OR SAPE OR “Supine position” OR lithotomy OR “Lloyd-Davies position” OR “ventral decubitus”). We also searched for additional studies using the references of previously included studies.
Eligibility criteria
The inclusion criteria were: (1) randomized controlled trials (RCTs) or observational studies; (2) APR or ELAPE for rectal or anal canal cancer that compared prone with supine positions during the perineal surgery phase; and (3) when multiple reports from the same study were available, we included the one with the highest quality or the most recent publication. If different outcomes were addressed in the reports, both papers were considered for the analysis.
The exclusion criteria were (1) standard coloanal anastomosis; (2) non-oncological APR; (3) studies lacking a control group or in which the control group was unreasonable; (4) non-RCTs or non-observational studies; (5) conference abstracts; and (6) overlapping populations.
Data extraction and endpoints
Two authors (B.F.P. and E.P.) independently screened articles for inclusion criteria and extracted data from included studies. Any disagreements were resolved through consensus or, if necessary, by consultation with a third author (F.B.F.). The primary endpoints assessed were: (1) specimen perforation, (2) positive CRM, (3) perineal wound infection, (4) abdominal wound infection, (5) perineal wound dehiscence, (6) operative time, and (7) intraoperative bleeding. The secondary endpoints were: (1) urinary retention, (2) urinary injury (ureteral, bladder, or urethral injury), (3) Clavien–Dindo ≥3, (4) reoperations, (5) local recurrence, (6) distant recurrence, and (7) overall survival.
Quality assessment
The evaluation of nonrandomized studies was carried out using the Cochrane Collaboration tool for assessing the risk of bias in nonrandomized studies.19,17 In this assessment, each study was categorized as critical, serious, moderate, or low risk in the six domains: confounding, selection, classification, deviations from intended interventions, missing data, measurement of outcomes and selection of reported results. The evaluation of randomized studies followed the Cochrane Collaboration tool for assessing the risk of bias in randomized trials, where studies are categorized as low-risk, high-risk, or expressing some concerns in five domains: randomization, deviations from intended intervention, missing outcome data, measurement of the outcome, and selection of the reported result.18,20 Two authors (B.F.P. and E.P.) independently assessed the risk of bias, and disagreements were resolved by consensus.
Statistical analysis
We pooled odds ratios (ORs) for binary outcomes and mean differences (MDs) for continuous endpoints, with 95% confidence intervals (CIs). A random-effects model was used for all outcomes. Statistical significance was defined as P < .05. Heterogeneity was assessed using the Cochran Q test and I2 statistics, with P-values lower than .10 and I2 >25% considered significant for heterogeneity. For outcomes with substantial heterogeneity, we used Baujat plots to assess each study’s contribution to the overall effect and heterogeneity. Furthermore, we also performed leave-one-out sensitivity analyses by systematically removing each study from the pooled estimates to ensure the robustness of the results. R Software (R Foundation for Statistical Computing), version 4.4.1, was used for the statistical analysis.
Results
Study selection and characteristics
As detailed in Figure 1, the initial search identified 1060 results. Finally, two RCTs and 26 observational studies were included in the analysis, comprising 4529 patients.2–12,21–37 Of these, 2249 (49.7%) underwent APR or ELAPE in the prone position and 2280 (50.3%) in the supine position. The mean age was 63.7 years, the mean BMI was 25.1 kg/m2, and 2866 (63.2%) were males. The follow-up ranged from 3 to 80 months. Traditionally, surgery started with the abdominal approach, followed by the perineal phase. Patients in the intervention group switched to the prone position in the final stage of surgery. In only one study, the intervention group started with the perineal phase. 29

PRISMA Flow Diagram of Study Screening and Selection.
Adenocarcinoma was the most common histological type.2–12,20–36 Only two studies included patients with squamous cell carcinoma of the anal canal.7,31 According to the cancer stage, 2343 (61.5%) had pT3 or pT4 involvement. In addition, positive lymph nodes were observed in 1196 (53.9%). The average tumor anal verge distance was 3.32 ± 0.62 cm. Neoadjuvant therapy was administered to 4383 patients (63%). All study characteristics are reported in Tables 1 and 2.
Baseline Characteristics of the Studies Included in the Meta-Analysis
Median and range.
Mean and standard deviation.
R-obs, retrospective observational study; RCT, randomized controlled trial; BMI, body mass index; NA, not available.
Surgical Characteristics of the Studies Included in the Meta-Analysis
ELAPE, extra-levator abdominoperineal excision; APR, abdominal perineal resection; NA, not available.
Pooled analyses of all studies
Surgical specimen perforation, CRM, subgroup analysis, intraoperative bleeding
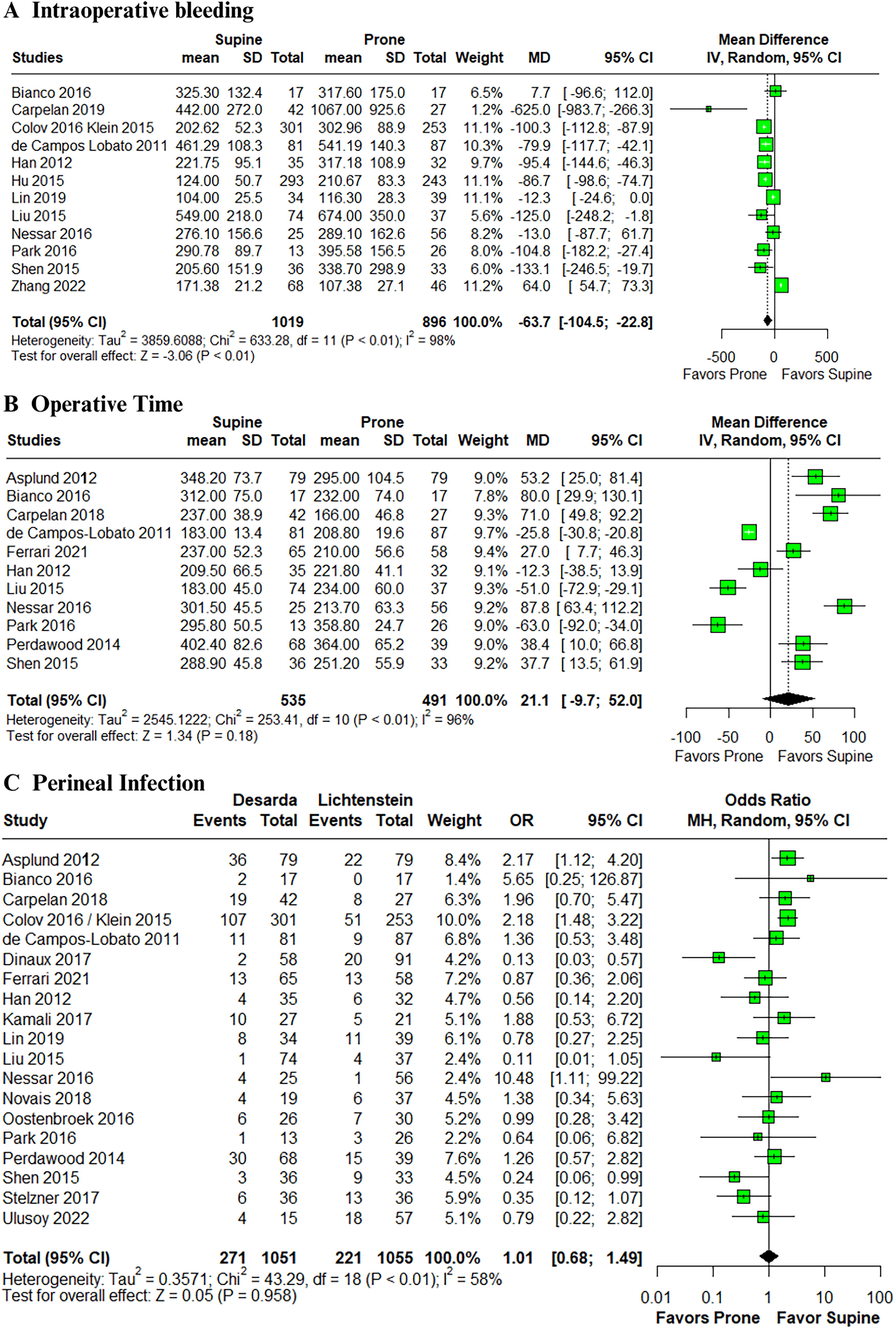
In the pooled analysis, the prone position was associated with a significant reduction in surgical specimen perforation (5.3% versus 9.4%; OR: 0.44; 95% CI: 0.39–0.78; P < .001; I2 = 27%; Fig. 2A),2–12,21–37 and lower positive CRM (9.8% versus 14.3%; OR: 0.69; 95% CI: 0.53–0.89; P < .001; I2 = 36%; Fig. 2B).2–5,7–12,21–37 We performed a subgroup analysis comparing prone APR versus supine APR and ELAPE versus supine APR. The outcomes remained consistent with prone APR (OR: 0.40; 95% CI: 0.22–0.73; P < .01; I2 = 0%) and ELAPE (OR: 0.59; 95% CI: 0.40–0.88; P < .01; I2 = 29%), reducing the chance of intraoperative perforation.2–12,21–27,29–35 However, for positive CRM, only ELAPE significantly decreased the outcome (OR: 0.67; 95% CI: 0.49–0.92; P = .01; I2 = 98%).2–11,21–37 Intraoperative bleeding was also significantly lower in the prone position group (MD: –63.7; 95% CI: −104.5, −22.8; P < .01; I2 = 93%; Fig. 3A).3,6,8,10,11,21,23–25,30,34,37 Only prone APR had low heterogeneity. The remaining outcomes demonstrated moderate and high heterogeneity.

Forest plots of comparison with subgroup analysis between prone and supine positions for abdominal perineal resection. Subgroups were APR prone versus APR supine and ELAPE (prone) versus APR Supine:
Forest plots of comparison between Prone and Supine positions for abdominal perineal resection:
Operative time, perineal infection, perineal dehiscence, abdominal wound infection
There was no significant difference between prone and supine positions in operative time (MD: 21.2; 95% CI: −9.7–52.0; P = .28; I2 = 96%; Fig. 3B),3,5,6,8,11,21–23,30,33,34 perineal wound infection (OR: 1.01; 95% CI: 0.68–1.49; P = .95; I2 = 58%; Fig. 3C),3–8,11,21–25,28,29,31,33–36 perineal wound dehiscence (OR: 0.62; 95% CI: 0.30–1.27; P = .18; I2 = 55%; Fig. 4A),4,6,7,24–28,32 and abdominal wound infection (OR: 0.80; 95% CI: .36–1.81; P = .59; I2 = 0%; Fig. 4B).3,4,6,11,21,34

Forest plots of comparison between prone and supine positions for abdominal perineal resection:
Urinary retention, urinary injury, Clavien–Dindo ≥3, reoperation
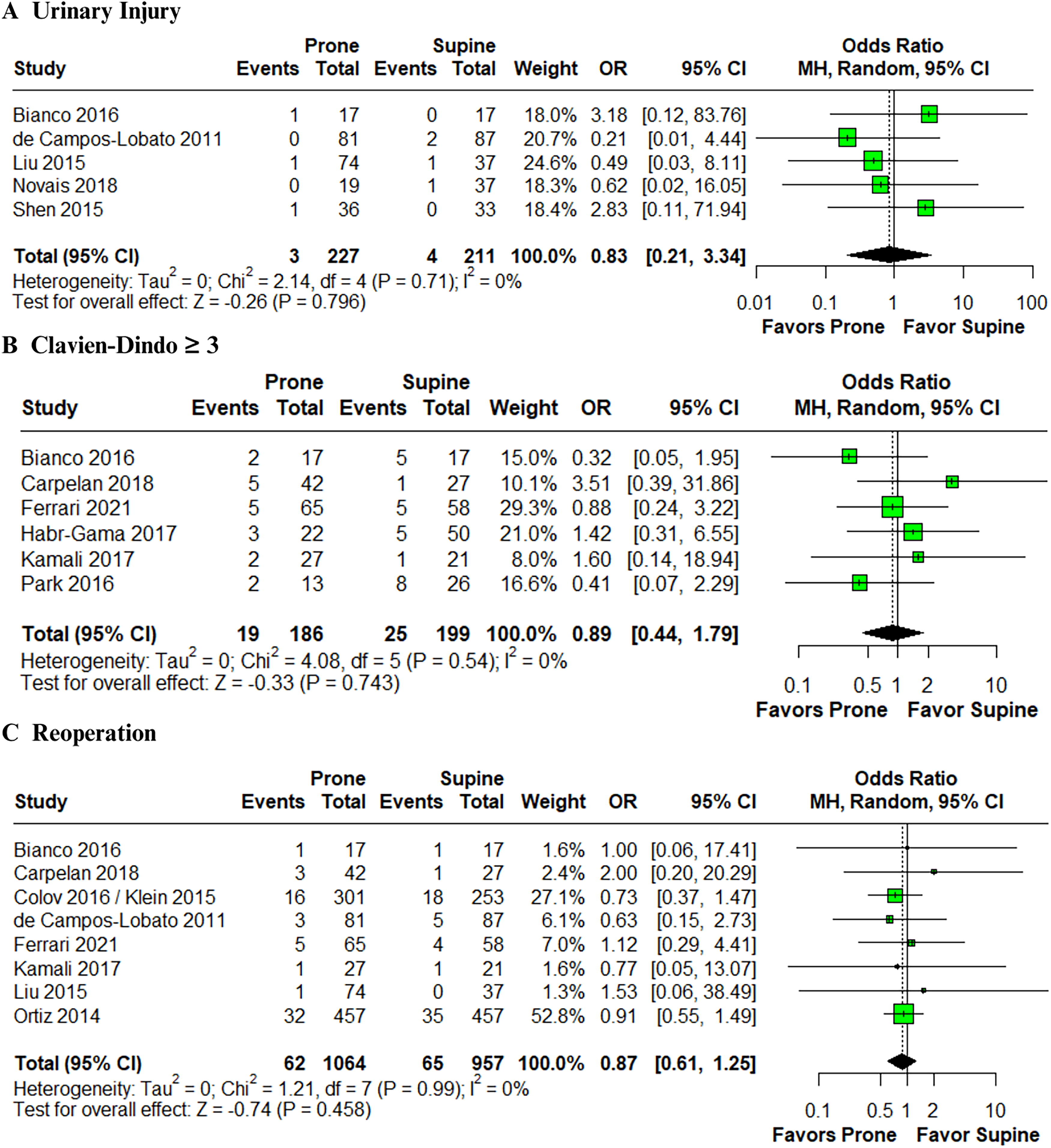
There was no significant difference between prone and supine positions in urinary retention (OR: 1.31; 95% CI: 0.69–2.48; P = .408; I2 = 0%; Fig. 4C),3,6–8,11,21,23 urinary injury (OR: 0.83; 95% CI: 0.21–3.34; P = .796; I2 = 0%; Fig. 5A),3,6,7,21,24 Clavien–Dindo ≥3 (OR: 0.89; 95% CI: .44–1.79; P = .743; I2 = 0%; Fig. 5B),5,8,21,23,26,28 or reoperation (OR: 0.87; 95% CI: .61–1.25; P = .458; I2 = 0%; Fig. 5C).3,5,6,21,23,24,28,32
Forest plots of comparison between prone and supine positions for abdominal perineal resection:
5-Year local recurrence, 5-year distal recurrence, 5-year overall survival
In the pooled analysis, we also observed no significant difference between the prone and supine positions in 5-year local recurrence (OR: 0.68; 95% CI: 0.38–1.23; P = .205; I2 = 71%; Fig. 6A),2–6,10–12,22,23,38,30,33–35 5-year distal recurrence (OR: 0.82; 95% CI: 0.55–1.23; P = .335; I2 = 0%; Fig. 6B),3–6,11,28,35 or 5-year overall survival (OR: 1.06; 95% CI: 0.84–1.35; P = .608; I2 = 3%; Fig. 6C).3–6,10,23,29,35

Forest plots of comparison between prone and supine positions for abdominal perineal resection:
Sensitivity analyses
In Baujat plot analyses, Ortiz et al. contributed substantially to heterogeneity in intraoperative specimen perforation and positive CRM (Supplementary Figs S1 and S3). 32 However, there was no change in the significance of the outcome when this study was excluded from the leave-one-out sensitivity analysis (Supplementary Figs S2 and S4). Zhang et al. were identified as the key contributor to heterogeneity in the intraoperative bleeding outcome (Supplementary Fig. S5). 37 However, the results remained consistent in the leave-one-out sensitivity analysis (Supplementary Fig. S6). Capelan and Nassar et al. were the primary sources of heterogeneity in the operative time outcome (Supplementary Fig. S7).23,30 After omitting these studies, the results were consistent in the leave-one-out sensitivity analysis (Supplementary Fig. S8). Dinaux et al. contributed to heterogeneity in the perineal wound infection outcome (Supplementary Fig. S9). 4 However, the results remained consistent in the leave-one-out sensitivity analysis (Supplementary Fig. S10). Habr-Gama et al. contributed to heterogeneity in the perineal dehiscence (Supplementary Fig. S11). 26 However, the results were consistent in the leave-one-out sensitivity analysis (Supplementary Fig. S12). Finally, Tayyab et al. contributed to heterogeneity in the 5-year local recurrence (Supplementary Fig. S13). 12 However, the results were consistent in the leave-one-out sensitivity analysis (Supplementary Fig. S14).
In addition, the funnel plot of the intraoperative bowel perforation outcome presents a symmetrical distribution of studies, indicating no evidence of significant publication bias (Supplementary Fig. S15). We also performed an Egger regression, demonstrating that the funnel plot’s distribution was insignificant (Egger test: t = −1.28, df = 22, P = .249)2–12,21–37
Quality assessment
The individual assessment of each study included in the meta-analysis is shown in Figure 7. The two RCTs were classified as low risk of bias.11,21 Sixteen observational studies presented a serious risk of bias,2,3,5,7–9,22,23,27,28,30,30,33–36 and nine were classified as having a moderate risk of bias.4,6,10,12,24–26,29,37 The domain of bias due to confounding was mainly responsible for the risk of bias in the included studies. Only one study additionally had a moderate risk of bias. 7

Critical appraisal of nonrandomized and randomized controlled trials according to the Cochrane Collaboration’s tool for assessing risk of bias.
Discussion
In this systematic review and meta-analysis of 26 observational studies and two RCTs, including 4529 patients, we compared prone and supine positions in patients undergoing APR for rectal cancer. We found that the prone position was associated with a reduction in surgical specimen perforation (5.3% versus 9.4%; OR: 0.44; 95% CI: 0.39–0.78; P < .001), lower rates of positive CRM (9.8% versus 14.3%; OR: 0.69; 95% CI: 0.53–0.89; P < .001), and intraoperative bleeding (MD: –63.7 mL; 95% CI: −104.5, −22.8; P < .01). Moreover, no significant differences were observed in operative time, urinary retention, urinary injury, perineal and abdominal wound infections, perineal dehiscence, Clavien–Dindo ≥3, reoperation, local recurrence, distal recurrence, and overall survival.
In the conventional APR technique, plane dissection near the anal canal and rectal tube creates a constriction on the specimen,4,13 which can inadvertently lead to intestinal perforation or CRM involvement.8,9,14 For this reason, performing APR in the supine position can increase the risk of intraoperative bowel perforation.3,8,12 These outcomes may negatively impact local recurrence and overall survival. In our meta-analysis, the prone position was associated with a reduction in surgical specimen perforation compared with the lithotomy position in patients undergoing APR. This finding resonates with a study conducted by Han et al. which evaluated cylindrical versus conventional APR surgical specimens and found a lower frequency of bowel perforation (5.7% versus 15.6%). 11 Similar results were observed by Lin et al. (2.9% versus 15.4%) and West et al. (3.7% versus 22.8%), showing a significant difference between groups.9,29 Park et al., on the contrary, reported more cases of bowel perforation in the prone position (15.4% versus 3.8%), but no significant difference between groups was observed. 8 In our study, a subgroup analysis, regardless of whether ELAPE or conventional APR was used, suggests that the shift from the lithotomy to the jackknife position considerably reduced the risk of intraoperative surgical specimen perforation. Specifically, the prone APR was associated with a lower perforation rate than supine APR (4.3% versus 10.2%; OR: 0.4; 95% CI: 0.22 to 0.73; P < .001). Similarly, ELAPE in the prone position showed a reduced perforation rate compared with supine APR (5.5% versus 9.2%; OR: 0.59; 95% CI: 0.40 to 0.88; P < .01).
Furthermore, our results showed that prone APR was associated with a significant reduction in positive CRM compared with the lithotomy position. This might be because resecting the levator muscles and ischiorectal fossa fat creates a true cylindrical specimen where the surrounding tissue maintains the integrity of the anal canal, mesorectum, and tumor margins.8,9,13,14 West et al. reported that the cylindrical technique was significantly associated with lower CRM involvement (14.8% versus 40.6%), 9 a finding confirmed by Han et al. (5.7% versus 28.1%). 11 Conversely, De Campos-Lobato and Lin et al. showed no differences between prone and supine positioning in CRM involvement rates.3,29
APR procedures provide poor oncological outcomes, with a 5-year cancer-specific survival of 62%.6,38,39 Dinaux et al. demonstrated no significant differences between the groups in local recurrence, long-term distant metastatic disease, or rectal cancer-related death, and similar results were observed by Liu et al.4,6 Our pooled analysis also found no differences between the groups at 5-year follow-up for local recurrence, distant recurrence, and overall survival. However, despite observing fewer perforations and better surgical margins in the APR group, there were no significant differences in 5-year survival and disease-free rates. Although the APR group had fewer perforations and better surgical margins, no significant differences were found in 5-year survival or disease-free rates. This lack of significant variation may be due to the limited number of studies and the potentially insufficient sample size in the available data. Further research with larger datasets is necessary to clarify these findings.
Switching the patient to the prone jackknife position during the perineal phase provides a more comfortable position for the surgeons. In addition, this position allows better exposure, more illumination, and improved hemostasis, reducing blood accumulation in the surgical field.8,11,29 The change in the patient’s position during surgery led to the incorrect assumption that the prone position takes longer. Han et al. demonstrated that the median time for the perineal phase was significantly shorter in the prone APR (32 versus 46 minutes). 11 Liu et al. showed that the time needed to change the operating position during prone APR was less than 18 minutes. In contrast, they found that the supine position takes longer because surgeons spend more time on exposure, operative vision, and hemostasis to avoid iatrogenic organ injury. 6 Our meta-analysis showed no significant difference in operative time between groups. In addition, our analysis demonstrated that intraoperative bleeding was lower in the prone position, a finding previously shown by Liu et al., where estimated blood loss in the intervention group was reduced by more than 120 mL. 6
However, our finding regarding estimated blood loss may be of limited clinical significance, given it was only 63.7 mL.
This study has limitations. First, most included studies are observational and cannot establish causality and might introduce bias. Second, there was significant heterogeneity in some outcomes assessed. Therefore, we performed sensitivity analyses and found mostly stable results. Third, the studies included in this meta-analysis evaluated tumors of different stages, which may have influenced the effect size found in our statistical analysis. Further RCTs are needed to determine the definitive benefits of APR in a prone position over standard techniques for targeted patient populations.
Conclusion
The prone position during APR is associated with reduced specimen perforation, lower positive CRM rates, and less intraoperative bleeding. Moreover, no significant differences were observed in operative time, urinary retention, urinary injury, wound infections, perineal dehiscence, Clavien–Dindo ≥3, reoperation, local recurrence, distal recurrence, or overall survival. These findings suggest that adopting the prone position, regardless of whether ELAPE or conventional APR is performed, could improve surgical outcomes by specifically reducing the risk of intraoperative complications.
Footnotes
Authors’ Contributions
B.F.P., S.M.P.F., and F.B.F.: Conceptualization; B.F.P., E.P., L.M.D. S.M.P.F., and F.B.F.: Methodology; B.F.P., B.P., M.R.A., L.M.D., L.S.S.P.G., and E.P.: Formal analysis and investigation; B.F.P., E.P., M.R.A., and S.M.P.F.: Writing—original draft preparation; E.P., S.M.P.F., B.F.P., L.M.D., and F.B.F.: Writing—review and editing; B.F.P., S.M.P.F., and F.B.F.: Supervision.
Disclosure Statement
F.B.F. is a speaker for Janssen Brazil. All other authors report no relationships that could be construed as a conflict of interest. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.