
Abstract
Background:
Single-port robotic-assisted radical prostatectomy (SP-RARP) has been demonstrated to be a feasible and safe procedure. Nonetheless, the challenges of SP surgery could limit the transferability of skills from multi-port (MP) console. The aim of our study was to assess the learning curve of SP-RARP.
Methods:
SP-RARPs performed by a single experienced surgeon were reviewed. The surgical learning curve was assessed using risk-adjusted cumulative summation (CUSUM) methodology in terms of operative time, separately for SP-RARPs with pelvic lymphadenectomy (PLND) and without PLND.
Results:
119 extraperitoneal SP-RARPs were evaluated, 83 with PLND and 36 without PLND. After CUSUM calculation, a cubic polynomial regression was performed to plot the learning curves. The inflection points, representing the number of cases required to achieve proficiency, corresponded to the 42nd and 20th procedure, respectively, for SP-RARP with and without PLND. The learning curves were subsequently divided into a learning phase and a proficiency phase to compare perioperative and postoperative outcomes of the two phases. In both groups, cases in the proficiency phase demonstrated significantly lower median operative times (P = .01 and P < .001) and hospital stays (P = .015 and P = .04). In the SP-RARP without the PLND group, patients in the proficiency phase demonstrated significantly lower postoperative pain scores (P = .04). No differences were found in terms of estimated blood loss, complication rates, and positive surgical margin rates (P > .05).
Conclusion:
Results from our analysis suggest that the learning curve of extraperitoneal SP-RARP is not longer than that reported for MP-RARP. Moreover, when cautiously approached, the learning process can be undertaken without compromising safety and oncological outcomes.
Introduction
Robotic-assisted radical prostatectomy (RARP) has become the mainstay intervention for the treatment of localized prostate cancer. 1 When compared to the laparoscopic approach, it demonstrates similar oncological outcomes but better functional results in terms of rates of erectile function preservation and faster incontinence recovery.2,3 In order to reduce invasiveness, a single-site surgical laparoscopic approach has been evaluated for different major urological procedures. laparoendoscopic single-site RARP (LESS RARP) using the Da Vinci multi-port (MP) Xi surgical system (Intuitive surgical Inc., Sunnyvale, CA, USA) has been proposed and demonstrated lower postoperative pain, better aesthetic results, and faster recovery than standard RARP. 4 However, technical difficulties related to the adaptation of an MP system to the limited working space of a single-site approach limited its application. The introduction of the DaVinci single-port (SP) surgical system has been the greatest surgical innovation of the last 6 years. Growing data in support of the feasibility and safety of SP urological procedures, including SP-RARP, is already emerging.5–7 Single-port robotic-assisted radical prostatectomy (SP-RARP) demonstrated reduced hospital stay, pain, and complications when compared to standard MP-RARP. 8 The docking of the DaVinci SP platform is significantly faster than the Da Vinci Xi. The console and instrumentation of the two surgical platforms are very similar, but the multi-jointed instruments and the 3D-HD articulating scope of the SP represent major differences with the Xi system. These innovations, while allowing surgeons to efficiently work in confined spaces, reduce the transferability of skills between the two systems, causing an initial learning and adaptation phase even for experienced robotic surgeons.
One of the most frequently used learning curve assessments in the surgical field is the cumulative sum curve (CUSUM) of continuous variables, such as operative time and estimated blood loss (EBL).9,10 It is based on the continuous summation of differences between the outcome of interest for each case and the target value, which is then represented in an inverse parabolic curve. Examining the learning curve is crucial for establishing the number of cases required for a surgeon to achieve proficiency, which in turn is a key determinant of better patient outcomes, as it correlates with reduced operative times and EBL. In addition, understanding the learning curve for a particular surgical procedure is essential to efficiently guide training programs, setting realistic expectations, and aiding in making informed decisions regarding patient safety during the initial learning phase. 11
In our single-center study, we assess the learning curves of extraperitoneal SP-RARP with and without PLND of a single experienced robotic surgeon with >10 years of experience with MP-RARP by applying CUSUM analysis based on operation time, with the aim to provide a reference for practitioners performing SP-RARP.
Materials and Methods
Population
We conducted a retrospective study using clinical data from patients who underwent extraperitoneal SP-RARP with or without PLND, performed in a single institution by the same experienced chief physician with the Da Vinci Single-Port Platform (Intuitive surgical Inc., Sunnyvale, CA, USA) between 2018 and 2024. The primary surgeon already had >10 years of experience and >100 cases of multi-port-RARP (MP-RARP). All cases were discussed in an MDT group prior to being offered the possible therapeutic options according to American Urological Association guidelines. 12 All included patients chose SP-RARP and signed the informed consent for the procedure. The risk for positive lymph node involvement was determined using validated nomograms,13,14 and a PLND was offered accordingly on the basis of applicable guidelines at the time of surgery. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of the University of Illinois Chicago (IRB: 2017-0152).
The inclusion criteria were:
Patients with a histologically confirmed diagnosis of nonmetastatic PCa who received SP-RARP, with or without PLND, during the specified period. All surgeries were performed by the same experienced surgeon using the extraperitoneal SP-RARP approach. All surgeries were performed using the novel DaVinci SP Platform.
The exclusion criteria were:
Patients submitted to RP with any other technology rather than the SP DaVinci Platform. Surgeries performed by other surgeons than the aforementioned experienced physician. Previous pelvic radiotherapy, chemotherapy, androgen deprivation therapy, or treatment with any medication that could impact prostate tumor growth.
Surgical procedure
The technique for extraperitoneal SP-RARP has been previously described. 15 In brief, patients are positioned in the supine position, and an 18/20Ch Foley catheter is placed to empty the bladder. A 3–4 cm suprapubic incision is made 3 fingerbreadths up from the pubic bone. After incision of the rectus fascia, finger dissection is used to develop the extraperitoneal space. The Da Vinci SP access kit with an 8 mm assistant port is positioned and after insufflation with the valveless AirSeal (ConMed, Utica, NY, USA), the robot is docked and the instrument inserted. For suction and irrigation, the ROSI (Vascular Technology Incorporated, Nashua, New Hampshire) is inserted through the assistant port. After dissection of the retropubic extraperitoneal fat of the Retzius space, the prostate and anterior bladder neck are reached. From this point, radical prostatectomy is carried out following the standard surgical steps, following a nerve-sparing approach when applicable, and performing an PLND when deemed necessary following international guidelines.
CUSUM curve construction
Assessment of the surgical learning curve was performed using risk-adjusted CUSUM methodology in terms of operative time, separately for patients undergoing SP-RARP with PLND and without PLND. First, the mean operative time (μ) was calculated as the reference value. The CUSUM for each case was then computed iteratively using the formula:
Where Xn represents the operative time for case n, and CUSUM1 was initialized at zero. To visualize trends, the CUSUM values were plotted against the case sequence to construct the CUSUM curve. The number of surgical cases was plotted on the x-axis and the CUSUM value on the y-axis. To better represent the nonlinear trends in the data, a polynomial regression was performed. The order of the polynomial that best fit the resulting learning curve was calculated using the coefficient of determination (R2), which quantifies how well the model explains variability in data. An R2 value close to 1 indicates a strong fit (i.e., the model effectively captures the trend in the learning curve). In our case, a cubic polynomial was selected, since it demonstrated the higher R2 value.
The resulting CUSUM curve allowed for the identification of trends in operative performance. An upward slope indicates an initial learning phase, whereas a downward trend suggests improvement. A stable trend near zero represents consistent performance. This method provides an objective assessment of surgical efficiency over time.
Statistical analysis
Statistical analysis was carried out using SPSS version 27.0 (IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp.) and Stata version 18.1 (Stata Corporation, College Station, TX, USA). Continuous data were expressed as number of cases, mean ± SD, median, and range, categorical variables were reported as absolute numbers and percentages. Qualitative data were compared using a Fisher’s exact test and chi-square test. Quantitative data comparison and pairwise intergroup comparisons of variables were performed using a Mann–Whitney test or an ANOVA one-way test. Statistical significance was evaluated at P < .05.
Results
Study cohort characteristics
General characteristics of the study population are shown in Table 1. A total of 119 patients who underwent extraperitoneal RARP with the Da Vinci SP platform from 2018 to 2024 were included for final analysis; of these, n = 83 (69.7%) underwent a PLND on the basis of the preoperative risk of lymph-node involvement calculated with the aforementioned validated nomograms. Median age was 64 (interquartile range [IQR]: 59–68), and median body mass index (BMI) was 27.8 (IQR: 24.6–33.1). N = 28 patients (23%) had a preoperative International Society of Urological Pathology (ISUP) grade ≥4. The most frequent ISUP grade was 2 (n = 48, 41%), and only 12% (n = 14) and 24% (n = 29) had, respectively, a preoperative ISUP grade of 1 and 3. Median preoperative prostate-specific antigen (PSA), American Society of Anesthesiologists (ASA) score, and Charlson Comorbidity Index (CCI) were, respectively, 9 ng/mL (IQR: 5.8–15.4), 3 (IQR: 2–3), and 5 (IQR: 4–6). Median and mean overall operative times were, respectively, 243 minutes (IQR: 212–281) and 250 ± 48. Since mean operative times were used for CUSUM curve construction, both mean and median are reported. Total EBL (mL) and LOS (hours) were, respectively, 100 mL (IQR: 50–200) and 9 hours (IQR: 8–18). Only n = 3 (2.5%) patients experienced any intraoperative complications.
Demographic, Perioperative and Pathological Characteristic of the Study Cohort Reviewed according to ePLND Execution (Yes or No)
ePLND, extended pelvic lymphadenectomy; IQR, interquartile range; BMI, body mass index; PSA, prostate specific antigen; ISUP, International Society of Urological Pathology; ASA, American Society of Anesthesiologists; CCI, Charlson Comorbidity Index; EBL, estimated blood loss; LOS, length of stay; SD, standard deviation.
Patients who underwent PLND had a significantly higher median preoperative PSA when compared to the non-PLND group (10.8 ng/mL, IQR: 6.6–21 versus 6.3, IQR: 4.7–10-1; P < .001) and were more likely to have a higher preoperative ISUP grade (P < .001). Median operative times were similar between the SP-RARP with and without PLND groups (P = .5). No significant differences in terms of preoperative BMI, ASA score, and CCI, EBL, complication rates, LOS, and total postoperative opioid administered were found between the two groups (P > .05).
CUSUM learning curves
The learning curve for operation time of RARP with PLND is shown in Figure 1. With an R2 = 0.78 coefficient, the best-fitting polynomial was the cubic polynomial. After plotting the curve, the cubic polynomial regression equation obtained was the following:

CUSUM learning curve for operative time of SP-RARP with ePLND. The y-axis represents the CUSUM of deviations from the mean operative time. An upward trend (positive slope) indicates that operative times are consistently longer than the expected mean (μ). A downward trend in the curve indicates that operative times are becoming shorter relative to the mean (μ).
After computing the second derivative and setting it to zero (−0.012X −0.696 = 0), the inflection point, representing the peak value for the number of cases required to achieve proficiency, was calculated and corresponded to the 42nd case.
Figure 2 shows the learning curve of operation time for RARP without PLND. The cubic polynomial was the best fit, with an R2 = 0.86. The cubic polynomial equation resulting from the polynomial regression was the following:
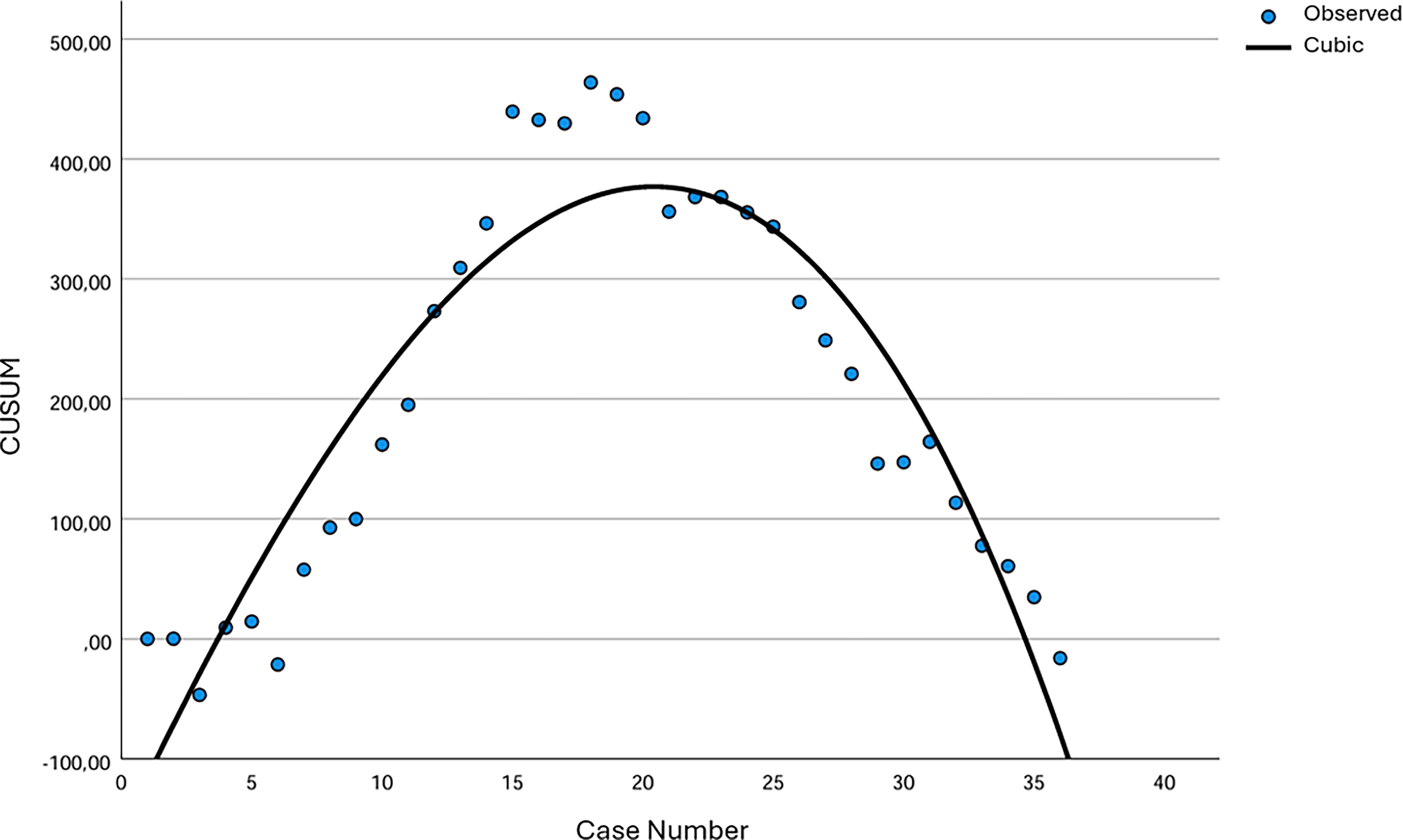
CUSUM learning curve for operative time of SP-RARP without ePLND. The y-axis represents the CUSUM of deviations from the mean operative time. An upward trend (positive slope) indicates that operative times are consistently longer than the expected mean (μ). A downward trend in the curve indicates that operative times are becoming shorter relative to the mean (μ).
The peak point of the learning curve calculated for RARP without PLND was the 20th procedure.
Comparative analysis of learning and proficiency phases
Forty-two and 20 cases were identified as the threshold for mastering SP-RARP with PLND and SP-RARP without PLND, respectively. The learning curves were divided into a learning phase (cases 1–41 and 1–19 for SP-RARP with PLND and SP-RARP without PLND) and a proficiency phase (cases 42–83 for SP-RARP with PLND and cases 20–36 for SP-RARP without PLND). Comparative analysis of perioperative and postoperative outcomes between the two phases was carried out for both groups (Tables 2 and 3). In both groups, there was a significant decrease in operative times and length of stay (LOS) between the learning and the proficiency phases (P < .05). Interestingly, despite the nonsignificant differences in terms of total postoperative opioids administered, patients operated in the proficiency phase demonstrated lower postoperative pain scores, especially in the SP-RARP without PLND group (P = .04). No intraoperative complications were found in the proficiency phases of either group. There were no significant differences in EBL between the learning and proficiency phases of both groups (P > .05). Similarly, non-focal positive margin rates and 90-day complication rates were superimposable between the learning and proficiency phases of the two groups (P > .05).
Comparison of Perioperative and Postoperative Outcomes between the Learning and Proficiency Phases for SP-RARP with PLND
SP-RARP, single-port robotic-assisted radical prostatectomy; ePLND, extended pelvic lymphadenectomy; IQR, interquartile range; EBL, estimated blood loss; LOS, length of stay; non-FPM, non-focal positive margin.
Comparison of Perioperative Outcomes between the Learning and Proficiency Phases for SP-RARP without ePLND
SP-RARP, single-port robotic-assisted radical prostatectomy; ePLND, extended pelvic lymphadenectomy; IQR, interquartile range; EBL, estimated blood loss; LOS, length of stay; non-FPM, non-focal positive margin.
Discussion
Despite its relatively new introduction, the advantages of SP robotic surgery have already been demonstrated, particularly for urological procedures. Reduced bleeding, complication rates, postoperative pain, and better cosmetic results are the most common benefits.16,17 In addition, the versatility of the systems and the maneuverability of the robotic arm allow for a standardized supine position for virtually every urological procedure, which simplifies OR setups and patient monitoring and reduces preoperative contraindications and intraoperative complications. Moreover, the majority of the operations can be carried out extraperitoneally, reducing the variability of hostile abdomens and anesthesiologic complications associated with pneumoperitoneum and improving bowel function recovery. 18 All these characteristics ultimately allow us to carry out major surgery in an outpatient setting, reducing costs and hospitalization burden. 19 After only 1 year since its EU approval, the appeal of the SP platform is growing in many European countries, and SP robotic procedures are becoming increasingly popular. In this scenario, a clear definition of the learning curve required to master SP robotic procedures is a topical demand. The narrow workspace, difficult instrument handling, and reduced mobility are the main challenges of SP robotic surgery. Achieving proficiency in this technique requires dedicated training and practice and requires a learning curve even for experienced MP robotic surgeons.
While experienced surgeons have dominated the initial discovery phase of SP robotic surgery in the United States, access to SP training and procedure is now expanding to younger surgeons and to urologists in training. Assessing the learning curve is not only a mere understanding of the skill acquisition process but is also fundamental to providing evidence-based guidance for optimizing surgical training and improving overall clinical performance. When using postoperative complication rates to determine the proficiency acquisition process of different urological SP robotic procedures, the risk of complications was minimized after 150 SP-RARPs in a recent study, providing a scenario of a steeper and longer learning curve (LC) than that demonstrated by LC studies on MP-RARP.20–22 Nonetheless, a previous systematic review of 49 robot-assisted surgery publications reported procedural time to be the most common measurement of surgical LC. 23 Ramos-Carpinteyro and colleagues, using a CUSUM method on the basis of times of specific surgical steps (console, prostate excision, PLND, and vesicourethral anastomosis), identified plateaus within the first 10–30 cases for transvesical SP-RARP. 24
In the present study, we used overall (skin-to-skin) operative times to assess the learning curve of SP-RARP, differentiating between SP-RARP with PLND and SP-RARP without PLND. Previous research reported a mean operative time for PLND at the time of RARP of 79 minutes with open, laparoscopic and MP robotic approaches and 24 minutes with the SP robotic technique.24,25 This difference can mainly be attributed to the different extension of the PLND. Indeed, means of 13 to 17 dissected lymph nodes were reported with open, laparoscopic, and MP robotic techniques compared to a median of only four nodes in the SP experience. Nevertheless, the impact of PLND on overall operative times cannot be correctly overlooked and led us to carry out our analysis separately for these two populations. Interestingly, in the current study, while mean operative times between SP-RARP with or without PLND are superimposable in the learning phase, the difference becomes evident in the proficiency phase. Moreover, this difference in mean operative time (roughly 20 minutes) is in accordance with SP-PLND times reported in previous literature. 23 While operative time is the most used data to develop LCs of robotic-assisted procedures, it is variable and can be largely influenced by different factors. For example, for oncological kidney surgery and for robotic-assisted partial nephrectomies, overall operative time is widely dependent on tumor characteristics (dimension, location, number), surgical choices (off-clamp or on-clamp), and patient’s features (previous surgery or variant anatomy). In the case of RARP, however, surgical steps are standardized, and these characteristics have little impact on surgical performance, especially in the case of an extraperitoneal approach, which mostly avoids the challenges of previous abdominal surgery. Nonetheless, operation time can still be influenced by prostate dimension, previous urological surgery, surgical team rotation, unexpected pauses, or other OR-related variables. 26 In the present study, we identified a plateau at the 42nd RARP + PLND case and the 20th RARP without PLND, with stabilization of surgical results and operative time after that landmark. After dividing the two study populations into a learning and a proficiency phase, we found significant improvements in terms of operative times, LOS, and postoperative pain scores. Interestingly, no significant differences were found in terms of EBL, intraoperative complication rates, and surgical margin positivity rates. Survival outcomes were not explored in the present study, but surgical margin positivity can be used as a surrogate for oncological safety. These results suggest that, in a cautious and safe learning process, the learning phase, despite inevitably influencing OR-related parameters and operation times, does not have a negative impact on patients’ short-time and long-time survival outcomes in oncological surgery. In the present study, SP-RARP did not demonstrate steeper learning curves than those reported for MP-RARP. Moreover, it demonstrated a smooth and safe learning process without negatively impacting on patients’ outcomes, at least in the case of MP-experienced surgeons. Despite that, the reported median operative time was significantly longer than that reported in the available literature regarding initial MP-RARP experiences, even when only taking into account the proficiency phase.27,28
Our study is not without limitations. First, as previously mentioned, while operative time is the most used parameter to develop learning curves, it is not always an indicator of a surgeon’s proficiency, as it is influenced by many different factors. Second, the adopted CUSUM model must be carefully interpreted, as its excessive visual representation can lead to asserting conclusions. 29 Despite that, the use of a polynomial regression with the evaluation of the R2 coefficient partially mitigates these disadvantages. Polynomial fitting allows for a data-driven identification of learning phases, rather than subjective cutoffs, and the goodness-of-fit coefficient (R2) ensures that our model adequately represents real data trends, minimizing the risk of arbitrary conclusions. Thirdly, we opted to divide the learning curves of SP-RARP with and without PLND because of the added surgical step on final operating times. However, since the rest of the procedure remains mostly identical, learning phases are mutually influenced, and the number of cases required to reach proficiency likely benefited from this reciprocity. Nonetheless, this is also true for other surgical operations carried out with the same approach and similar access, like different robotic-assisted kidney operations, that are normally considered separately when evaluating LCs. Third, due to the retrospective nature of the study, some useful data is lacking. For example, the lack of complete docking time data limited our ability to analyze the two phases separately and evaluate its impact comprehensively. Lastly, due to the short follow-up, we were not able to compare long-term outcomes between the learning phase and proficiency phase, such as functional results (continence and potency recovery) and recurrence rates.
Conclusions
In the present study, we adopted the CUSUM method to provide a visual representation of the learning process of extraperitoneal SP-RARP. Our results suggest that this procedure can be carried out safely even in a learning phase and did not demonstrate a steeper learning curve than that reported for its MP counterpart, despite the longer operative times. In the future, research should focus on multicenter collaborations and incorporate long-term follow-up to validate these findings.
Footnotes
Authors’ Contributions
Each of the authors contributed significantly to this research as per the guidelines of the International Committee of Medical Journal Editors. S.C., R.A., A.B., and G.F.: Study design. V.S., F.M.V., M.A., H.B.H., and L.A.M.: Data collection and analysis. V.S., S.C., G.B.D.P., and S.S.: Article preparation and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.