
Abstract
Objective:
To identify the safest and most effective knot-tying sequences for cruroplasty after gastric sleeve surgery, aiming to reduce recurrence risk.
Materials and Methods:
A total of 38 knot-tying sequences were tested using a dynamometer and nonabsorbable sutures. These were divided into four groups: Silk 0 (8 sequences), Silk 2/0 (12), Nylon 1 (12), and Polypropylene 2/0 (14). Each sequence was randomly selected and evaluated based on the average tensile strength of 10 tied knots.
Results:
For Silk 2/0, the strongest sequences were H3H2a (46.39 N) and H2H1aH1aH1aH1a (45.89 N); the weakest were SSbSb (22.28 N) and SSbSbSb (24.18 N). For Silk 0, H3H2a (72.44 N) and H3H2s (70.48 N) were most resistant, while H1H1sH1sH1sH1s (56.6 N) had the lowest strength. With Nylon 1, H2H1sH1sH1sH1sH1s and H2H1aH1aH1aH1aH1aH1a had the highest strengths; SSbSbSb (29.38 N) was weakest. Polypropylene 2/0 sequences showed consistent strength, with H2H1aH1aH1aH1a (48.91 N) being the strongest.
Conclusions:
For Silks 0 and 2/0, at least three half-knots (H1H1H1) are recommended. Starting with a double knot (H2) offers no added benefit. Slip knots should include a minimum of five throws. For Nylon 1, six-throw sequences are optimal; fewer than four throws are not recommended. Polypropylene 2/0 showed uniform performance across sequences. Knot symmetry did not significantly affect strength in any group. All recommended sequences exceed the 43 N threshold needed to prevent cruroplasty dehiscence under normal intra-abdominal pressures.
Introduction
Cruroplasty dehiscence represents a significant problem in the treatment of patients with hiatal hernia. This issue gains greater importance in patients undergoing gastric sleeve surgery, as this procedure alone is associated with the presence of gastroesophageal reflux,1–3 which could exacerbate reflux symptoms and negatively impact the patient’s quality of life.
Among the factors associated with cruroplasty dehiscence are inadequate suturing technique and increased intra-abdominal pressure.4,5 Therefore, it is essential to perform secure knots capable of withstanding elevated intra-abdominal pressure. This can be achieved by using appropriate suture material and caliber, as well as employing a knotting sequence that does not slip and can resist sustained increases in intra-abdominal pressure.
The suture material frequently used in cruroplasty is nonabsorbable sutures of varying calibers, typically 2/0 and larger. Currently, there are no studies investigating an adequate knotting sequence with nonabsorbable sutures that can resist increased intra-abdominal pressure. Abdominal hypertension is considered to start at pressures between 12 and 15 mmHg. 6 For these intra-abdominal pressure values, the tensile strength required for the suture material should range between 34.68 and 43.35 N (considering a peritoneal surface area of 1.7 m2). This raises the question of whether the current surgical technique for cruroplasty is sufficient to withstand increased intra-abdominal pressure and thereby prevent dehiscence. Thus, knotting sequences performed with nonabsorbable sutures should resist forces above 43 N to reduce the likelihood of recurrence.
Over the years of a surgeon’s training, various methods of performing surgical knots are taught, many of which lack scientific evidence. Nevertheless, this knowledge is passed from one generation to the next. In recent years, publications have demonstrated, in laboratory settings, the correct knotting sequences and the horizontal and vertical combinations required for a knot to be considered secure. In 2017, Kondo W and colleagues introduced concepts of single-handed and two-handed knotting, clockwise and counterclockwise rotation of the needle holder, as well as symmetrical and asymmetrical knots, half-knots, and sliding knots. Most importantly, they introduced the concept of a blocking sequence (the knotting sequence necessary to prevent a surgical knot from coming undone or slipping). 7 In 2018, Romeo A and colleagues published about the safest knotting sequences using a dynamometer to quantify knot security. 8
For a surgical knot to have good tensile strength, it fundamentally depends on two factors: the type of suture material used and the execution of a secure knot 9 (i.e., the correct knotting sequence). Suture can be defined as a strand of a specific material used to ligate blood vessels and approximate tissues, facilitating the healing process. 3
Suture materials are classified into absorbable and nonabsorbable categories. Absorbable sutures can be either animal-derived or synthetic. Animal-derived absorbable sutures include simple catgut and chromic catgut, while synthetic absorbable sutures include polyglycolic acid, Polyglactin 910, Glycomer 631, Polyglyconate, Poliglecaprone 25, and Polydioxanone. Nonabsorbable sutures can be of plant, animal, mineral, or synthetic origin. Plant-derived sutures include cotton and linen; silk is animal-derived, stainless steel is mineral, and synthetic options include nylon, polyester, and polypropylene.9,10
In 2023, Romeo A and colleagues reported the effect of suture diameter and type on the safety of surgical knots. However, their tests were conducted only with absorbable suture materials such as Polyglactin 910, Poliglecaprone 25, and Polydioxanone.7–9 Until today, no studies have evaluated knot safety with nonabsorbable suture materials.
The objective of the present study is to determine safe knotting sequences using nonabsorbable sutures to perform cruroplasty after gastric sleeve surgery and prevent recurrence.
Materials and Methods
Terminology
The safety of a surgical knot is defined as a combination of knots that does not come undone and does not slip before the suture line breaks, and if it does slip, it does not exceed 3 mm. 8 Since 2017, Romeo A and colleagues have established the foundation for a new theory of surgical knotting with their publications. From these publications, different terminologies have been introduced to refer to surgical knotting techniques.
There are two fundamental types of surgical knotting: the half-knot (denoted as “H”) and the sliding knot or half-hitch (denoted as “S”). A half-knot and a half-hitch can be combined in horizontal and vertical sequences. A horizontal turn of the thread is denoted as “H1,” two turns as “H2,” and three turns as “H3.” A vertical combination is a sequence of half-knots stacked on top of each other (e.g., if the base knot or first knot has two horizontal turns, the next knot has one horizontal turn, and the subsequent knot also has one horizontal turn, it is denoted as H2H1H1). The concepts of symmetry and asymmetry in a surgical knot are introduced, as shown in Figure 1. If the second half-knot (one horizontal turn) is symmetrical with respect to the first (two horizontal turns), it is denoted as H2H1s; if the second half-knot is asymmetrical with respect to the first, it is denoted as H2H1a.7,8,11–15

A half-hitch is a sliding knot where one end of the thread forms an axis, and the other end is tied around this axis. If a single knot is made around the axis, it is denoted as “S”; if two knots are made, it is denoted as “SS.” Previous studies with absorbable sutures determined that to create a blocking sequence in sliding knots, the axis must be reversed, meaning the active thread becomes the passive one (axis), forming a blocking half-hitch denoted as “Sb.” Vertical combinations of half-hitches can be formed as shown in Figure 2.
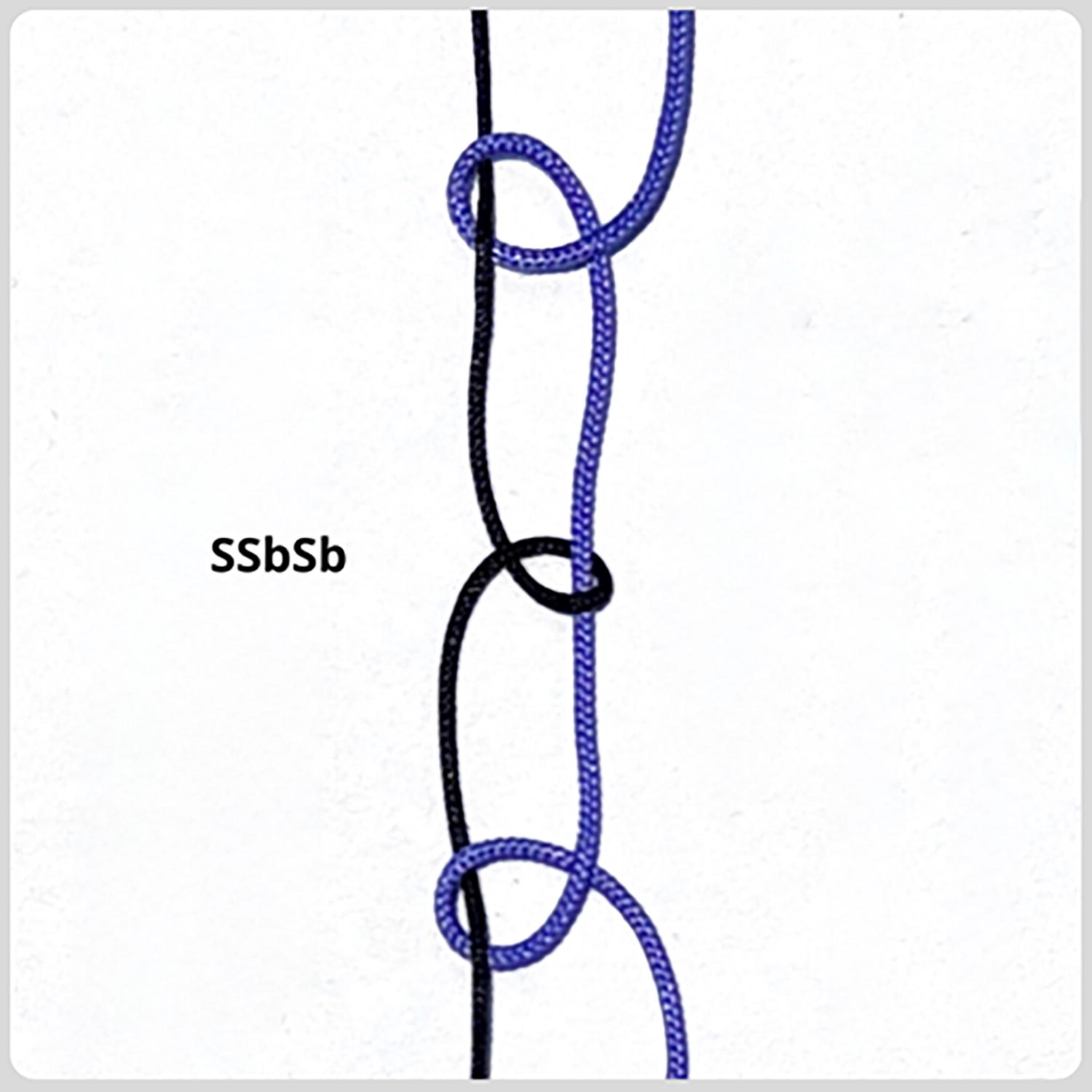
Vertical combination of a slip knot: You can see how the tying axis alternates, forming two blocking sequences (SSbSb).
Knotting sequences studied and suture materials
This study examines nonabsorbable suture materials (Silk 2/0, Silk 0, Nylon 1, Polypropylene 2/0) and the following knotting sequences:
Silk knotting sequence: H1H1aH1aH1aH1a Silk knotting sequence: H1H1sH1sH1sH1s Silk knotting sequence: H1H1aH1aH1a Silk knotting sequence: H1H1sH1sH1s Silk knotting sequence: H1H1aH1a Silk knotting sequence: H1H1sH1s Silk knotting sequence: SSbSbSbSb Silk knotting sequence: SSbSbSb Silk knotting sequence: SSbSb Nylon knotting sequence: H2H1aH1aH1aH1aH1aH1a Nylon knotting sequence: H2H1sH1sH1sH1sH1sH1s Nylon knotting sequence: H2H1aH1aH1aH1aH1a Nylon knotting sequence: H2H1sH1sH1sH1sH1s Nylon knotting sequence: H2H1aH1aH1aH1a Nylon knotting sequence: H2H1sH1sH1sH1s Nylon knotting sequence: H2H1aH1aH1a Nylon knotting sequence: H2H1sH1sH1s Nylon knotting sequence: H2H1aH1a Nylon knotting sequence: H2H1sH1s Nylon knotting sequence: SSbSbSbSb Nylon knotting sequence: SSbSbSb Polypropylene knotting sequence: H2H1aH1aH1aH1a Polypropylene knotting sequence: H2H1sH1sH1sH1s Polypropylene knotting sequence: H2H1aH1aH1a Polypropylene knotting sequence: H2H1sH1sH1s Polypropylene knotting sequence: H2H1aH1a Polypropylene knotting sequence: H2H1sH1s Polypropylene knotting sequence: SSbSbSbSb Polypropylene knotting sequence: SSbSbSb Polypropylene knotting sequence: H1H1aH1aH1aH1a Polypropylene knotting sequence: H1H1sH1sH1sH1s Polypropylene knotting sequence: H1H1aH1aH1a Polypropylene knotting sequence: H1H1sH1sH1s Polypropylene knotting sequence: H1H1aH1a Polypropylene knotting sequence: H1H1sH1s Silk knotting sequence: H3H2a Silk knotting sequence: H3H2s Silk knotting sequence: H2H1aH1aH1aH1a
Methodology
This study employs a quantitative and experimental design. The studied population consists of 38 knotting sequences using nonabsorbable suture materials (with 10 repetitions for each sequence). Appropriate suture materials were selected, and the knotting sequences were organized into blocks. The total number of surgical knots (470) was included in the study.
All surgical knots were performed by the same individual (Y.T.L.), a senior general surgeon, and all knotting procedures were supervised by one of the authors (W.K.). The knot combinations were divided into four blocks: Silk 0 (8 sequences), Silk 2/0 (12 sequences), Nylon 1 (12 sequences), and Polypropylene 2/0 (14 sequences). The knotting sequences were randomized using computer-based random numbers (Excel). Ten surgical knots were made for each studied sequence.
Knotting technique and knot quality testing with dynamometer
Surgical knotting was performed following the Romeo’s Gladiator Rule 8 using second-generation laparoscopic simulators ETX A2 EVE (Prodelphus Surgical Simulators, Olinda, Pernambuco, Brazil) with Karl Storz Full HD imaging system (IMAGE 1 HUB HD and a 3-chip HD camera head) and two Karl Storz needle holders (KARL STORZ KOH Macro Needle Holder). A digital dynamometer IP90-DI (Impac Comercial e Tecnologia Ltda, Sao Paulo, Brazil) was tested at a speed of 200 mm/minutes. Threads of 20 cm in length were used, and the knotting sequences were performed around a 15-mm diameter plastic tube. After completing each knot, the suture threads were cut to 10 mm to check for slippage, and then the loops were placed on the hooks of the digital dynamometer. The tensile strength values of each knot were recorded until breakage, measured in Newtons (kg × m/s2), using a data collection form.
Statistical analysis
In the descriptive analysis, the mean and standard deviation of the strength of the surgical knots were estimated according to suture material and knotting sequence. An analysis of variance test was applied to compare the strength of the knotting sequences for each type of suture material. The analyses were conducted using STATA MP version 17, with values of P < .05 considered significant.
Results
For Silk 2/0, the knotting sequences H3H2a and H2H1aH1aH1aH1a had the highest average strengths (46.39 and 45.89 N); in contrast, the sequences SSbSb and SSbSbSb showed the lowest strength values within the block (22.28 and 24.18 N), reaching nearly half the strength of the most resistant knots (Table 1).
Results of Mechanical Tests for Surgical Knot Breakage, According to Suture Material
Groups 9 and 10 for Nylon 1 were excluded because they opened and slipped to 0 N of force during the experiment.
SD, standard deviation.
For Silk 0, the same table shows that the knotting sequence with the highest average strength was H3H2a (72.44 N), followed by H3H2s (70.48 N); conversely, the knotting sequences with the lowest average strength for this material were H1H1sH1sH1sH1s and H1H1sH1sH1s (56.6 and 58.45 N).
Regarding Nylon 1, the highest observed average strengths were for the sequences H2H1sH1sH1sH1sH1s and H2H1aH1aH1aH1aH1aH1a; while the lowest strength values were for the groups SSbSbSb with 29.38 N and H2H1aH1aH1a with 57.7 N (Table 1). Two knotting sequences were excluded from the study because they either opened or slipped to 0 N of force: H2H1aH1a and H2H1sH1s.
For Polypropylene 2/0, Table 1 shows average strengths that do not exceed 49 N, with the highest values among the sequences H2H1aH1aH1aH1a and H2H1aH1aH1a (48.91 and 47.05 N), while the lowest values were from the sequences SSbSbSb, H1H1sH1s, and H1H1aH1a (37.13, 37.96, and 38.59 N).
At the inferential level, 12 groups with different knot types for the Silk 2/0 material were compared, and significant differences were found between group 10 and groups 1 through 9, as well as with group 12. The same results were observed for group 11 (Fig. 3).
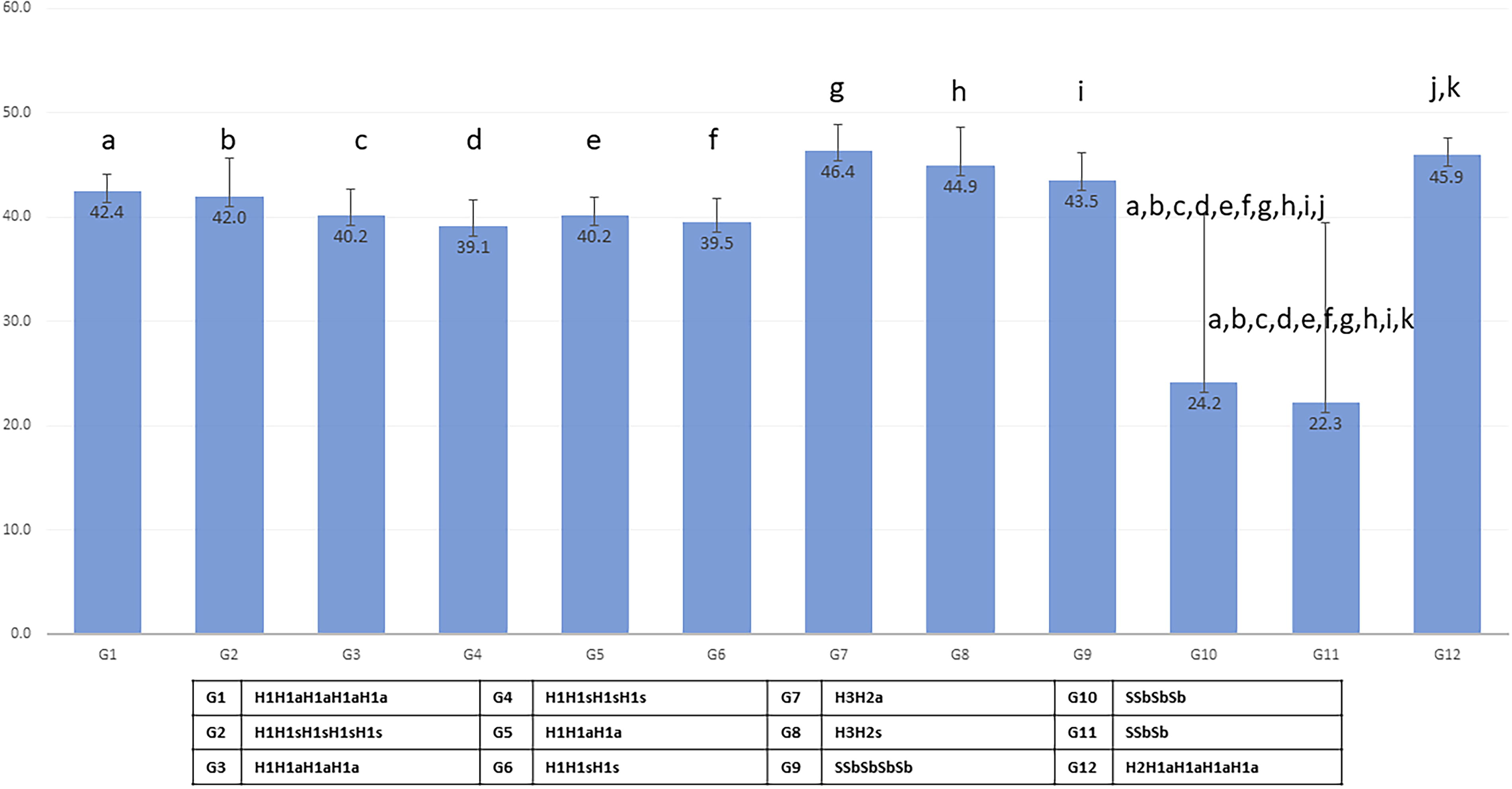
Effect of 12 knot sequences on tensile strength (newtons) in case of Silk 2/0 suture material breakage. The same letters in charts mean significant differences between groups.
Regarding the Silk 0 material, eight groups with different knot configurations were compared, and it was found that group 6 showed a significant difference only with group 2. Meanwhile, groups 7 and 8 (independently) showed significant differences compared with groups 1 through 5 (Fig. 4).

Effect of eight knot sequences on tensile strength (newtons) in the case of breakage of Silk 0 suture material. The same letters in charts mean significant differences between groups.
Twelve groups with different knot sequences using Nylon 1 material were also compared. It was found that both group 7 and group 8 had significant differences compared with groups 1 through 6 and groups 11 and 12. Group 11 showed differences with groups 1, 3, 4, 7, 8, and 12 (Fig. 5).

Effect of 12 knot sequences on tensile strength (newtons) in the case of breakage of Nylon 1 suture material. The same letters in charts mean significant differences between groups.
Finally, for Polypropylene 2/0, 14 different knot sequences were compared, and it was found that group 5 showed significantly different values compared with group 1. Additionally, group 8 had significant differences with groups 1 through 6 and groups 9, 11, and 12. Group 9 showed differences with groups 13 and 14, while group 10 had differences with group 1. Group 11 also showed significant differences with groups 12, 13, and 14. Group 12 had significant differences with group 1, and group 13 showed differences with groups 1 through 4 and groups 6, 9, and 14. Finally, group 14 also had significant differences with groups 1 through 4 and groups 6, 9, and 13 (Fig. 6).

Effect of 14 knot sequences on tensile strength (newtons) in the case of breakage of Polypropylene 2/0 suture material. The same letters in charts mean significant differences between groups.
Discussion
The study of the safety of surgical knots is not a new topic. Various surgical specialties, such as orthopedics, gynecology, and general surgery, have investigated the safety of surgical knots, linking it to the execution of square knots and the number of turns. There are discrepancies regarding the number of turns that provide greater safety for knots, as well as between safety and the type of suture material used. For example, Kim SH et al., in 2005, studied the safety of sliding knots in arthroscopy using nonabsorbable monofilament suture 2/0. They determined that in all cases where sliding knots are used, two to three additional half-knots should also be performed to ensure knot security. 16 In the present study, we used Polypropylene 2/0 and Silk 2/0, but the types of knots studied were different since sliding knots were not examined. However, it was found that the tensile strength of polypropylene and silk is lower, likely due to the type of material used. In arthroscopy knot studies, Ethibond suture with tensile strength between 80 and 100 N is used, whereas in this study, the most resistant sequences had an average tensile strength of 46.39 N (sequence H3H2a) for silk and 48.91 N (H2H1aH1aH1aH1a) for polypropylene.
Tidwell JE et al. conducted a study in 2012 at West Virginia University, published in the journal Orthopedics, where they determined the minimum number of turns a surgical knot must have to be considered secure. They used nylon and polypropylene sutures, with knot sequences ranging from three to six symmetrical half-knots (H1s), and the thread diameter was 2/0. In both cases, a minimum of four turns was necessary to prevent the knots from slipping and to withstand 24.5 and 28.5 N, respectively, until thread rupture. 17 In the present study, we examined the same knot sequences for Polypropylene 2/0. Unlike the mentioned study, we found that the sequence of four symmetrical half-knots (H1H1sH1sH1s) had a tensile strength of 42.62 N (SD = 2.73) and that asymmetrical knot sequences had higher tensile strength compared with symmetrical knots (44.94 N for the H1H1aH1aH1a sequence, SD = 3.82). For Nylon, we used a diameter “1” and only sequences starting with a double half-knot (H2), where the tensile strength of the H2H1sH1sH1s sequence was 65.9 N (SD = 4.32).
Marturello DM et al., in 2014, published a study in the journal Veterinary Surgery, examining the resistance of surgical knots with various nonabsorbable and absorbable suture materials. For nonabsorbable sutures, they studied nylon and polypropylene. In all cases, they used knot sequences of three to six symmetrical half-knots (H1s) with a thread diameter of 2/0. This study did not differentiate between suture materials for statistical purposes. It was found that a knot is considered secure when it has an average of five turns, with a mean breaking force of 14.6 N. 15 This differs from our results, where the sequence with four turns (H1H1sH1sH1s) had a tensile strength of 42.62 N (SD = 2.73).
In veterinary surgery, large-caliber sutures (sizes 2 and 3) were studied, where the anchor knot in a continuous suture was found to be superior to a square knot and a surgeon’s knot, as studied by Guillen AM et al. in 2016 and published in the journal Veterinary Surgery. 18 The same researcher published in 2017 in the same journal a study comparing the square knot with the surgeon’s knot using Polyglactin 910 and Polydioxanone sizes 2 and 3. It was determined that six turns at the start of the continuous suture and seven turns at the end are required for secure knotting. Additionally, Polyglactin 910 had more tensile strength than Polydioxanone. 19 The same team published, in 2020, a modified anchor knot with greater tensile strength than the Aberdeen knot, the surgeon’s knot, and the square knot, also using the same suture material. 20 In all cases, absorbable and large-caliber sutures were used. In the present study, we did not use absorbable sutures but did use a large-caliber suture, Nylon “1,” where the knot sequence with the highest tensile strength was six turns (H2H1sH1sH1sH1sH1s) with a value of 103.28 N (SD = 6.05). It is noteworthy that in our study, the knot sequences with five, six, and seven turns did not show statistically significant differences when compared with each other, and all three sequences, both symmetrical and asymmetrical, exhibited good tensile strength. The sequences with four turns showed very irregular behavior when tested for tensile strength, as the knots opened or slipped within a very variable range between 41 and 70 N (no four-turn knot sequence withstood until rupture), and when tested with three turns, the tensile strength was very low, with knots even reaching “0 N,” leading to the decision to stop the experiment at that point.
A study in general surgery published, in 2002, by Amortegui JD et al. in the journal Surgical Endoscopy examined the safety of knots in laparoscopic surgery. They used nonabsorbable braided Polyester 2/0 and performed knot sequences H2H1s, H1H1s, sliding knots without blocking sequences and with blocking sequences. They determined that six turns were necessary for a laparoscopic knot to be secure, with the H1H1sH1sH1sH1sH1s configuration being the most secure with 41.68 N (SD = 10.17). 21 In our study, the knot sequence with the most turns was H1H1sH1sH1sH1s (five turns) using Silk 2/0, which had a tensile strength of 41.99 N (SD = 3.68). It is noteworthy that with this material, there were no statistically significant differences when performing three, four, or five turns, whether symmetrical or asymmetrical knot sequences. The sequences H3H2a, H3H2s, and SSbSbSbSb were also safe. The sliding knot sequences SSbSbSb (four turns) and SSbSb (three turns) had low tensile strength of 24.18 and 22.28 N, respectively, and exhibited very irregular behavior when measured with a dynamometer, as all knots slipped, some even to 0 N.
Van Leeuwen N et al. published a study in 2012 in the Journal of Gynecologic Surgery, where they tested the tensile strength of sliding knots with and without blocking sequences and compared Polyglycolic Acid and Polyglactin 910. The suture diameter was 3/0. The thread with the highest tensile strength was Polyglactin 910, and the best knot sequence was the sliding knot with blocking sequences (five turns), with values ranging between 50 and 60 N (the article does not provide exact average values but includes a graph). 22 In our study, we worked with nonabsorbable and larger diameter suture (2/0), where the same knot sequence SSbSbSbSb had an average tensile strength of 43.49 N (SD = 2.71) for silk and 41.83 N (SD = 3.32) for polypropylene.
Romeo A et al. published in 2023 in the Clinical Medicine Journal, a study where they investigated the tensile strength of Polydioxanone and Polyglactin 910. They found that sliding knots with blocking sequences are superior to half-knots when greater security is required, as well as adding more flexibility. Polydioxanone requires five turns and Polyglactin 910 requires four turns, both sliding knots with blocking sequences, with a suture diameter of 2/0. The average tensile strength was 50 N. 11 In our study with nonabsorbable suture, for Silk 2/0, the sliding knot sequence with blocking sequences (SSbSbSbSb) had a tensile strength of 43.49 N (SD = 2.71), which was higher than all sequences of half-knots of three to five turns. Only the sequences H3H2 and H2H1H1H1H1 (symmetrical and asymmetrical) had higher values than the sliding knot sequence with five turns. For Polypropylene 2/0, the sliding knot sequence with blocking sequences of five turns (SSbSbSbSb) had a tensile strength of 41.83 N (SD = 3.35), which was lower than all half-knot sequences of three, four, and five turns that start with a double knot and also lower than the symmetrical and asymmetrical half-knot sequences of four and five turns. It was only higher than the sliding knot sequences with blocking sequences of four turns (SSbSbSb) and the symmetrical and asymmetrical half-knot sequences of three turns, though these differences were not statistically significant. The only sliding knot sequence whose traction strength showed statistically significant differences was the four-blocked sequence with four turns (SSbSbSb), which also had the lowest value within the study (37.13 N, SD = 6.85).
In 2021, Taysi AE et al. published a study in the Oral Clinical Research journal comparing various suture materials, including polypropylene and silk. The thread diameter was 3/0, and the knotting sequence was H2H1H1H1 (the article does not specify whether the knots were symmetrical or asymmetrical). The average breaking strength for silk was 64.8 N and for polypropylene was 70.4 N. 23 These results differ from those found in our study, as despite using a larger thread diameter (2/0), the traction strength for the same sequence was 45.9 N for silk and 45.99 N for polypropylene.
Two years later, in 2023, Taysi AE et al. also studied the relationship between knot configuration and suture material. This study, published in the Journal of Oral and Maxillofacial Surgery, used nylon and polypropylene as nonabsorbable sutures, with a diameter of 3/0. They found that the H2H1H1 configuration was the most resistant (it is not specified whether the knots were symmetrical or asymmetrical). The highest traction strength was with nylon at 28.6 N, while polypropylene had a traction strength of 24.7 N. 24 In comparison, our study used polypropylene 2/0, and the traction strength for the same knotting sequence was 44.26 N.
Clinical implications
For Silk 2/0, the knotting sequence H2H1aH1aH1aH1a has a traction strength of 45.89 N, which is higher than all sequences of symmetrical and asymmetrical half-knots that start with a simple knot (H1). However, this does not have clinical relevance for the recommendation because there are no statistically significant differences. Additionally, a double knot (H2) made with silk does not fully secure to living tissue. Therefore, it is recommended to use knotting sequences starting with a simple knot, whether symmetrical or asymmetrical, with three to five turns. For sliding knots, it is recommended to use the sequence SSbSbSbSb (five turns with blocking sequences). Sequences with four turns should be avoided due to their uncertain behavior when tested for traction strength with a dynamometer, as these sequences open and slip even at 0 N of force.
For Silk “0,” the knotting sequence H1H1sH1s had the highest traction strength at 65.72 N, which was superior to all sequences of symmetrical and asymmetrical simple half-knots. Although the results were not statistically significant, it is recommended to use this sequence over four- and five-turn half-knot sequences because it uses less foreign material and optimizes operative time. The H3H2a and H3H2s knotting sequences for both silk diameters have higher traction strength values than all other sequences, but this result does not have significant clinical relevance.
For Nylon 1, sequences with three turns (H2H1H1) and sliding knot sequences with four turns should be avoided, as these sequences have very low traction strength, slipping even at 0 N of force. The sequence of symmetrical half-knots with six turns (H2H1sH1sH1sH1sH1s) has higher traction strength, but this result is not statistically significant and lacks clinical relevance.
For Polypropylene 2/0, it is recommended to use knotting sequences with four or five turns, starting with either a double knot (H2) or a simple knot (H1), as these have high traction strength values.
Limitations and strengths
This study has some limitations, such as not including other diameters of the materials used. Another limitation may be that the knots were performed by a single expert surgeon; however, the knots were supervised by another expert surgeon. A strength of the study is that, to our knowledge, it is the first study evaluating the resistance of knots in nonabsorbable suture material. Additionally, another strength is the number of repetitions (n = 10) performed for each knotting sequence with different suture materials.
Conclusions
For Silks 0 and 2/0, it is recommended to use at least three-turn half-knot sequences (H1H1H1). For Silk 2/0, starting a knotting sequence with a double knot (H2) has neither clinical nor statistical relevance. Therefore, any knotting sequence can begin with a simple knot (H1). If using half-hitch, they should be five turns and all with blocking sequences, as resistance to traction is very low with four or fewer turns. For Nylon 1, the six-turn knotting sequence (H2H1sH1sH1sH1sH1s) has higher traction strength than all other knotting sequences, including those with seven turns. Thus, its use is recommended according to the surgeon’s criteria. Sliding knots with four or fewer turns are not recommended due to their very low traction strength. For Polypropylene 2/0, all knotting sequences show very similar and acceptable traction strength, so any of them can be used interchangeably. There is no significant difference between using symmetrical or asymmetrical knots with any of the suture materials studied. The choice of knot symmetry is left to the surgeon’s criteria. For all recommended knotting sequences, cruroplasty dehiscence would be low since, under normal intra-abdominal pressure conditions, it is sufficient for the repair to withstand a force of 43 N.
Footnotes
Acknowledgment
The authors thank Marith Oscco Llacchua, general surgery resident.
Authors’ Contributions
Y.T.L.: Writing, original draft, review, editing, visualization, and supervision. C.L.C. and A.R.: Writing, editing, and visualization. J.P.A.: Writing, review, editing, and visualization. W.K. and A.P.H.: Writing, review, and editing.
Disclosure Statement
Y.T.L., C.L.C., A.R., W.K., J.P.A., and A.P.H. have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.