
Abstract
Background:
Laparoscopic surgery (LS) is widely recognized as the standard minimally invasive method for colorectal cancer. Although robotic surgery (RS) has seen increased adoption, its clinical and economic advantages over LS remain uncertain.
Methods:
A systematic search was carried out across PubMed, Scopus, and the Cochrane Central Register up to March 2025. Only randomized controlled trials (RCTs) directly comparing RS and LS were included. Pooled risk ratios (RRs) and mean differences (MDs) with 95% confidence intervals (CIs) were calculated using random-effects models. Heterogeneity was assessed via the I2 statistic. Trial sequential analysis (TSA) was applied to assess the robustness of the cumulative evidence.
Results:
Fourteen RCTs encompassing 2867 patients were included. Compared with LS, RS significantly lowered the conversion rate to open surgery (RR = 0.54; 95% CI: 0.36–0.80; P = .002), time to first stool (MD = −0.33 days; 95% CI: −0.60 to −0.06; P = .016), and positive circumferential resection margin (CRM) (RR = 0.65; 95% CI: 0.46–0.93; P = .017). Sensitivity analysis revealed a slight benefit for RS in time to first flatus (MD = −0.13 days; P = .03). RS was associated with a longer surgery duration (MD = +49.4 minutes; 95% CI: 18.0–80.7; P = .002). No significant differences were observed for intraoperative blood loss, postoperative complications, or cancer recurrence. TSA confirmed definitive findings for selected outcomes, while others remained underpowered.
Conclusions:
RS and LS showed equivalent results for postoperative complications and cancer-related outcomes. RS was advantageous in reducing conversion and CRM positivity, despite longer operative time.

Introduction
Colorectal cancer represents a significant global health issue, ranking consistently among the most commonly diagnosed malignancies and one of the primary contributors to cancer-related mortality worldwide.1,2 In recent decades, minimally invasive surgical techniques have emerged as the preferred approach for managing colorectal tumors, offering benefits such as accelerated postoperative recovery, reduced physiological impact, and decreased need for analgesics, all while preserving oncologic safety when compared with traditional open procedures.3–16 Laparoscopy is well established as the standard approach for colorectal resections; however, the value of robotic-assisted surgery continues to be debated.4–7,9,11–14 Although robotic platforms were designed to overcome specific limitations of laparoscopy, such as restricted instrument mobility and ergonomic strain, their widespread use is hindered by the lack of robust evidence demonstrating clinical superiority over traditional laparoscopic methods.3,6–9,11–16
Robotic surgery (RS) has been associated with several potential advantages over laparoscopy, including enhanced instrument articulation, high-definition three-dimensional visualization, steady camera control, and improved surgeon ergonomics, all of which may facilitate more precise dissection in confined pelvic spaces.3,6–9,11–16 These features have led some to consider robotic platforms a viable and potentially superior option in complex colorectal procedures.4–7,9,11–14 Nevertheless, concerns remain regarding the elevated costs of robotic systems, and current evidence has yet to clearly demonstrate their clinical superiority over conventional laparoscopy.3,6–9,11–16
Previous meta-analyses assessing RS and laparoscopic surgery (LS) have often presented methodological limitations, such as the combination of randomized trials and observational studies, the inclusion of heterogeneous colorectal conditions, and potential overlap of patient cohorts across studies.17–22 To address these issues, the present meta-analysis was restricted to RCTs, excluded duplicated datasets, and focused specifically on patients undergoing surgery for colorectal cancer. The primary objective was to compare robotic and laparoscopic techniques in terms of postoperative complications, perioperative performance, and oncologic outcomes.
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations, 23 as detailed in Supplementary Table S1. The protocol was registered in advance in the International Prospective Register of Systematic Reviews (PROSPERO) under the identification number CRD420251025708. 24 As this analysis is based solely on previously published studies, ethical approval was not required. To ensure methodological transparency and adherence to good publication practices, all included studies are appropriately cited, and standardized language is used where applicable. This approach aligns with the recommendations of the Committee on Publication Ethics (COPE) regarding acceptable text reuse, with any overlapping phrasing employed solely to preserve clarity and reproducibility. 25
Systematic search process
We conducted a broad literature search using PubMed, the Cochrane Central Register of Clinical Trials, and Scopus to identify studies published until March 2025. The PubMed search strategy was as follows: (“colorectal neoplasms”[MeSH Terms] OR “colorectal cancer”[tiab] OR “colorectal neoplasm”[tiab] OR “colon cancer”[tiab] OR “rectal cancer”[tiab] OR “colon neoplasms”[MeSH Terms] OR “rectal neoplasms”[MeSH Terms] OR “colon neoplasm”[tiab] OR “rectal neoplasm”[tiab] OR “bowel cancer”[tiab]) AND (“robotic surgical procedures”[MeSH Terms] OR “robotic surgery”[tiab] OR “robot-assisted surgery”[tiab] OR “robot-assisted”[All Fields] OR “robotic-assisted”[All Fields] OR “robotic”[tiab] OR “da Vinci”[All Fields]) AND (“laparoscopy”[MeSH Terms] OR “laparoscopic”[tiab] OR “laparoscopic surgery”[tiab] OR “laparoscopic-assisted”[tiab] OR “laparoscopic approach”[tiab] OR “laparoscopic resection”[tiab] OR “laparoscopic colectomy”[tiab] OR “laparoscopic proctectomy”[tiab] OR “laparoscopic”[All Fields]). The Scopus and Cochrane strategies used simplified terms, as follows: (“colorectal cancer” OR “colon cancer” OR “rectal cancer”) AND (“robotic surgery” OR “robot-assisted surgery” OR “robotic-assisted surgery”) AND (“laparoscopic surgery” OR “minimally invasive surgery”).
Study selection criteria
We included RCTs that compared robotic and laparoscopic surgical approaches for colorectal cancer, regardless of tumor site or treatment context, including both upfront surgery and perioperative strategies. Exclusion criteria were as follows: (1) studies involving histological subtypes other than adenocarcinoma; (2) studies focusing on benign colorectal conditions; (3) studies lacking a comparative control group; (4) publications classified as noneligible formats, such as single-arm trials, case reports, conference abstracts, meta-analyses, narrative reviews, or animal studies; and (5) studies with overlapping patient populations, in which the most recent or most comprehensive dataset was prioritized.
Data extraction and endpoints
Two independent reviewers (B.D.P. and L.E.B.M.A.) assessed the retrieved articles for eligibility and performed data extraction from the studies that met the inclusion criteria. Discrepancies were resolved by consensus, and when necessary, a third reviewer (B.F.P.) provided adjudication. The following intraoperative and postoperative outcomes were evaluated: (1) conversion to open surgery, (2) intraoperative blood loss, (3) intraoperative complications, (4) postoperative pain on day 1 (visual analog scale [VAS] 1-day), (5) VAS 2-day, (6) VAS 5-day, (7) overall postoperative complications, (8) anastomotic leakage, (9) severe complications (Clavien-Dindo grade ≥ III), (10) reoperation, (11) hospital readmission, (12) operative time, (13) time to oral intake, (14) time to first flatus, (15) time to first stool, (16) length of hospital stay, (17) 30-day mortality, (18) positive circumferential resection margin (CRM), (19) distal resection margin, (20) specimen perforation, (21) completeness and integrity of mesorectal excision, (22) number of lymph nodes harvested, (23) local recurrence, and (24) distant metastasis.
Quality assessment
Two reviewers (B.F.P. and V.M.) independently assessed the risk of bias of the included randomized controlled trials (RCTs) using the revised Cochrane risk-of-bias tool (RoB 2). 26 Each trial was categorized as having low, high, or some concerns regarding bias across five domains: the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported results. Disagreements were resolved by consensus, with arbitration by a third reviewer (F.B.F.) when required. The certainty of evidence for each outcome was rated using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework, with levels of confidence classified as very low, low, moderate, or high. 27 Publication bias was evaluated by visual inspection of funnel plot asymmetry and tested using Egger’s regression method for outcomes reported in at least 10 studies.28–30
Statistical analysis
Risk ratios (RRs) and their associated 95% confidence intervals (CIs) were computed for binary outcomes. Continuous variables were analyzed using mean differences (MDs), also presented with 95% CIs. All results were pooled using random-effects models based on the DerSimonian and Laird method. 31 A P value <.05 indicates rejection of the null hypothesis. Heterogeneity across studies was evaluated using both the Cochran Q test and the I2 statistic; values >25% and P values <.10 were interpreted as indicative of substantial heterogeneity. Statistical analyses were performed using R software version 4.4.1, and trial sequential analysis (TSA) was conducted with TSA software version 9.5.10.
Sensitivity analysis
For outcomes with substantial heterogeneity (I2 ≥ 25%), we performed additional sensitivity analyses using three distinct strategies: First, Baujat plots were generated to identify which individual studies had the greatest influence on both the pooled estimate and overall heterogeneity. 32 Second, a leave-one-out analysis was carried out, where each study was sequentially excluded to determine whether the findings were dependent on any single trial. Third, TSA was employed to evaluate the potential for random errors and to enhance the precision of the evidence. In TSA, the cumulative Z-curves were interpreted using adjusted monitoring thresholds based on the O’Brien–Fleming alpha-spending approach. The required information size (RIS) was computed assuming a type I error of 5% and a type II error of 20%, incorporating the pooled MD and the estimated heterogeneity (D2) derived from applying a random-effects model to the pooled data of all included studies. 33
Results
Study inclusion and baseline characteristics
In Figure 1, we describe the results of the literature search, which initially identified 4329 records. After removing 1635 duplicates and excluding 2672 based on title and abstract screening, 14 RCTs were included in the final analysis.3–16 Collectively, these studies encompassed 2867 patients who underwent surgical treatment for colorectal cancer. Among them, 1434 individuals (50.1%) underwent RS, while 1433 (49.9%) were treated with LS. The mean follow-up of all included trials was 23.8 ± 16.9 months.3–16 Males comprised 1829 participants (64% of the total population).3–16 The average age in the RS group was 60.9 ± 11.1 years, compared with 62.1 ± 11.0 years in the LS group. Body mass index was comparable between groups, averaging 23.96 ± 3.84 kg/m2 in RS and 23.74 ± 3.83 kg/m2 in LS.3–16 Based on the classification of the American Society of Anesthesiologists (ASA) Physical Status Classification, most patients were categorized as ASA I (42.7%), ASA II (37.2%), ASA III (19.4%), and ASA IV (0.7%).3–16 With respect to tumor location, the majority were in the rectum (72.0%), followed by the sigmoid colon (15.2%), left or transverse colon (8.1%), and right colon (4.7%).3–16 Among the studies that reported clinical staging, 944 patients (53%) were classified as having T3 tumors.3–16 The most commonly performed surgical procedures included low anterior resection in 54.2% of cases, abdominoperineal resection in 24.4%, total mesorectal excision (TME) in 10.3%, right colectomy (RC) in 2.1%, and segmental colectomy in 2.0%.3–16 A detailed overview of the remaining study characteristics is presented in Tables 1 and 2.
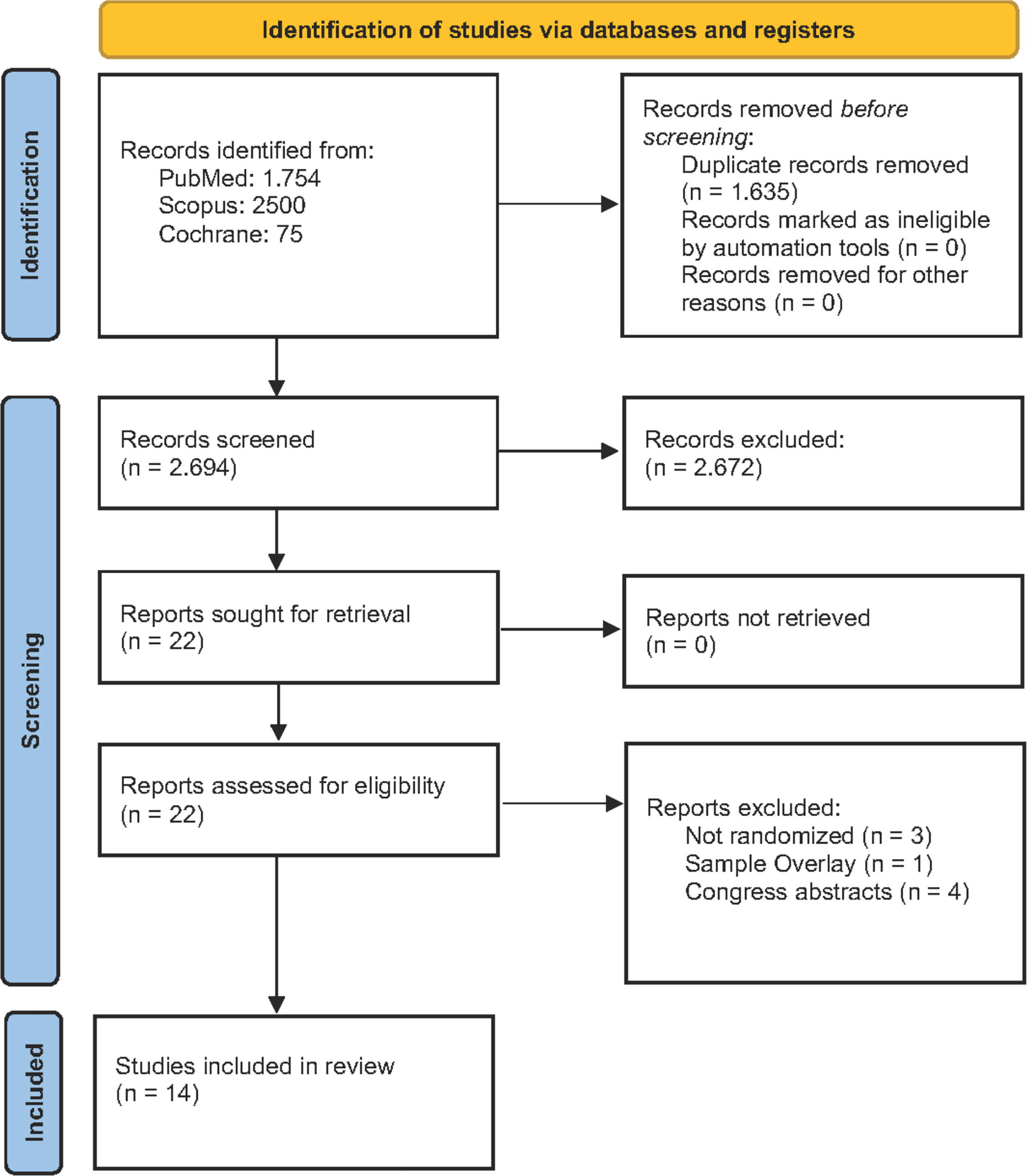
PRISMA Flow Diagram of Study Screening and Selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Baseline Characteristics of the Included Studies
aMean (no SD given).
ASA, American Society of Anesthesiologists; BMI, body mass index; LS, laparoscopic surgery; RS, robotic surgery; SD, standard deviation.
Surgical Characteristics of the Included Studies
APR, abdominal perineal amputation; CAA, intersphincteric resection with coloanal anastomosis; DS, double stapling; EA, extracorporeal anastomosis; EE, end-to-end anastomosis; ERC, extended right colectomy; HAR, high anterior resection; HS, hand-sewn; IA, intracorporeal anastomosis; LAR, low anterior resection; LC, left colectomy; NA, not available; PME, partial mesorectal excision; RAR, rectal anterior resection; RC, right colectomy; Rt, rectum; SC, sigmoid colectomy; SD, standard deviation; SFR, splenic flexure resection; Sig, sigmoid; SS, side-to-side; SST, single stapling; TL, tumor location; TNM, tumor, node, metastasis system; Tv, transverse colon.
Pooled analyses of the included studies
Intraoperative complications
In our pool of studies, RS was associated with a significantly lower rate of conversion to open surgery compared with LS (RR = 0.54; 95% CI: 0.36–0.80; P = .002; I2 = 0%; Fig. 2A), with no evidence of heterogeneity across studies.3–10,12–16 There was no statistically significant difference between RS and LS in terms of intraoperative blood loss (MD = −9.91 mL; 95% CI: −64.41 to 44.59; P = .721; I2 = 91.4%; Fig. 2B) or intraoperative complications (RR = 0.83; 95% CI: 0.60–1.15; P = .263; I2 = 0%; Fig. 2C).4–7,9,10,12–16 Blood loss highlights high levels of heterogeneity, and intraoperative complications indicate low heterogeneity.
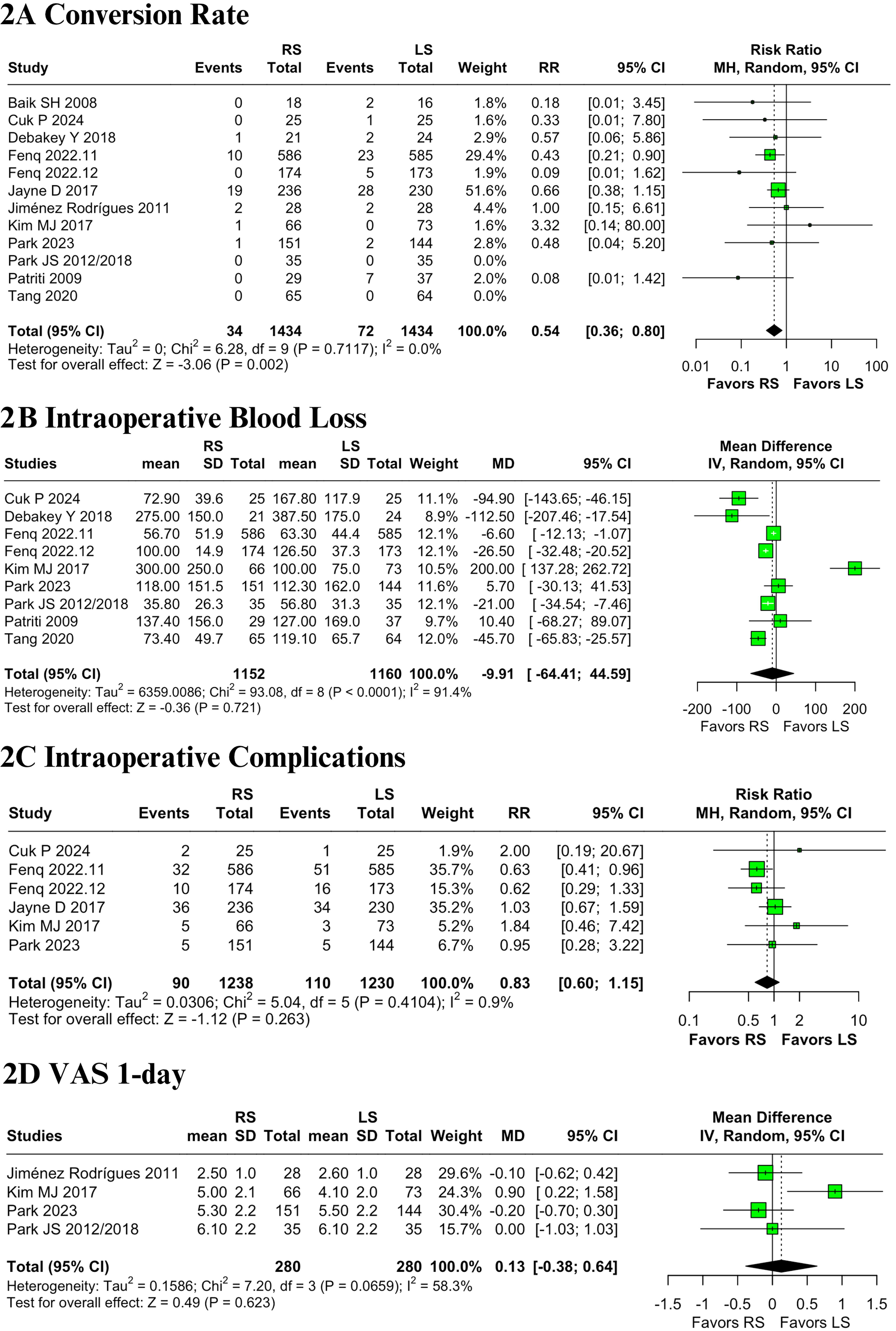
Forest plots comparing robotic and laparoscopic approaches for colorectal cancer:
Postoperative pain
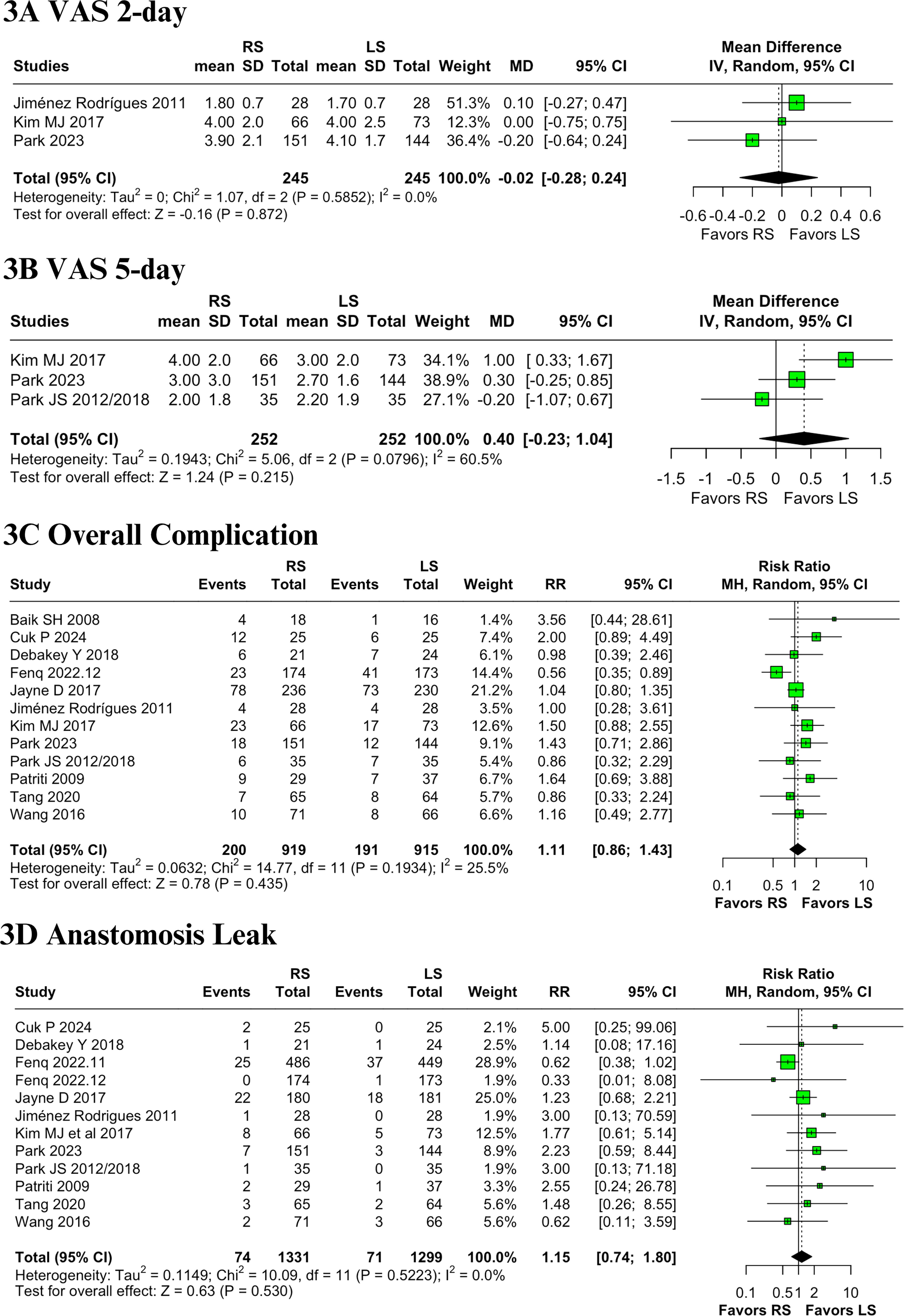
The analysis revealed no statistically significant differences between RS and LS in terms of postoperative pain scores. For VAS 1-day, the MD was 0.13 (95% CI: −0.38 to 0.64; P = .623; I2 = 58.3%; Fig. 2D).8–10,13,16 Similarly, VAS 2-day showed no difference between groups (MD = −0.02; 95% CI: −0.28 to 0.24; P = .872; I2 = 0%; Fig. 3A),8,13,16 and the VAS 5-day comparison also failed to reach statistical significance (MD = 0.40; 95% CI: −0.23 to 1.04; P = .215; I2 = 60.5%; Fig. 3B).9,10,13,16 While VAS 2-day demonstrated no heterogeneity across studies, moderate to high heterogeneity was observed in the VAS 1-day and VAS 5-day analyses.
Forest plots comparing robotic and laparoscopic approaches for colorectal cancer:
Postoperative complications
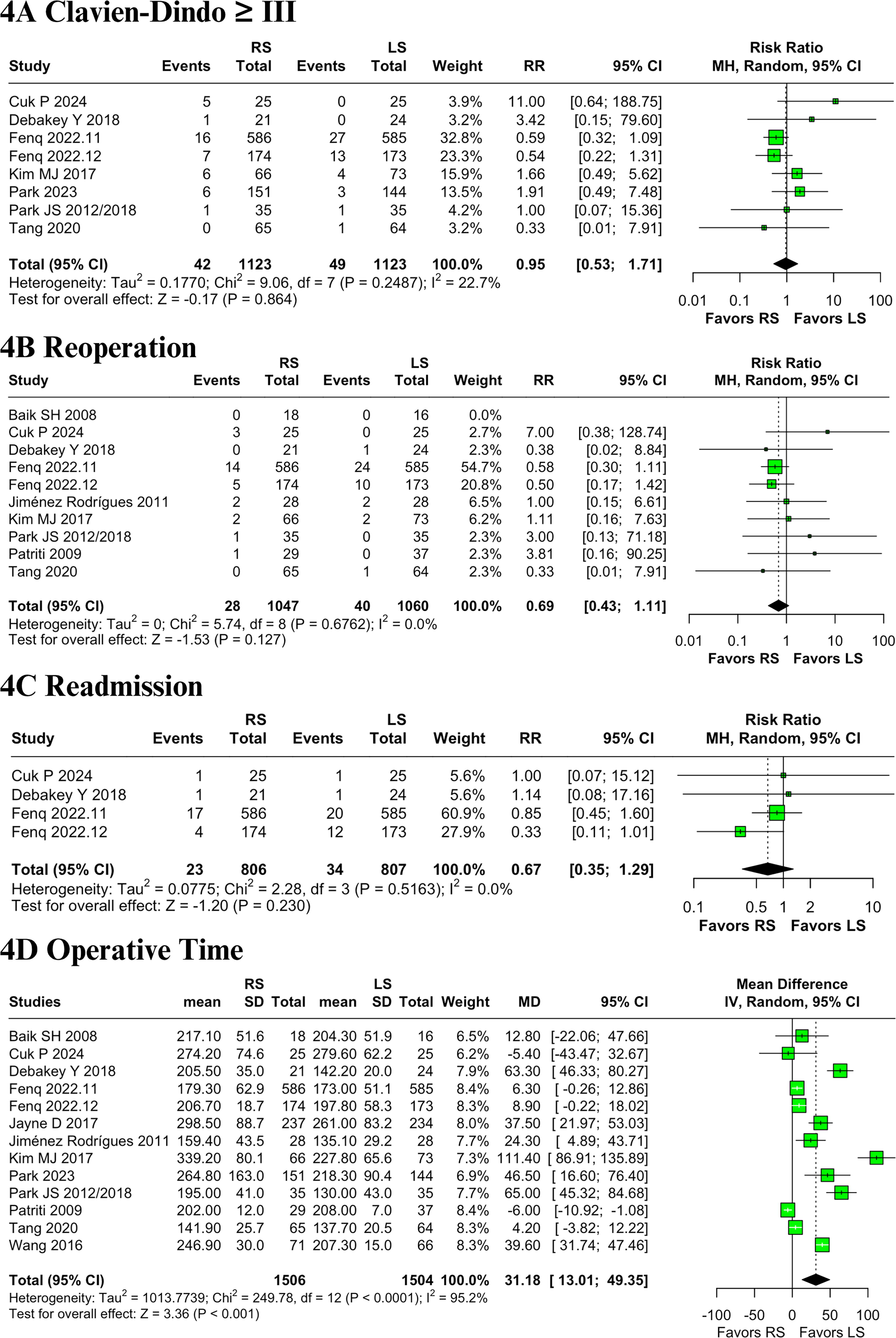
The pooled analysis showed no statistically significant differences between RS and LS in several postoperative outcomes. These included overall complication rates (RR = 1.11; 95% CI: 0.86–1.43; P = .435; I2 = 25.5%; Fig. 3C),3–5,7–16 anastomotic leakage (RR = 1.15; 95% CI: 0.74–1.80; P = .530; I2 = 0%; Fig. 3D),4–16 and severe complications classified as Clavien-Dindo grade ≥ III (RR = 0.95; 95% CI: 0.53–1.71; P = .864; I2 = 22.7%; Fig. 4A).4–6,9,10,13–16 There were also no significant differences in reoperation rates (RR = .60; 95% CI: 0.35–1.11; P = .110; I2 = 0%; Fig. 4B)3–6,8–10,13–16 or hospital readmissions (RR = .77; 95% CI: 0.35–1.29; P = .230; I2 = 0%; Fig. 4C).4–6,14 Overall complications showed moderate heterogeneity, and the other outcomes showed low heterogeneity.
Forest plots comparing robotic and laparoscopic approaches for colorectal cancer:
Gastrointestinal postoperative recovery, operative time, hospital stay, and mortality
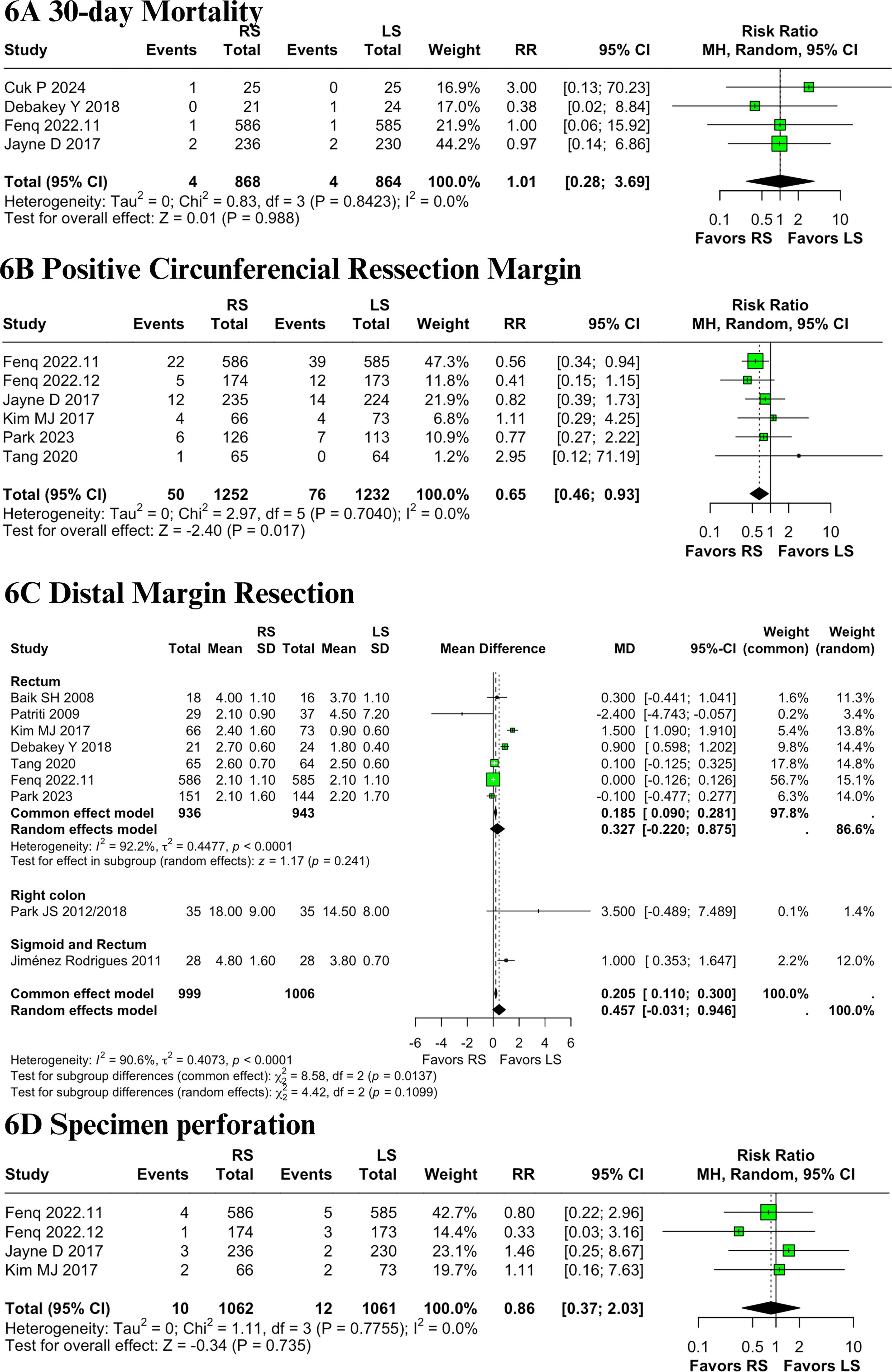
RS was associated with a significantly longer operative time compared with LS (MD = +49.4 minutes; 95% CI: 18.0–80.7; P = .002; I2 = 95.2%; Fig. 4D). There was a high heterogeneity observed across studies.3–16 In terms of gastrointestinal (GI) recovery, there were no significant differences between groups regarding time to oral intake (MD = −0.30 days; 95% CI: −0.78 to 0.19; P = .234; I2 = 91.0%; Fig. 5A) or time to first flatus (MD = −.27 days; 95% CI: −0.64 to 0.10; P = .156; I2 = 94.3%; Fig. 5B),4–6,8–10,15,16 both outcomes showing high heterogeneity. However, RS was associated with earlier recovery of bowel function, as indicated by a shorter time to first stool (MD = −0.33 days; 95% CI: −0.60 to −0.06; P = .016; I2 = 33.5%; Fig. 5C), with moderate heterogeneity.5,14,16 No significant differences were found between RS and LS in terms of length of hospital stay (MD = −0.36 days; 95% CI: −0.97 to 0.26; P = .257; I2 = 88%; Fig. 5D) or 30-day mortality (RR = 1.01; 95% CI: 0.28–3.69; P = .988; I2 = 0%; Fig. 6A).3–16 High heterogeneity was present for hospital stay, while mortality analysis showed no heterogeneity.

Forest plots comparing robotic and laparoscopic approaches for colorectal cancer:
Forest plots comparing robotic and laparoscopic approaches for colorectal cancer:
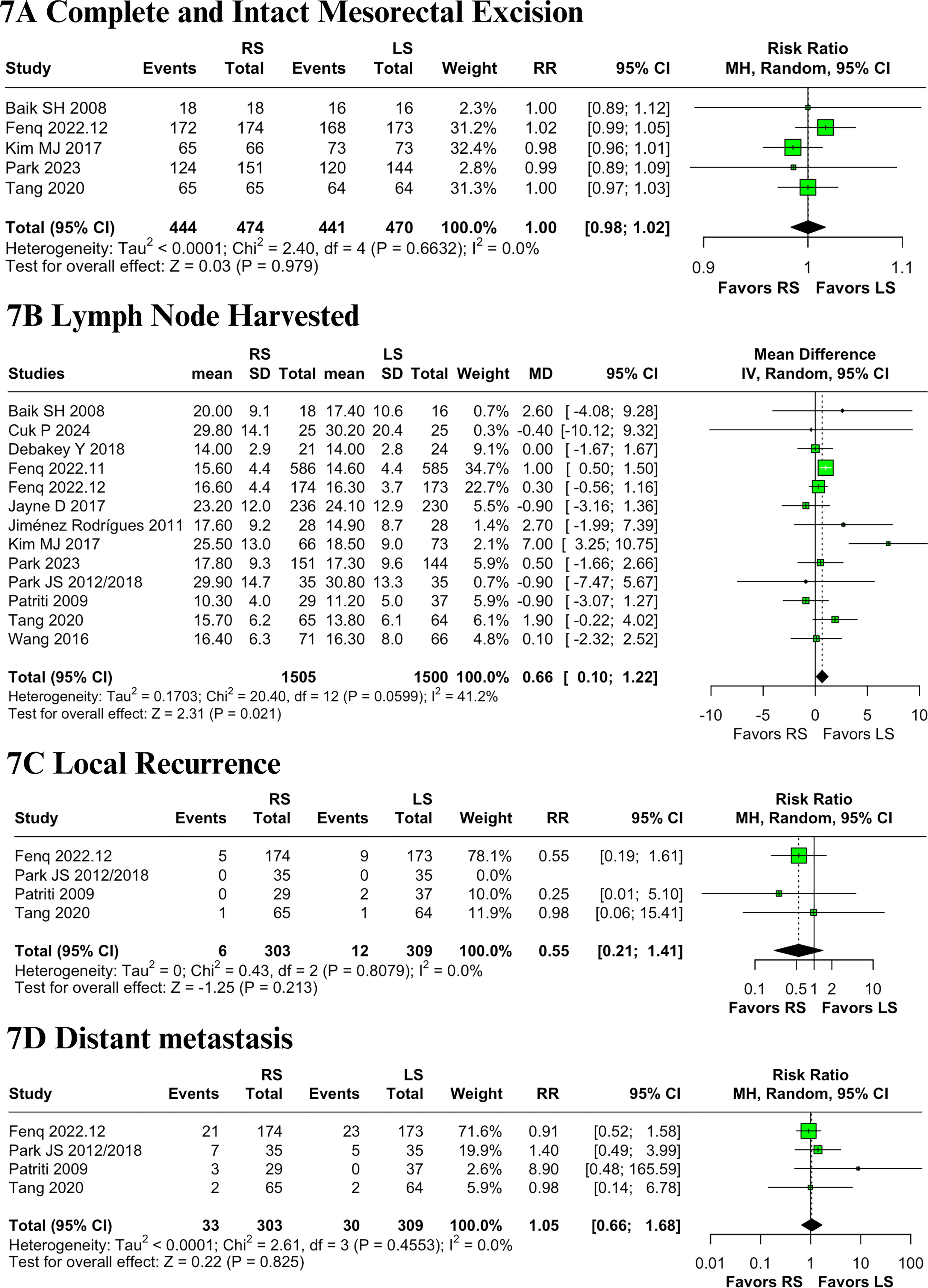
Pathology specimen outcomes and recurrence
RS was associated with more favorable pathological outcomes in two domains. Specifically, RS resulted in a significantly lower rate of +CRM compared with LS (RR = 0.65; 95% CI: 0.46–0.93; P = .017; I2 = 0%; Fig. 6B) and a greater number of lymph nodes retrieved (MD = +0.66; 95% CI: 0.10–1.22; P = .021; I2 = 41.2%; Fig. 7B), 3–16 with the latter showing moderate heterogeneity. No significant differences were observed between groups in distal resection margin length (MD = +0.46 mm; 95% CI: −0.03 to 0.95; P = .066; I2 = 90.6%; Fig. 6C),3,4,7–11,13,15,16 surgical specimen perforation (RR = .86; 95% CI: 0.37–2.03; P = .735; I2 = 0%; Fig. 6D),5,6,12,16 or the integrity of mesorectal excision (RR = 1.00; 95% CI: 0.98–1.02; P = .979; I2 = 0%; Fig. 7A).3,6,13,15,16 Regarding oncologic outcomes, there were no statistically significant differences between RS and LS in rates of local recurrence (RR = 0.55; 95% CI: 0.21–1.41; P = .213; I2 = 0%; Fig. 7C) or distant metastasis (RR = 1.05; 95% CI: 0.66–1.68; P = .825; I2 = 0%; Fig. 7D).6,7,9,10,15
Forest plots comparing robotic and laparoscopic approaches for colorectal cancer:
Sensitivity analyses
Baujat plot analyses were used to identify studies contributing most to heterogeneity. For intraoperative blood loss, VAS 1-day, and VAS 5-day, the study by Kim et al. was the primary driver of heterogeneity. 16 Nonetheless, its exclusion did not significantly impact the overall estimates, which remained consistent across analyses (Supplementary Figs. S1–S6). Regarding overall postoperative complications, Feng et al. contributed the most to heterogeneity. 6 The leave-one-out sensitivity analysis confirmed that removing this study did not alter the pooled result (Supplementary Figs. S7 and Figs. S8). Similarly, Kim et al. were identified as the major source of heterogeneity for operative time. 16 Omitting this trial from the analysis yielded similar results, indicating robustness. (Supplementary Figs. S9 and Figs. S10). For outcomes related to GI recovery and hospital stay, the studies by Feng et al. and Cuk et al. were identified as principal contributors to heterogeneity (Supplementary Figs. S11–S18).6,14 After removing these studies, the pooled results for hospital stay, time to oral intake, and time to first stool remained unchanged (Supplementary Figs. S12, Figs. S16, and Figs. S18). However, for time to first flatus, exclusion of Feng et al. shifted the result in favor of RS (MD = −0.13; 95% CI: −0.24 to −0.01; I2 = 0%) (Supplementary Fig. S14). 6 Finally, for distal margin and number of lymph nodes retrieved, Kim et al. were again identified as the main source of heterogeneity.16 Their removal in sensitivity analyses did not alter the direction or statistical significance of the pooled estimates (Supplementary Figs. S19–S22).
Trial sequential analysis
The TSA plots are presented in Supplementary Figures S23–S46. For the outcome of conversion to open surgery, TSA demonstrated a definitive benefit with RS. The cumulative Z-curve crossed both the conventional significance boundary and the trial sequential monitoring boundary and also reached the RIS of 1592 patients, confirming a statistically significant effect with minimal risk of random error (Supplementary Fig. S23). Likewise, when operative time was assessed, the cumulative Z-curve surpassed the traditional significance threshold and achieved the RIS of 1360 participants, consistently indicating a benefit for LS. These results indicate a reliable and robust effect, suggesting that future studies are unlikely to change this conclusion (Supplementary Fig. S34). For several secondary outcomes, including intraoperative blood loss, intraoperative complications, overall complications, reoperation, readmission, time to oral intake, time to first flatus, 30-day mortality, number of lymph nodes harvested, and local recurrence, the cumulative Z-curves did not cross either the conventional significance threshold or the trial sequential monitoring boundary nor did they reach the RIS. These findings indicate that the current evidence is inconclusive and underscore the need for further high-quality RCTs. In contrast, outcomes such as time to first stool, positive CRM, and distal resection margin demonstrated Z-curve crossings of the conventional significance boundary. However, none reached the RIS, suggesting possible differences between RS and LS, but with insufficient statistical certainty to support definitive conclusions. Finally, for outcomes such as early postoperative pain (VAS scores), anastomotic leakage, Clavien-Dindo grade ≥ III complications, length of hospital stay, specimen perforation, completeness of mesorectal excision, and distant metastasis, TSA could not be formally interpreted due to an insufficient amount of accrued data, representing <5% of the RIS. Therefore, these results should be interpreted with caution, as the current evidence is markedly underpowered to draw reliable conclusions.
Quality assessment and certainty
An overview of the study-specific risk-of-bias assessments conducted in this meta-analysis is provided in Figure 8. All trials were evaluated using the RoB 2 tool (Risk of Bias 2, the revised tool for assessing risk of bias in randomized trials). Of the 14 studies, nine were deemed to have low risk of bias, three were classified as high risk, and two raised some concerns regarding methodological quality.5,6,9,10,12–16 Among the two studies with “some concerns,” limitations were primarily observed in the randomization process and in the selection of reported outcomes,4,8 suggesting possible flaws in sequence generation or allocation concealment, as well as potential selective reporting. The three trials rated as “high risk” demonstrated issues across multiple domains, including deficiencies in randomization, substantial missing outcome data, and concerns regarding outcome measurement.3,7,11 Notably, the study by Wang et al. was also judged as high risk in the domain related to selective reporting, due to the absence of a prespecified protocol or clearly defined outcomes. 11
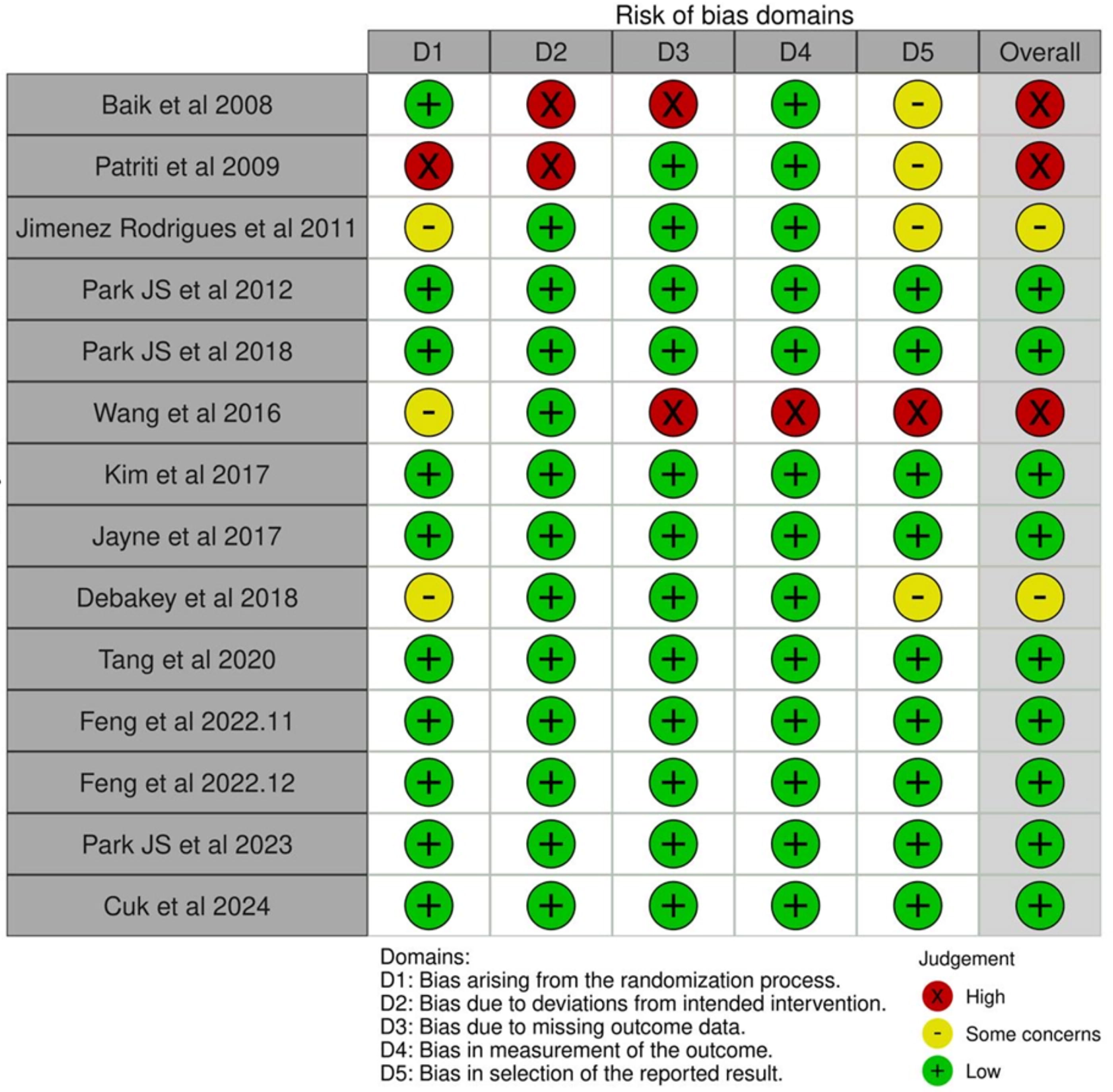
Critical appraisal of RCTs according to the Cochrane Collaboration’s tool for assessing risk of bias (RoB 2).
The GRADE evaluation revealed high certainty of evidence for several key outcomes, including conversion to open surgery, intraoperative complications, anastomotic leakage, severe postoperative complications (Clavien-Dindo grade ≥ III), 30-day mortality, CRM positivity, specimen perforation, complete mesorectal excision, and distant metastasis.
Moderate certainty was assigned to outcomes such as intraoperative blood loss, overall complications, reoperation, hospital readmission, postoperative pain (VAS scores on days 1, 2, and 5), time to first stool, distal resection margin, lymph node yield, and local recurrence. Low certainty ratings were assigned to operative time, return to oral intake, initial flatus passage, and duration of hospitalization. Full details of the GRADE assessments are available in Supplementary Table S2.
Publication bias was evaluated using funnel plots (Supplementary Figs. S47–S53) and Egger’s regression test (Supplementary Table S3). Evidence of small-study effects was detected for operative time, as indicated by visible asymmetry in the funnel plot and a statistically significant Egger’s test result (t = 2.66; df = 11; P = .0221; bias estimate = 5.15; SE = 1.9319). For all other outcomes, funnel plots appeared symmetric, and Egger’s test yielded nonsignificant results (P > .5), indicating no substantial evidence of publication bias.
Discussion
In this systematic review and meta-analysis, which included 14 RCTs comprising 2867 patients undergoing surgical treatment for colorectal cancer, the RS group was associated with lower rates of conversion to open surgery, shorter time to first flatus (after sensitivity analysis), shorter time to first stool, lower rates of positive CRM, and a higher number of lymph nodes harvested. However, RS was associated with longer operative time compared with LS. No significant differences were observed between the groups in rates of intraoperative blood loss, intraoperative complications, postoperative pain (VAS 1-day, VAS 2-day, and VAS 5-day), overall postoperative complications, anastomotic leakage, severe complications (Clavien-Dindo grade ≥ III), reoperation, readmission, time to oral intake, length of hospital stay, 30-day mortality, distal resection margin, specimen perforation, completeness and integrity of mesorectal excision, local recurrence, or distant metastasis.
Robotic-assisted surgery offers well-documented technical advantages, including advanced instrument articulation with seven degrees of motion, enhanced three-dimensional visualization, stable camera control, and improved surgeon ergonomics.3,6–9,11–16 Such capabilities contribute to greater operative precision, facilitating meticulous dissection in anatomically restricted regions.3,6–9,11–16 While intraoperative complication rates were similar between groups, the robotic platform may offer superior control when such events occur. Factors known to contribute to conversion to open surgery, such as technical complexity, prior abdominal operations, and intraoperative adverse events, may be better managed through the precision offered by RS.3–10,12–16 Supporting this interpretation, Laks et al. reported higher conversion rates in the LS group compared with RS (23.1% vs. 6.8%). 34 Likewise, Wang et al. found a 0% conversion rate in robotic rectal surgeries versus 2.5% in the laparoscopic cohort. 35 Together, these data align with our findings and reinforce the potential of the robotic approach in minimizing conversion rates.
Faster GI recovery was also observed in the RS group, particularly regarding time to first flatus and stool passage.3–16 Although both approaches are minimally invasive and inherently promote better postoperative bowel function, robotic platforms may offer additional benefits by minimizing unnecessary manipulation of nontarget bowel loops, thereby reducing local irritation and enhancing recovery.3–16 This interpretation is supported by TengTeng et al., who conducted a prospective study with 102 patients undergoing surgery for mid or low rectal cancer. The authors reported a significantly shorter time to first flatus in the RS (35.1 ± 9.4 hours) compared with the LS (40.7 ± 1.9 hours), as well as earlier initiation of oral intake (2.1 ± 0.8 vs. 2.9 ± 0.4 days). 36 Similarly, Li et al. (2023) found that RS was associated with earlier flatus passage (P = .050) and a shorter time to liquid diet initiation (P = .040) among patients without ileostomy. 37 Yamanashi et al. also described faster progression to soft diet following robotic procedures. 38 On the contrary, Serin et al. reported no significant difference between the two techniques, suggesting that the extent of this advantage may depend on patient-related factors and variations in perioperative management protocols. 39
RS has also been linked to improved quality of TME, potentially reducing CRM involvement and local recurrence due to enhanced precision of dissection. TengTeng et al. proposed this relationship, although no significant differences in CRM or recurrence were found between RS and LS. 37 Similarly, Aliyev et al. reported CRM involvement in 10.9% of patients undergoing LS and 8.3% of those undergoing RS, without reaching statistical significance. 40 Studies by Wang et al. and Laks et al. also failed to identify meaningful differences in margin status between the two techniques.34,35 In contrast to these individual studies, our meta-analysis demonstrated a significantly lower rate of positive CRM in the robotic group. This suggests that robotic-assisted procedures may provide superior preservation of the mesorectal envelope, which could lead to better oncologic control. However, despite this finding, we did not observe differences in either local or distant recurrence between the two surgical approaches.
Lymph node yield, a key indicator of oncologic adequacy in colorectal cancer surgery, was found to be higher in the robotic group in our pooled analysis. Chen et al. observed a significantly greater number of lymph nodes retrieved with RS compared with laparoscopy (27.6 ± 12.5 vs. 24.4 ± 9.2; P = .028), while TengTeng et al. reported a similar pattern, with median values of 23 ± 6 in the RS group versus 15 ± 4 in the LS group.36,41 On the contrary, some studies, including those by Yamanashi, Laks, and Mathew, did not demonstrate statistically significant differences in lymph node harvest between the two approaches.34,38,42 Despite these discrepancies, the aggregated evidence points to a potential advantage of RS in enabling more thorough lymphadenectomy. Our meta-analysis supports this interpretation, showing a higher lymph node yield associated with robotic-assisted procedures.
Operative time remains a relevant consideration when comparing robotic and laparoscopic techniques. 43 Initially, the longer durations observed with robotic procedures were largely attributed to docking processes and the surgical learning curve associated with the platform. 43 Despite technological advancements and increased familiarity, extended operative times continue to be reported in recent literature.3–16 Multiple studies, including those by TengTeng et al., Aliyev et al., Li et al., Huang et al., Tagliabue et al., and Hannan et al., consistently identified longer operative durations for RS in both TME and RC procedures.36,37,40,44–46 Our findings corroborate this trend. Conversely, no significant difference in operative time between RS and LS was reported by Wang et al., Yamanashi et al., and Laks et al.34,35,38 Similarly, Chen et al. and Srinath et al. found comparable operative times between approaches for RC specifically.41,47 It is important to note that although robotic procedures tend to require more time, this has not been associated with increased rates of postoperative complications, as shown by our meta-analysis and several other reports.3–16 While longer operative times may contribute to greater procedural costs, they appear not to adversely affect clinical outcomes. With ongoing improvements in robotic systems, streamlined docking workflows, and wider adoption in clinical practice, this time differential may diminish in the coming years. 48 Regardless of procedural type, robotic-assisted surgery has remained consistently more costly. An initial estimated cost difference of ∼$3000 in 2023 has risen to over $3200 when adjusted for inflation to 2025 using U.S. economic indices. 49
This study presents several limitations. First, although the analysis included 2867 patients across 14 RCTs, the included studies showed variability in surgical technique, surgeon experience, and institutional protocols, which may have influenced some outcomes and contributed to clinical heterogeneity. Second, several endpoints demonstrated high statistical heterogeneity, such as operative time, intraoperative blood loss, and GI recovery, despite sensitivity analyses and the exclusion of influential studies identified through Baujat plots and leave-one-out analysis. Third, long-term outcomes such as disease-free survival and overall survival were not consistently reported across studies, limiting the assessment of oncologic efficacy. Fourth, cost data were not directly reported by the included trials and were inferred from external sources, limiting the precision of economic conclusions. Fifth, the majority of procedures across the included trials were conducted in high-volume centers by surgeons with substantial experience. As a result, the findings may not be fully generalizable to settings with lower surgical volumes or to teams with limited proficiency in robotic or laparoscopic colorectal techniques. Last, although most outcomes were rated as high or moderate certainty by the GRADE approach, a few key endpoints, such as operative time, GI recovery, and hospital stay, were graded as low certainty, reflecting potential imprecision or inconsistency in the data. These limitations underscore the need for future high-quality, multicenter trials with standardized reporting to refine the comparative effectiveness of robotic and laparoscopic approaches in colorectal cancer surgery.
Conclusions
In this systematic review and meta-analysis, which included 14 RCTs comprising 2867 patients undergoing surgical treatment for colorectal cancer, the RS group was associated with lower rates of conversion to open surgery, shorter time to first flatus (after sensitivity analysis), shorter time to first stool, lower rates of positive CRM, and a higher number of lymph nodes harvested. However, RS was also associated with longer operative time compared with LS. No significant differences were observed between the groups in intraoperative blood loss, intraoperative complications, postoperative pain (VAS day 1, 2, and 5), overall postoperative complications, anastomotic leakage, severe complications (Clavien-Dindo grade ≥ III), reoperation, readmission, time to oral intake, length of hospital stay, 30-day mortality, distal resection margin, specimen perforation, completeness and integrity of mesorectal excision, local recurrence, or distant metastasis.
Authors’ Contributions
B.F.P.: Conception and design, data acquisition, data analysis, data interpretation, drafting and editing the article, and revising it critically for important intellectual content. L.E.B.M.A.: Conception and design, data acquisition, data analysis, and data interpretation. G.L.B.: Data acquisition, data analysis, data interpretation, and drafting and editing the article. L.M.D.: Data acquisition, data analysis, data interpretation, and drafting and editing the article. L.S.S.P.G.: Data acquisition, data analysis, and data interpretation. S.M.P.F.: Conception and design, drafting and editing the article, and revising it critically for important intellectual content. F.B.F.: Conception and design, drafting and editing the article, and revising it critically for important intellectual content. All authors approved the final version of the article, including the authorship list.
Disclosure Statement
F.B.F. serves as a speaker for Janssen Brazil, while the remaining authors declare no relevant conflicts of interest. All authors affirm their responsibility for the accuracy, integrity, and impartiality of the data presented and the analyses discussed. This article contains limited and necessary textual similarity with previous works by the authors, particularly within the section “Methods,” where the use of standardized language is critical to ensure clarity, consistency, and reproducibility. Additionally, some overlap with the original RCTs included in this meta-analysis is expected, as methodological descriptions and reported outcomes must be accurately represented to uphold scientific rigor. Importantly, this study offers a new and comprehensive synthesis of RCTs comparing robotic and LS in colorectal cancer. It includes original statistical analyses, TSA, and interpretation not previously published, thereby advancing current understanding in the field. The limited textual similarity observed is justified by methodological rigor and clarity and does not represent redundant publication. All prior works and included studies are appropriately cited, and the article adheres fully to the COPE guidelines on acceptable text recycling. Any overlap is justified in the interest of scientific transparency and reproducibility.