
Abstract
Abstract
There are controversial views as to whether intratumoral or peritumoral lymphatics play a dominant role in the metastatic process. Most clinical observations originate from studies of colon cancer. Colon contains mucosa and submucosa rich in lymphatics and with high lymph formation rate. This seems to be a prerequisite for easy metastasis of cancer cells to regional lymph nodes. However, there are other tissues as pancreas with a rudimentary lymphatic network where cancer metastasis formation is as intensive as in colon cancer. This contradicts the common notion that intratumor lymphatics play major role in metastases.
We visualized interstitial space and lymphatics in the central and peripheral regions of colon and pancreas tumors using the color stereoscopic lymphography and simultaneously immunohistochemical performed stainings specific for lymphatic and blood endothelial cells. The density of open and compressed lymphatic and blood vessels was measured in the tumor core and edge.
There were very few lymphatics in the colon and pancreas tumor core but numerous minor fluid “lakes” with no visible connection to the peritumoral lymphatics. Lining of “lakes” did not express molecular markers specific for lymphatic endothelial cells. Dense connective tissue surrounding tumor foci did not contain lymphatics. Peritumoral lymphatics were irregularly distributed in both types of tumor and only sporadically contained cells that might be tumor cells. Similar lymphoscintigraphic and histological pictures were seen in colon and pancreas cancer despite of different structure of both tissues. This suggests a uniform reaction of tissues to the growing cancer irrespective of the affected organ.
Introduction
Although there is a large body of evidence that newly visualized lymphatics may facilitate formation of metastases, it remains unclear whether the intratumoral lymphatics participate in transport of detached tumor cells to the lymph nodes. Some studies prove peritumoral neolymphangiogenesis contribution to tumor metastases, however, opposite views exist originating from clinical studies.1,2 The colon intratumoral and peritumoral tissue might be devoid of active lymphangiogenesis and intratumoral lymphatics are frequently collapsed and non-functional. 3 Tissue fluid accumulates in cancer tissue forming interstitial “lakes” not communicating with peritumoral lymphatics. 4 Moreover, there are reports that tumor tissue fluid pressure is high and tumor cell mass and desmoplastic connective tissue compress lymph and blood vessels.5–7 Furthermore, formation of metastases in regional lymph nodes is not related to the density of lymphatics in the drained organs as for example in colon and pancreas. Whereas the former contains a dense network, there are only few interacinar lymphatics in pancreas. 8 However, in both cases cancer metastases to lymph nodes are similar with 56% in patients undergoing pancreatic cancer resection 9 with the same numbers in colon cancer at surgery.
The open question remains whether dynamics of metastases formation depend on organization of the lymphatic network of a given organ modified by cancer humoral factors or are an inherent trait of cancer cells irrespective of organ lymphatics. To answer this question we studied the anatomy of lymphatics in cancer tissue of two morphologically different organs: colon and pancreas.
Identification of lymphatics has been routinely based on immunohistochemical staining of lymphatic endothelial cells. This method does not, however, show the tissue fluid filled tumor interstitial space and the shape of minute lymphatic vessels. We applied an original method for visualization of interstitial space structure and lymphatics in the central and peripheral regions of colon and pancreatic tumor using color stereoscopic lymphography in transparent specimens and in parallel performed immunohistochemical stainings specific for lymphatic and blood endothelial cells. The density of open and compressed lymphatic and blood vessels was measured in the intratumoral areas and at tumor edge. Moreover, the frequency of single tumor cells in intra- and peritumoral lymphatics was measured.
Material and Methods
Patients
Samples of human colon cancer, normal colon, pancreatic cancer and normal pancreatic tissue were obtained from 50 colon and 50 pancreas cancer patients (Table 1). In case of colon this was adenocarcinoma and in pancreas ductal adenocarcinoma, intraductal papillary mucinous and mucinous cystic neoplasm.
Processing of specimens
Tumor containing tissue of a size 5×3 cm was divided into two fragments for color lymphography and immunohistochemistry. One fragment was immediately injected with Patent Blue in chloroform suspension to visualize the structure of interstitial space and lymphatic capillaries. Another fragment was snap-frozen at 70° C, sectioned and stained with monoclonal antibodies. (Table 1)
Color lymphangiography
Briefly, a 3×2 cm fragment of tissue was injected with Paris blue (artist paint) suspension.10,11 One gram of paint was suspended in 20 mL of chloroform (Sigma, St.Louis, USA), mixed for 1 h, then centrifuged for 20 min at 2000 rpm. Filtration through a 0.22 micron bacterial filter followed. A drop of suspension was put on the microscopic glass and checked under light microscope for presence of clumps. The solution should be clear blue. For injection, a glass insulin syringe with 23 gauge needle was used. Plastic syringes undergo dissolving by chloroform. Injection of 1mL lasted for 3 minutes under low pressure. Subsequently, the injected tissue was fixed in 6% formalin for 1 day and dehydrated daily for 6 days, first in 60% ethanol (first day), 70% (second day), 80% (third day), 96% (forth and fifth days) and 100% (sixth day). Then, tissue was placed in methyl salicylate (Sigma, St.Louis, USA)) for 24 h. It was cut into 150–500 micron thick slices. Preservation in methyl salicylate may last for years. Magnification of 100x was a routine. For higher magnifications, specimens were cut thinner (50–100 microns). To discriminate between lymphatics, veins, and arteries of the same size, they were injected through the stumps protruding from the specimens.
In order to further prove that the stained structures were not blood vessels, five-by-five mm thick Paris Blue injected fragments of tissue were snap frozen at 70° C and sectioned for immunohistochemical staining with monoclonal antibodies to LYVE 1 lymphatic endothelial cell hyaluronan receptor and FVIII and CD31 to identify blood endothelial cells.
Immunohistochemistry of tumor specimens
The tumors fragments were fixed in 10 percent formalin for 24 hours at room temperature and embedded in paraffin. Five-micron-thick sections were then incubated with 10 percent normal rabbit serum in phosphate-buffered saline (PBS) solution, followed by treatment with biotinylated mouse anti-human fVIII, CD31 (both Dako, Glostrup, Denmark), LYVE1, podoplanin and prox1 (RELIATech, Wolfenbüttel, Germany) monoclonal antibody and streptoavidin- alkaline phosphatase complex (LSAB 2 Kit AP, DAKO, Glostrup Denmark). Counterstaining was performed with Mayer's hematoxylin.
Quantification of blood and lymphatic vessels
Lymphatic vessel density (LVD) and micro-blood vessel density (MVD) were assessed on histological sections of the cancer as well as in normal tissue distant from the cancer (>5 cm). Presence of vessels in tissue sections was evaluated following staining with monoclonal antibodies as described above. Briefly, LVD and MVD were identified on the cancer sections by screening in three areas in the vicinity of normal tissue (tumor periphery) and three towards the tumor center (tumor core). Additionally MVD and LVD were counted on 3 areas distant from the tumor (normal tissue). The number of vessels was counted within a counting grid at 200× magnification in 3 to 5 consecutive fields in each area. As defined by N. Weidner for the blood and lymphatic vessels count, “any stained endothelial cell or cell cluster separated from another microvessel structure was considered a countable microvessel”. 12 The slides were reviewed independently by three observers (WLO, MS, MG) blinded to clinical details. MVD and LVD are expressed as the mean value of counted microvessels in 3 to 5 evaluated grids.
Cross section area of lymphatic and blood vessels
The cross section area ratio—the ratio of lymph and blood vessel area within the tumor and adjacent colon tissue—to lymphatic and blood vessels area in the normal tissue was counted using a computerized image analysis system (Olympus, Microimage, Japan). The ratio of open vs. closed lymph and blood vessels within the tumor and adjacent colon tissue to lymphatic and blood vessels in the normal tissue was counted using the same software.
The level of compression of lymphatic vessels was assessed by quantification of the aspect ratio—the ratio of maximum to minimum axes of perfused vessels. An aspect ratio of 1 represented a perfect circle. The larger was the aspect ratio, the greater the amount of vessel compression. Aspect ratio data were shown as mean±SD.
Statistical analysis
Statistical analysis was performed by using the Student's t-test and Mann-Whitney U test. Differences were considered to be statistically significant at p<0.05.
Results
Color lymphography of tumor and adjacent tissues
Color lymphangioraphic pictures of the colon tumor center, edge and adjacent tissue were evaluated. At the colon tumor edge and in adjacent tissues lymphatics of various size of lumen were seen (Fig. 1A). On color lymphography, lymphatics surrounding pancreatic tumor foci had a tortuous shape (Fig. 1B). In the tumor center no regular shape lymphatic vessels were seen. Sporadically, small blind fragments of lymphatics of a length of 50–100 microns could be detected. The picture was dominated by multiple oval or round, sometimes irregular shape 10–20 micron diameter structures with density in the “hot places” of 100–200 (Fig.1C). Some tumor fragments showed only blue dye between collagen fibers (Fig. 1D). In specimens stained with Paris Blue and subsequently hematoxilin-eozin lymphatics were identified only in the peritumoral areas.
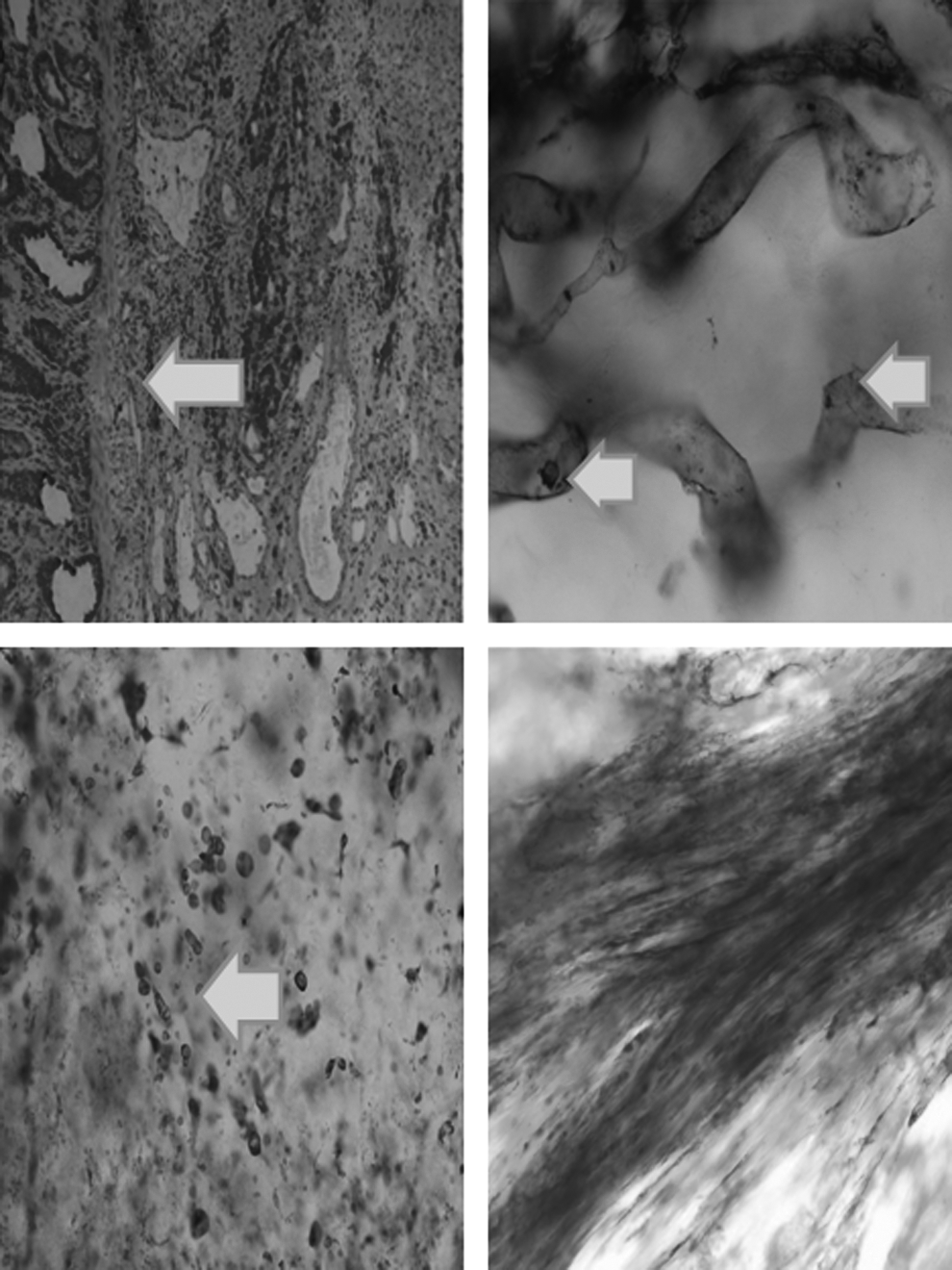
A to D. Colon cancer. A.Submucosa. Red stained peritumoral lymphatics (arrow) and single macrophages. Large cell-lined spaces are dilated veins. LIVE 1, ×100. B. Peritumoral lymphatic with two small tumor cells or lymphocytes (arrows), ×200. C. Intratumoral accumulation of Paris Blue in minute irregular, oval and round spaces most likely containing tissue fluid. Lack of lymphatic structures, ×100. D. Fibrous tissues around a single tumor focus. Paris Blue fills microspaces between collagen bundles, no lymphatics, ×100.
The colon cancer foci were surrounded by fibrous tissue (Fig. 2A). Single peritumoral LYVE 1+ lymphatics were seen (Fig. 2B). Peritumoral lymphatics stained with Paris Blue were dilated and tortuous (Fig. 2C). There was intratumoral accumulation of Paris Blue in minute irregular, oval and round spaces most likely containing tissue fluid with lack of lymphatic structures (Fig. 2D). Fibrous tissue around tumor foci was deprived of lymphatics. Paris Blue filled microspaces between collagen bundles (Fig. 2E).
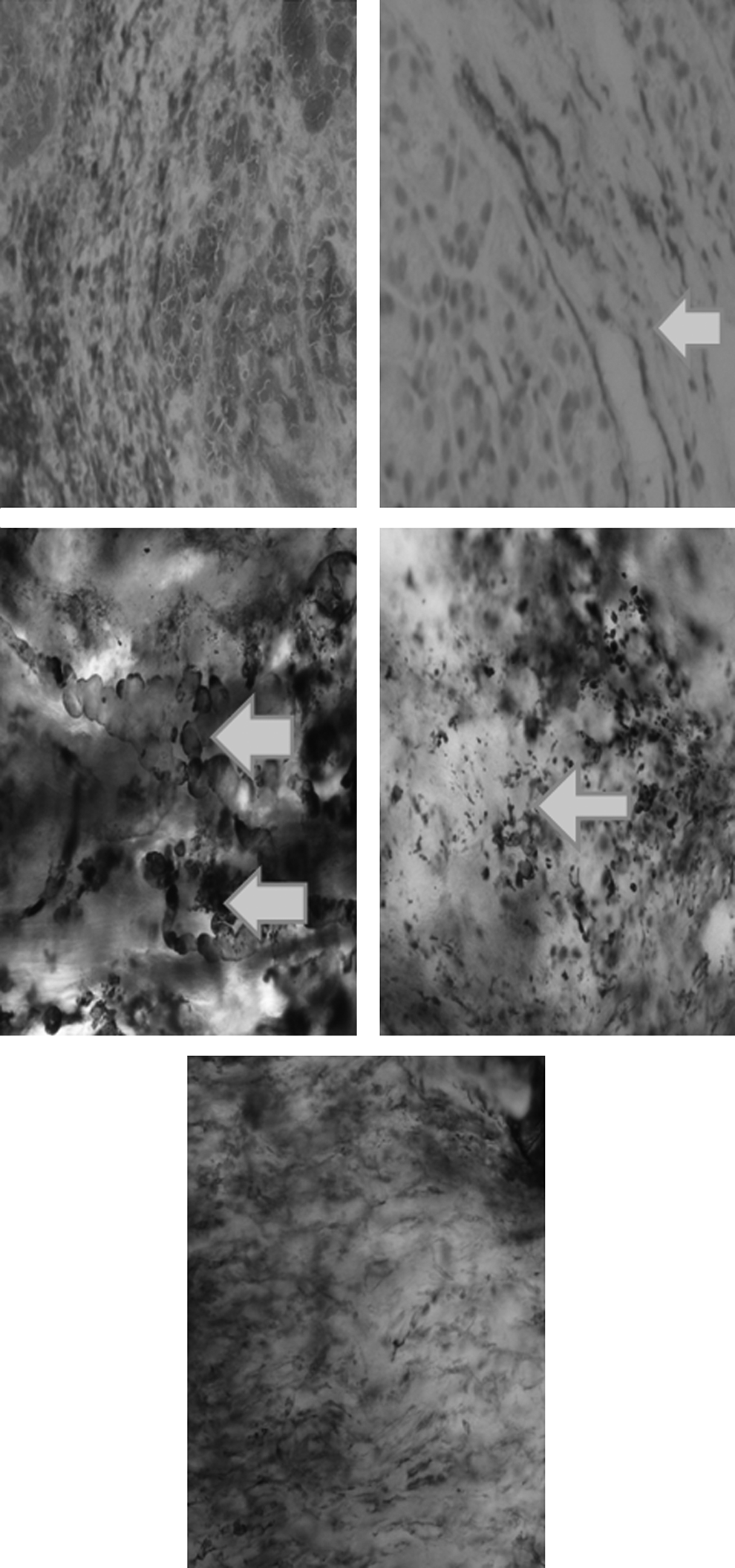
Pancreatic cancer. A. Fibrous tissue around the cancer focus. Trichrome, ×100. B. Peritumoral lymphatic (arrow), LYVE 1, ×100. C.Peritumoral lymphatics stained with Paris Blue. Multiple dilated and tortuous lymphatics (arrows). D. Intratumoral accumulation of Paris Blue in minute irregular, oval and round spaces most likely containing tissue fluid. Lack of lymphatic structures, ×100. E. Fibrous tissues around a single tumor focus. Paris Blue fills microspaces between collagen bundles, no lymphatics, ×100.
Immunohistochemistry of tumor lymphatics and blood vessels
Histological evaluation was carried out in normal (N) colon wall, tumor edge (TE) and tumor core (TC). In 20 specimens lymphatics were found in N in 100%, in TE in 70%, and in TC in 20%. Vessels in the TC regions were tiny, fragmented and had their lumen of irregular outline in most cases closed. The mean values of density ratio of lymphatics (LVD) to blood vessels (MVD) are shown in Table 2. There was also less blood vessels in TC compared with N region, however, there was a high density in TE ( Table 2).
Data are the mean values±SD of counted microvessels in 3 to 5 evaluated grids in areas of maximum vessel density. *TC vs. TE and N p<0.05.
In pancreatic cancer density of lymphatics at TE was not different from TE and in the center it was 4 times less than in N tissue. There was also fewer blood vessels (Table 3).
Data are the mean values±SD of counted microvessels in 3 to 5 evaluated grids in areas of maximum vessel density. *TC vs. TE and N p<0.05.
Cross section area of lymphatic and blood vessels
The cross section area of lymphatics in colon cancer core was 8 times lower than at TE, whereas, at the TE was higher than in normal wall. There was a high density of blood vessels at the TE (Table 4).
Data are mean number of pixels covering vessel area±SD, magnification ×200. *TC vs. TE and N p<0.05.
The cross section area of lymphatics in pancreatic cancer core was 8 times lower than at TE, whereas, at the TE was not higher than in the N wall (Table 5).
Data are mean number of pixels covering vessel area±SD, magnification ×200. *TC vs. TE and N p<0.05.
Open vs. closed lymphatic and blood vessel ratio
Evaluation of the number of open lymphatics revealed that only 40% remained open at TE and 5% at TC spots. Also a small percentage of blood vessels was found open in these areas (Table 6).
Data are mean percentage of vessels with lumen to all vessels per microscopic field. *TC vs. TE and N p<0.05, **TE vs. N p<0.05.
Counting the number of open pancreatic cancer lymphatics revealed that 40% remained open at TE and 2% at TC spots. The percentage of open blood vessels was still relatively high in these areas (Table 7).
Data are mean percentage of vessels with lumen to all vessels per microscopic field. *TC vs. TE and N p<0.05, **TE vs. N p<0.05.
Compression of lymphatic and blood vessels
The level of compression of lymphatic and blood vessels was assessed by quantification of the aspect ratio—the ratio of maximum to minimum axes of perfused vessels. An aspect ratio of 1 represents a perfect circle. The larger the aspect ratio was, the greater the amount of vessel compression (Tables 8 and 9).
Data are mean±SD, TC vs. TE and N p<0.05.
Data are mean±SD, TC vs. TE and N p<0.05.
Tumor cells in peritumoral lymphatics
Single cells of various sizes were seen occasionally in peritumoral lymphatics on stereolymphangiography in colon cancer. This was less frequently observed in pancreatic cancer cases.
Discussion
The study provided the following information: a) the TC of colon cancer contained only few lymphatics with compressed lumen but multiple minute irregular, oval or round blind spaces “lakes,” presumably containing tissue fluid; b) they were not lined with endothelial cells; c) at TE, lymphatics were visualized, however their density was lower than in a normal colon submucosa—some of them contained large tumor-like cells; d) the frequency of blood vessels at TE was highest, higher than in the TC and N colon submucosa; e) pancreatic cancer core contained sporadic fragments of compressed lymphatics and dense accumulation of round blind spaces; f) cancer foci were surrounded by dense fibrous tissue and few open tortuous lymphatics were seen close to normal tissue; and g) the frequency of blood vessels at TE was slightly higher than in the TC and N pancreatic tissue. These findings suggest that the anatomical and hydraulic conditions of the TC of both types of cancer was similar and not favorable for detached tumor cells to penetrate lymphatics.
An original finding was multiple minute spaces “lakes” in the interstitium of TC detected by Paris Blue dye injection. These spaces were presumably formed by the capillary filtrate not drained away because of lack of patent lymphatics. Since the central parts of tumors showed also compressed blood vessels, it seems unlikely that lymphatics in this region are pathways for cancer cell dissemination. Our findings corroborate similar published observations.13,14
There is still a considerable debate about the role of intratumoral vs. peritumoral lymphatic vessels in the pathology of primary human tumors. Several studies have shown that the density of lymphatic vessels located immediately adjacent to the tumor is associated with the presence of lymph node metastases. 2 Moreover, in a retrospective prognostic study, it was found that the size of peritumoral lymphatic vessels was the most significant independent factor that correlates with lymph node metastases in human malignant melanomas. 15 However, other studies showed that intratumoral but not peritumoral lymphatic vessels are vital for lymphatic metastasis.1,16 Many authors could not prove presence of intratumoral lymphangiogenesis in cases with multiple metastases.17–19 There is growing evidence that lymphatic vessels within solid tumors remain nonfunctional despite the presence of lymphangiogenic growth factor, VEGF-C. 13
Tumor-associated LVD is most frequently assessed by counting the number of immunostained vessels in tumor sections, as defined by Weidner et al. 12 Vascular “hot spots” containing lymphatic and blood microvessels are thought to represent localized areas of biological importance since they originate from tumor cell clones with the highest angiogenic potential, which will predominantly enter the circulation and give rise to vascularized metastases. We did not observe presence of hot spots in pancreatic cancer, although some could be seen in colon cancer foci. The major drawbacks of the visual MVD counting method are its inherent subjectivity and the difficulty of standardization between laboratories. Our specimens were evaluated by three independent observers. To avoid subjectivity, the image cytometry is more objective and reproducible, and moreover, it provides additional information on vessel luminal area and vessel luminal perimeter.
We measured area and number of compressed lymphatic and blood vessels using image cytometry. Ninety-five percent of lymphatics in TC and 60% at TE were obstructed. The level of compression of lymphatic vessels assessed by quantification of the aspect ratio—the ratio of maximum to minimum axes of perfused vessels— was in hot spots around 5 in both lymphatics and blood vessels but it was equal to N at TE. The situation was different at TE. Here the lymphatic and blood vessel areas were found to be higher than in Nl colon submucosa. There were no such evident differences in pancreatic cancer.
Taken together, there were very few lymphatics in the tumor tissue but numerous minor fluid “lakes” with no connection to the peritumoral lymphatics. Lining of “lakes” did not express molecular markers specific for lymphatic endothelial cells. Most open lymphatics were located adjacent to the tumor. In some of them, the transparent lumen contained single cells of a size larger than lymphocytes. It can be concluded that lack of lymphatics in the center of tumor foci, low fluid conductivity, and compression of lymphatics and blood vessels by tumor tissue and proliferating connective tissue may hamper escape of tumor cells. Multiple stagnant tissue fluid “lakes” suggest a limited drainage of intratumoral region by lymphatics. The open question remains how single cancer cells can enter lymphatics at the site with so limited lymphatic drainage.
Footnotes
Author Disclosure Statement
No competing financial interests exist.