
Abstract
Background:
Submucosal tumors (SMT) of the esophagus and gastroesophageal junction (GEJ) are rare entities, which often present a significant challenge to surgeons. Prior studies have reported only single-modality approaches. We report our experience with SMTs using multiple surgical techniques with the intent of margin-negative resection and organ preservation.
Methods:
Between 2001 and 2022, a total of 55 patients underwent surgical resection for SMT of the esophagus or GEJ at our institution. We reviewed the electronic medical records to obtain demographic information and details of the operation. We also report peri- and early (<30 days) postoperative outcomes.
Results:
Median age at operation was 62 years (22–93), and 54.5% were male. Endoscopic ultrasound was used in 45 (81.8%) patients preoperatively to classify tumors as possibly amenable for enucleation versus requiring mucosal resection. Forty-eight (87.3%) patients underwent minimally invasive procedures. Enucleation was performed in 23 (41.8%) patients, whereas 32 (58.2%) required full-thickness resection (wedge: 18; segmental: 11) or tumor resection with mucosectomy. One patient experienced Clavien–Dindo grade III or greater complications. There were no reoperations or postoperative mortality. Pathology revealed gastrointestinal stromal tumor in 25 (45.5%) patients, leiomyoma in 22 (40%), and other histology in 8 (14.5%). Negative surgical margins were achieved in 100% of the cases. Involvement of the cardia was associated with the need for full-thickness or tumor resection with mucosectomy (68.4% versus 31.5%, P = .0214). Surveillance was conducted in 20 (36.4%) patients with a median follow-up of 656 days (210–3091). One patient had progressive multifocal disease, and another went on to develop metastatic disease.
Conclusion:
Minimally invasive approaches are appropriate in most esophageal and GEJ SMTs and are associated with low complication rates and disease recurrence. Involvement of the gastric cardia increases the likelihood of requiring full-thickness resection or tumor resection with mucosectomy rather than enucleation.
Introduction
Submucosal tumors (SMT) of the esophagus and gastroesophageal junction (GEJ) are rare and make up less than 1% of all esophageal tumors. 1 Symptoms associated with esophageal SMTs are primarily related to the size of the tumor and may include dysphagia, regurgitation, pain, gastrointestinal bleeding, or pulmonary symptoms secondary to extramural mass effect on the airways.2,3 However, these tumors are frequently discovered incidentally.
In parallel with radiographical advancements, the reliability in determining the benign nature of these lesions without the need for tissue sampling has increased. However, in some instances, imaging modalities may fail to rule out malignancy. In such cases, endoscopic forceps biopsy or endoscopic ultrasound (EUS)-guided fine-needle aspiration (FNA) may need to be utilized for definitive diagnosis. 4
Conventional treatment methods include both observation for small benign tumors and surgical resection for larger or symptomatic tumors. 5 The inability to rule out malignancy is also an indication for resection, regardless of the presence of symptoms or the size of the tumor.
Despite the rarity of esophageal SMTs, multiple resection techniques have been described, including endocopic techniques.6,7 However, not all tumors may be amenable to endoscopic resection. In these circumstances, the open approach, through either thoracotomy or laparotomy, has been described as the preferred method of resection due to its reported safety and resolution of symptoms. 3 Despite this notion, although limited, there is evidence to suggest the safety and efficacy of minimally invasive techniques in the resection of esophgeal SMTs, particularly those that involve either the GEJ or gastric cardia.8,9
To further add to the existing literature on the surgical removal of esophageal tumors, we aim to report our institution’s experience in surgically treating SMTs of the esophagus and GEJ, the majority of which were removed through a minimally invasive approach.
Methods
After institutional review board approval, we queried our electronic medical records service for patients who underwent surgical SMT resection at our institution between 2001 and 2022. Only patients over 18 years of age with SMTs located in the esophagus or at the GEJ were included. Patients with SMTs located in locations other than the esophagus or GEJ were excluded from the study.
SMTs were diagnosed preoperatively through either computed tomography (CT), magnetic resonance imaging (MRI), esophagram, or esophagoduodenoscopy (EGD). Additionally, depending on tumor characteristics and surgeon preference, some patients underwent a preoperative EUS, with or without FNA.
Resection technique was based on both the size and characteristics of the tumor, along with surgeon preference. Similarly, the choice of undergoing a laparoscopic versus robotic versus thoracotomy versus thoracoscopic approach was also based on surgeon preference. The DaVinci Surgical system (Intuitive Surgical Inc., Sunnyvale, CA, USA) platform was used in robotic operations.
In general, a contrast esophagogram was performed before initiating a diet postoperatively. Patients were discharged once they were able to tolerate a sufficient amount of oral intake and adequate pain control was achieved.
The collected variables included demographic information, body mass index (BMI), clinical and social characteristics, tumors’ location, histological type, size, and grade. Peri- and postoperative outcomes such as surgery details, mortality, early complications, early reoperations, surgical margins, lymph node involvement, and disease progression at the latest follow-up were also retrieved. Early complications were described as those occurring within 30 days of the surgery. Postoperative adverse events were described using the Clavien–Dindo classification.
The relationship between GEJ—gastric cardia involvement—and the need for mucosal resection versus enucleation was also analyzed.
Categorical variables were summarized as counts (percentages), and continuous variables were reported as median (range) or means (±standard deviation). The chi-square test was used to analyze the relationship between cardiac involvement and the type of tumor resection performed. All tests were two-sided, with a P value <.05 considered as statistically significant. The analysis was done using SPPS Statistics software.
Results
A total of 55 patients underwent surgical resection for SMTs of the esophagus or GEJ—gastric cardia—at our institution between 2001 and 2022. The median age at the time of surgery was 62 years (22–93), and 54.5% (30) were male. Most patients were Caucasian (87.2%). The mean preoperative BMI was 28.9 ± 5.6 kg/m2. Hypertension, gastroesophageal reflux disease, and hyperlipidemia were the most common comorbidities (61.8%, 54.5%, and 41.8%, respectively) (Table 1).
Demographics and Clinical Characteristics
GERD, gastroesophageal reflux disease.
Most of the SMTs were diagnosed by CT (76.4%), followed by EGD (12.7%), MRI (7.3%), and esophagogram (3.6%). Forty-five (81.8%) patients underwent preoperative EUS, with 33 (60%) having undergone FNA. Thirty-nine (71%) patients had SMTs located at the GEJ, and 16 (29%) were in the esophagus. Mean tumor size was 40.5 ± 22.2 mm (Table 2).
Submucosal Tumor Characteristics and Pathology
GEJ, gastroesophageal junction; GIST, gastrointestinal stromal tumor.
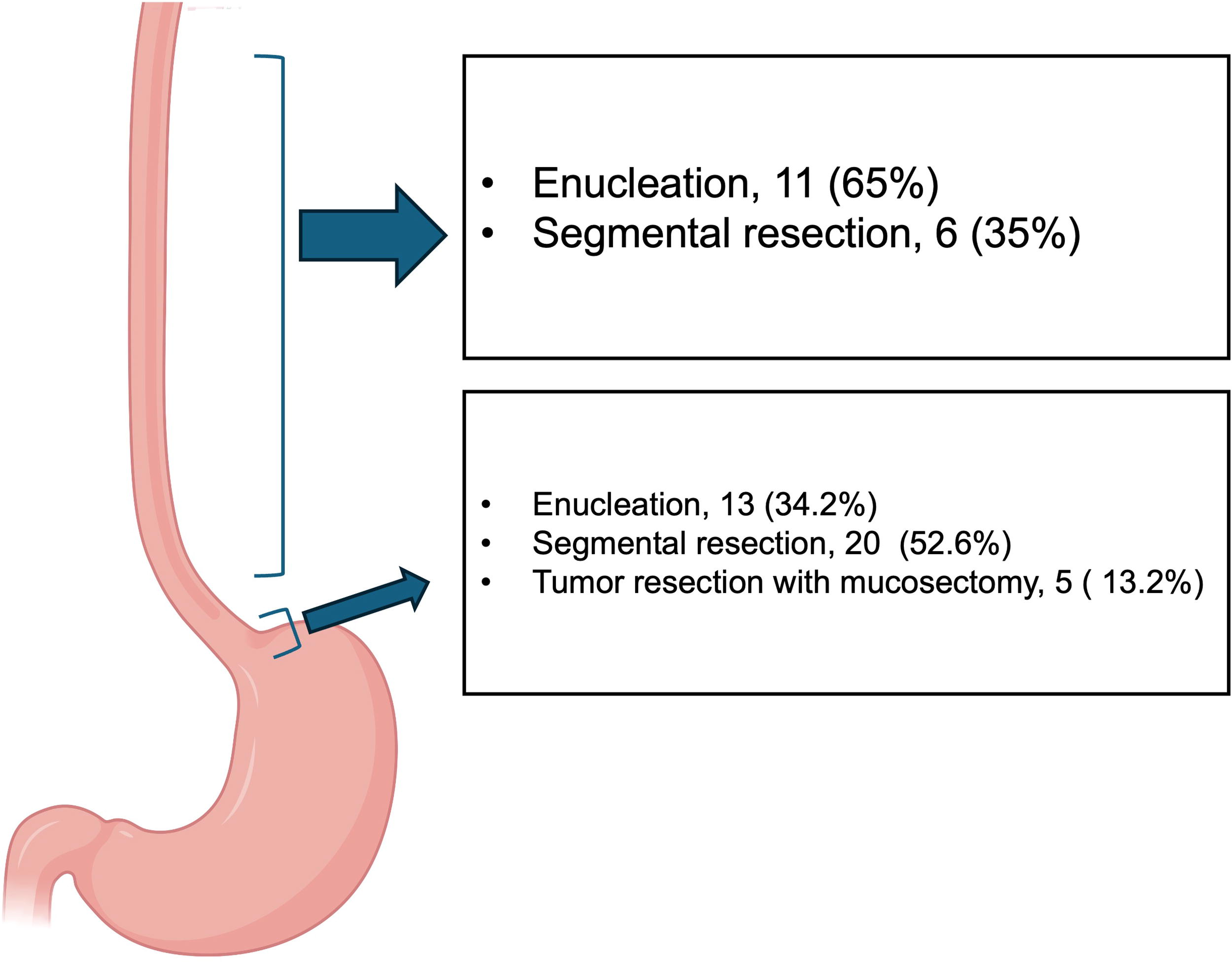
Most patients underwent a laparoscopic approach (67.3%). Enucleation was performed in 23 (41.8%) patients, whereas 32 (58.2%) required full-thickness resection (wedge: 18; segmental: 11) or tumor resection with mucosectomy (Table 3) (Fig. 1). Tumor involvement of the gastric cardia was associated with a greater likelihood of requiring mucosal resection (P = .021).
Postoperative Outcomes
Surgical approaches for esophagus and gastroesophageal junction tumor.
Ten patients developed postoperative complications, with only 1 (1.8%) being classified as ≥ grade III. This specific patient underwent an open proximal gastrectomy with anastomosis for a 10 cm gastrointestinal stromal tumor (GIST) of the GEJ and developed a perihepatic abscess on postoperative day 15 requiring drainage by our interventional radiology team. We had no early reoperations, and our 30-day mortality was 0%. Negative surgical margins were achieved in all patients. Lymph node involvement was reported in 3 (5.5%) cases; 1 who was found to have a high-grade gastric adenocarcinoma, another who had a benign GIST, and, lastly, 1 with a low-grade leiomyoma. Most of the tumors were benign (71%), and only 3 (5.5%) were high-grade (Table 2). The most common histological diagnosis was GIST (45.5%), followed by leiomyoma (40%) (Table 2).
At the latest follow-up, there was no evidence of disease progression in 53 (96.4%) patients. One patient with an intermediate-grade GIST later presented with evidence of local recurrence, and another patient with a high-grade leiomyosarcoma was found to have metastatic disease during postoperative follow-up.
Discussion
Between 2000 and 2022, a total of 55 patients underwent surgical resection for SMTs of the esophagus or GEJ at our institution. Thirty-nine (71%) SMTs involved either the GEJ or gastric cardia. Most patients underwent a laparoscopic approach (67.3%), with enucleation being the most common procedure (43.6%). Five patients were operated on robotically. Ten patients presented with postoperative complications, with only 1 (1.8%) being classified as Clavien-Dindo ≥ grade III. Most tumors were found to be benign (71%), and GIST was the most common histological diagnosis (45.5%). At the latest follow-up, there was no evidence of disease progression in 53 (96.4%) patients. Lastly, we found that involvement of the cardia was associated with a higher chance of requiring mucosal resection (P = .021).
Unlike endoscopic removal, evidence supporting the safety and efficacy of surgical removal of esophageal SMTs, particularly through MIS techniques, is limited. Similar to our study, Nguyen et al. evaluated 44 patients with esophagogastric SMTs who underwent either laparoscopic enucleation or wedge resection, suggesting safety when utilizing these approaches. 10 Although tumors within the esophagus and GEJ were included in this study, the majority were located within the stomach outside of the cardia. Shin et al. reported positive outcomes after reviewing 87 patients who had undergone surgical enucleation of esophageal SMTs. 11 However, the vast majority of these patients underwent a transthoracic approach (91%). Rahden et al. evaluated 25 patients who underwent surgical enucleation of esophageal SMTs through either a minimally invasive or open approach, concluding that minimally invasive approaches are suitable for surgical enucleation of these tumors. 12 Milito et al. published a single-institution retrospective review of 30 patients who underwent either thorascopic or laparoscopic enucleation of SMTs involving either the esophagus or GEJ, with results supporting its safety and efficacy. 13 Kent et al. evaluated 20 patients with SMTs involving either the esophagus or GEJ, the majority of whom underwent enucleation through a minimally invasive versus open approach. 14 The authors reported no major complications along with a shorter length of stay when utilizing a minimally invasive approach versus open. Unlike our cohort, the majority of the patients included in this report underwent a thorascopic approach, and, as in the report by Milito et al., most tumors were located within the esophagus as opposed to the GEJ or gastric cardia. Our reports add support to the notion that both enucleation and mucosal resection are safe when completed minimally invasively.
Highlighted in our study is the percentage of SMTs that involved either the GEJ or gastric cardia (71%). Tumors involving the cardia were more likely to require mucosal resection versus enucleation (P = .0214), which we believe is attributed to the fact that the majority of these SMTs arise within the muscularis or submucosal layers. Notably, the esophagus possesses a more distinctly defined submucosal layer compared to the stomach, which could explain the observed distribution.
Given the concern for gastric deformity or stenosis, there is debate regarding the safety of proceeding with laparoscopic wedge resection (LWR) of SMTs near the GEJ. This has prompted the conduction of case reports and retrospective reviews evaluating the results of modified, tailored procedures, such as single-incision laparoscopic (sLIGS) and transgastric techniques, in addition to reports promoting the safety of endoscopic-assisted LWR to address these tumors.15–21 With regard to conventional laparoscopic techniques, a case report was published by Bogoevski et al., who described successful performance of a full-thickness laparoscopic wedge excision of a submucosal tumor less than 1 cm away from the gastric cardia. 22 Wang et al. reviewed 12 cases of patients who underwent total laparoscopic intragastric surgery (T-LIGS) for cardia endogenous gastric SMTs, reporting positive outcomes. 23 However, this report was limited by a lack of long-term evaluation. Liao et al. evaluated 19 patients with SMTs located near the GEJ who underwent either endoscopic stapled resection or transgastric tumor resection with mucosectomy, supporting the feasibility and safety of laparoscopic resection. 24 Hwang et al. published a study reviewing 63 patients, 6 of whom involved the GEJ. 25 Five of these patients were treated by laparoscopic enucleation and one by tumor-everting resection, with reported positive outcomes. The greatest evidence supporting the safety and feasibility of laparoscopic resection of submucosal tumors near the gastroesophageal junction likely stems from a study reported by Kim et al. 9 In this report, 71 patients, 66 of whom underwent laparoscopic wedge resection, were evaluated. This study was limited by the lack of long-term follow-up data, including data development of recurrent disease.
Strengths and limitations
One of the major strengths of this study is that it represents one of the largest single-institution experiences focused on the surgical resection of esophageal and GEJ SMTs. Furthermore, the achievement of negative surgical margins in 100% of cases underscores the oncologic soundness of these approaches. The remarkably low rate of serious complications (Clavien–Dindo grade III or higher in only one patient) and the absence of 30-day mortality further support the safety and efficacy of minimally invasive surgical strategies for SMTs.
However, the study is not without limitations. As a retrospective analysis, it is subject to inherent biases, including selection and information bias, which could affect the validity of the findings. The lack of long-term follow-up for a portion of the cohort may have resulted in underestimation of recurrence rates or delayed complications. Being a single-center study, the generalizability of these results to other institutions with varying levels of surgical expertise and resources may be limited.
Conclusion
Our findings suggest that laparoscopic approaches, via enucleation and mucosal resection, can be performed with minimal complications and favorable patient outcomes. Additionally, we found that SMTs involving the GEJ or gastric cardia were more likely to require mucosal resection compared to enucleation.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
S.P.B. receives compensation for Educational Consulting from BK Medical, a subsidiary of General Electric; Dr. Bowers is founder, shareholder, and Chief Medical Officer of the Suture Shield LLC, a surgical device manufacturer that has not initiated the government regulatory approval process.